The Vertebral Canal (see also pp. 295-298)
The diameter of the vertebral canal is greatest at the level of the first and second cervical vertebrae. It is reduced in width throughout the cervical spine, increases again in the cranial thoracic region, and becomes narrower in the caudal thoracic region.
The diameter widens again in the lumbar region to accommodate the lumbar enlargement of the cord, before gradually narrowing into the tail.Meninges: The spinal cord and nerve roots are surrounded by three meningeal layers: the tough outer fibrous dura mater, the thin arachnoid membrane lining the inner surface of the dura, and the pia mater, which is attached to the spinal cord. The dura mater adheres to the periosteum of the first two cervical vertebrae but separates thereafter (Fig. 12.8), leaving a relatively narrow epidural space that contains fat. The cerebrospinal fluid in the subarachnoid space and the epidural fat cushion the cord and allow displacement during normal movements of the spine.
The cord is the thickest in the atlas, where it measures about 1 cm. Elsewhere, except for the cervical and lumbar enlargements, it is approximately half that diameter. The cervical enlargement involves cord segments C6-T1, which contain motor neurons innervating muscles of the forelimbs and from which necessarily the nerves forming the brachial plexus arise. For the same reason, the lumbar enlargement, involving cord segments L5-S1, gives rise to the lumbosacral plexus. The craniocaudal positioning of the cord (p. 295) within the vertebral column explains the topography of its segments (Fig. 12.9). Most cervical spinal cord segments are positioned about half a vertebra, and most thoracic segments a whole vertebra, cranial to the vertebra of the same numerical designation. The caudal thoracic and cranial lumbar segments occupy vertebrae of the same designation. From the midlumbar region onward, the cord segments are markedly shorter, generally with the result that the end of the cord is positioned over the last interlumbar joint (Figs.
12.9 and 8.56B). The cervical and lumbosacral enlargements lie in the sixth and seventh cervical vertebrae and the fourth and fifth lumbar vertebrae, respectively. The relative cranial position of the lumbar spinal cord segments is less marked in small dogs, in which the cord may reach the sacrum; in large dogs it may end at L4. The sacral canal contains only spinal nerves and the dural sheath, which extends about 2 cm beyond the caudal termination of the spinal cord. The termination of the cord is said to be variable in cats: all levels from the caudal border of L7 to the caudal border of S3 have been given by different writers. Some of this uncertainty may be due to individual and breed variation, but probably the more cranial limit is likely to be nearer the mark in adults, the more caudal one in young kittens.The cauda equina is the bundle of spinal nerves remaining in the vertebral canal after the termination of the spinal cord. It consists of the spinal nerves L6-Cd5 and includes those that form the sciatic (L6-S1) and pudendal (S2-S3) nerves. Each nerve exits the vertebral canal from its respective intervertebral foramen. Clinically, it may be trapped at the foramen by herniation of the adjacent disk. In the sacrum, the ventral branches of the first two sacral nerves emerge through foramina in the floor of the sacral canal. The "cauda equina syndrome," an important cause of neurologic dysfunction and pain, is a result of entrapment of one or more of the nerves of the cauda equina. The symptoms may include lower back pain, atrophy of muscles innervated by the sciatic nerve, paresis, tail weakness, incontinence of bladder and bowel, and paresthesias (abnormal sensation, possibly provoking self-mutilation). Entrapment may also be caused by bone pathology (e.g., osteochondrosis of the first sacral vertebra) or by secondary hypertrophy of the ligaments.
Puncture of the subarachnoid space is performed for the collection of cerebrospinal fluid and for the injection of contrast media for myelography. Myelograms are performed less often with the availability of more sophisticated imaging modalities such as computed tomography and magnetic resonance imaging, but the principle is explained here.
Contrast material outlines the subarachnoid space and may thus reveal cord lesions that are not apparent in survey radiographs; a myelogram is especially useful in revealing multiple lesions or when survey radiographs do not match the clinical signs. Recommended sites for puncture are the atlanto-occipital space and the lumbar spine at levels L4-L5 and L5-L6. Atlanto-occipital punctures enter the cerebromedullary cistern of the subarachnoid space (see Fig. 12.6). In this procedure, the neck is strongly ventro-flexed, and an entry is made midway between the external occipital protuberance and the cranial tip of the spinous process of the axis. These landmarks are more easily identified before flexion (Fig. 12.3A). The lumbar puncture (see Fig. 12.7) is also used. Surprisingly, accidental penetration of the spinal cord has minimal clinical effect although it provokes a histologic reaction.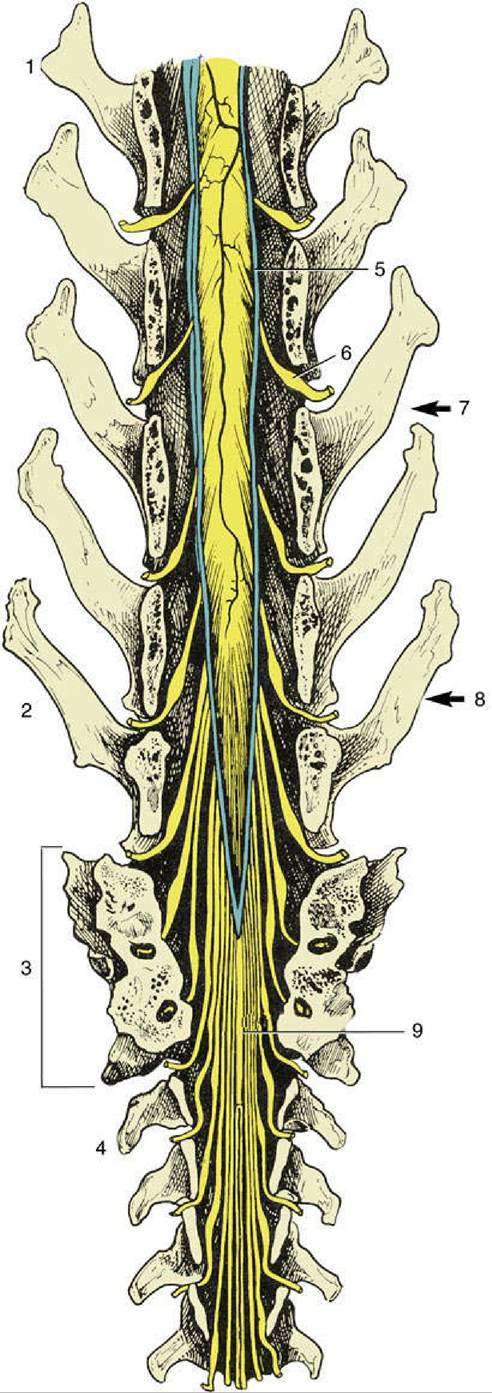
FIG. 12.9 Caudal end of the canine spinal cord in situ, dorsal view. 1, Third lumbar vertebra; 2, last lumbar vertebra (L7); 3, sacrum; 4, first caudal vertebra; 5, dura mater; 6, dorsal root ganglion; 7, approximate level of L7 cord segment; 8, end of spinal cord; 9, cauda equina.
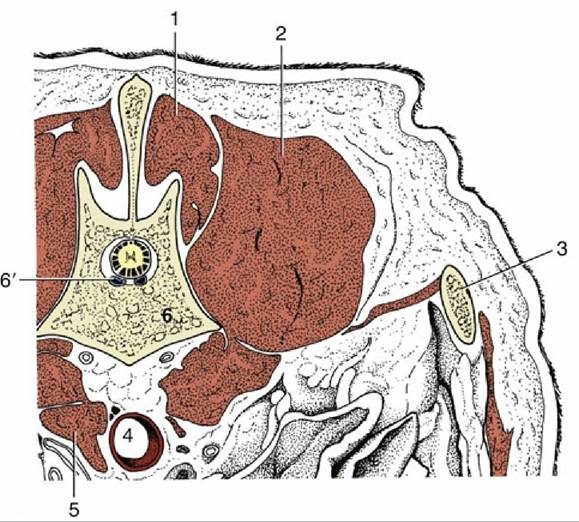
FIG. 12.10 Transverse section of the back of a dog at the level of the first lumbar vertebra. 1, Multifidus and spinalis muscles (mm.); 2, longissimus and iliocostalis mm.; 3, last rib; 4, aorta; 5, right crus of diaphragm; 6, first lumbar vertebra; 6', internal vertebral venous plexus.
Epidural anesthetics are administered at the lumbosacral or the sacrocaudal intervertebral space. The lumbosacral space is located a little in front of the cranial dorsal iliac spines (see Fig. 12.7). A misleading impression of its size may be obtained by failure to appreciate that a last lumbar spinous process is relatively short and does not approach as closely to the skin as that of the preceding vertebra.
The sacrocaudal space is smaller, and the defining features of the vertebrae less obvious, but the space is much closer to the skin.As in other species, the internal vertebral venous plexus consists of two longitudinal valveless veins on the floor of the vertebral canal, where they are embedded in epidural fat (Fig. 12.10/6'; p. 295). The left and right veins often anastomose at different levels; some connections pass below the dorsal longitudinal ligament, and others pass through the vertebral bodies. The plexus receives blood from the spinal cord and vertebrae; it is linked to extensive but less regular external networks and to adjacent great veins (caudal vena cava, azygos vein) by intervertebral veins. These veins, which may be double and triple, cushion the spinal nerves where they leave the vertebral canal.
At the foramen magnum the veins of the internal plexus are continuous with the right and left basilar sinuses that lead from the system of venous sinuses on the floor of the cranial cavity.
Like many other mammals, the dog makes use of its tail to maintain balance when executing various energetic maneuvers, but the tail is also used as a means of communication. Sometimes it is necessary to amputate part of the tail after an injury. A feature relevant to the operation includes the presence of the median caudal artery running below the vertebral bodies. The artery is partly shielded by processes of bone that take the form of separate V-shaped hemal bones located below the fourth to sixth tail vertebrae and hemal processes projecting from the ventral aspect of the more distal vertebral bodies. Obviously, amputation is simplest at the level of an intervertebral disk. It may be mentioned that these disks are not immune from the degenerative processes described earlier.