GLOMERULAR FILTRATION
1. What are the two capillary beds that perfuse the nephrons? Which one resembles the arterial end of a muscle capillary and which one resembles the venous end?
2. Study the capillary dynamics associated with filtration at the glomerulus.
3. How does efferent arteriolar constriction increase the FF?
4. What are the factors associated with autoregulation of RBF and GFR?
The kidneys have the Iunctional counterpart of two capillary beds, represented by the glomeruli and the peritubular capillaries. The glomeruli are considered to be a high-pressure system (high hydrostatic pressure (HP), favoring filtration) and the peritubular capillaries, which are perfused with blood coming from the glomerular capillary bed, are considered to be a low-pressure system (low HP, favoring reabsorption). As such, the glomeruli are similar to the arterial end of a typical muscle capillary and the peritubular capillaries are similar to the venous end (see Chapter 9). The fenestrated capillary endothelium of the glomerulus is markedly more porous than the muscle capillary endothelium facilitating the movement of plasma and solutes out of the glomerulus and into Bowman’s capsule whilst retaining cellular components, macromolecules, and the majority of proteins in the blood.
Dynamics of Filtration
Dr Michael Kimber, PhD
With each pass through the kidneys, approximately 25% of plasma is filtered out of the glomerulus to form a filtrate delivered to the nephron for selective reabsorption. The barriers to filtration from glomerular capillaries to the capsular space (the glomerular membrane) are the fenestrated capillary endothelium basement membrane and the filtration slit diaphragm (see Figure 11-11). The forces driving the movement of plasma across this filtration barrier are the same balance of hydrostatic and osmotic pressures as those governing capillary dynamics elsewhere (see Chapter 9), with minor differences as illustrated in Figure 11-13.
Capillary hydrostatic pressure (Pc, favors filtration) is high due to left ventricular contraction and may be modulated further by afferent and efferent arteriole tone (see later sections). The hydrostatic pressure exerted by fluid in the Bowman’s space (Pbs) is of lesser magnitude and is positive, that is, opposes filtration. This is unlike interstitial fluid hydrostatic pressure (Pjf) seen in extraglomerular capillary beds, which has a negative pressure (vacuum). The plasma colloidal osmotic pressure (πc) opposes filtration and is generated by the presence of protein in glomerular capillaries, which are prevented from leaving because of the filtration barrier. Some leak of protein does occur to generate a Bowman’s space colloid osmotic pressure (∏bs) but this is negligible under normal circumstances. The overall net filtration pressure at glomeruli is comparable to other capillary beds (e.g., muscle) but plasma movement out of glomerular capillaries is significantly higher. This is accounted for by the more porous fenestrated capillary endothelium and the greater surface area available for filtration presented by the convoluted capillary structure of the glomerulus.
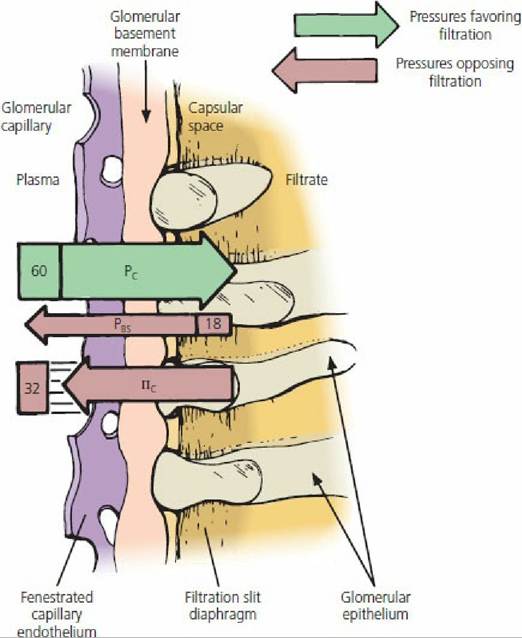
■ FIGURE 11-13 Dynamics of glomerular filtration in mammals. Bowman’s capsule is separated from the glomerulus by a glomerular membrane, through which filtration occurs. The extent of filtration is determined by the difference between the pressures favoring filtration and those opposing filtration. In this illustration, filtration occurs because 60 - (32 + 18) = 10 mm Hg. Values greater than or less than 10 mm Hg would correlate with more or less filtration, respectively. Pressure values (60, 32, 18) are in mm Hg. Pc is capillary hydrostatic pressure; Pbs is Bowman’s space hydrostatic pressure; and πc is colloidal osmotic pressure.
Filtration Factors
The GFR can be varied by changing the diameter of the afferent or efferent arterioles.
Dilatation of the afferent arteriole increases the blood flow to the glomerulus, which in turn increases the HP and potential for filtration. Constriction of the efferent arteriole increases the glomerular HP, just as blockage of a vein increases the HP in capillaries behind it. Even though RBF to the glomerulus is reduced because of the decreased outflow caused by efferent arteriole constriction, the GFR is maintained (because of the greater HP) and this allows for a continued FF.For any given molecular size, positively charged molecules are more readily filtered than negatively charged molecules. This happens because there are negatively charged (anionic) sites (mostly proteoglycans) in the glomerular basement membrane that repel similarly charged molecules. Accordingly, plasma albumin molecules are relatively restricted from filtration (might not be excluded altogether) because, coupled with their large molecular size, they are polyanionic in the physiologic pH range. In kidney disease, in which poor perfusion may become a factor, the electrostatic charge of the glomerular membrane can change, and molecules previously restricted from filtration can be filtered and gain entrance to the capsular space.
Autoregulation
A feedback mechanism, known as the tubuloglomerular feedback mechanism, performs the function of autoregulation. It has two components that act together to control GFR: (1) an afferent arteriolar feedback mechanism and (2) an efferent arteriolar feedback mechanism. Macula densa cells sense changes in volume delivery to the distal tubules. Decreased GFR slows the flowrate in the loop of Henle that allows for increased reabsorption of sodium and chloride ions in the ascending limb of the loop of Henle, thereby decreasing the concentration of sodium chloride at the macula densa cells. This results in a signal from the macula densa decreasing resistance to blood flow in the afferent arterioles, which raises glomerular HP, helping to return GFR to normal.
The signal from the macula densa also increases release of renin from the JG cells of the afferent and efferent arterioles (major storage sites for renin). Renin, an enzyme, increases the formation of angiotensin I, which is converted to angiotensin II by angiotensin converting enzyme (ACE).Angiotensin II constricts the efferent arterioles, thereby increasing glomerular HP and assisting the return of GFR toward normal. The production of angiotensin II continues because of the conversion of plasma angiotensinogen (produced in the liver) to angiotensin I by renin and its subsequent conversion to angiotensin II by ACE (Figure 11-14). Although ACE is derived mainly in the capillary endothelium of the lung, because of its vascularity it is also derived in the kidney endothelium and other organ beds.
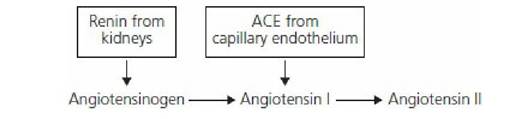
■ FIGURE 11-14 The conversion of angiotensinogen to angiotensin II. Plasma angiotensinogen is produced in the liver. It is converted to angiotensin I by renin released from the juxtaglomerular cells of the afferent and efferent arterioles. Angiotensin I is converted to angiotensin II by angiotensin converting enzyme (ACE) derived from capillary endothelium.
Next to vasopressin, angiotensin II is the second most potent vasoconstrictor produced in the body. It is rapidly destroyed in the peripheral capillary beds by a number of enzymes called angiotensinases. Although not related to autoregulation, angiotensin II stimulates the secretion of aldosterone, which causes reabsorption of [Na+]. This becomes a factor in (ECF) volume regulation.
■
More on the topic GLOMERULAR FILTRATION:
- Renal Function and Hyperthyroidism
- Tubular Necrosis
- Diagnosis
- Blood Urea Nitrogen
- Amyloidosis
- Creatinine
- Acute Renal Failure
- PATHOPHYSIOLOGIC DERANGEMENTS OCCURRING WITH HEPATIC DISEASE
- Perinatal Asphyxia Syndrome
- CLINICAL ANATOMY AND PHYSIOLOGY OF PAEDIATRIC PATIENTS