Acute Abdomen in Ruminants
David Francoz • GiUes Fecteau •
Andre Desrochers • Sylvain Nichols
Abdominal emergencies in ruminants are both a therapeutic and a diagnostic challenge for veterinary practitioners.
Some of them necessitate immediate surgical treatment, and others can be treated medically (Fig. 32.125). They are associated with numerous conditions that affect the abdominal cavity and can also be mimicked by diseases of extraabdominal origin (Fig. 32.126).Different questions should be addressed during management of an acute abdomen in ruminants: Where does the pain originate? Is it a medical or surgical problem? Is it an urgent or nonurgent problem? Is medical treatment indicated before surgery? What is the likelihood for survival and productivity? To answer these questions, the clinician should use a systematic approach that is based on adequate signalment and history, complete physical examination, and judicious choice of ancillary

FIG. 32.123 Transrectal sonogram of a left renal cyst in an Holstein dairy cow. This was an incidental finding. The cyst (star) is surrounded by the hyperechoic renal sinus and hypoechoic pyramid (P). Image obtained transrectally with a linear 8-MHz probe (maximal depth, 8 cm).
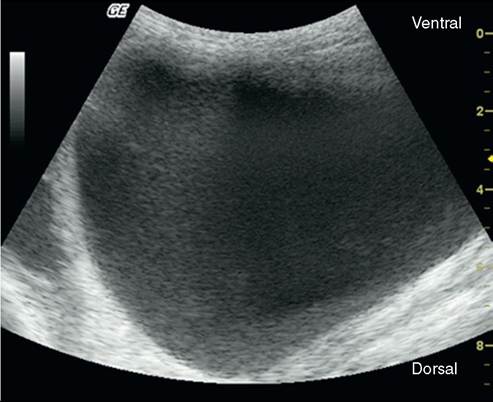
FIG. 32.124 Distended urinary bladder in a 4-month-old Boer buck with urolithiasis. The distended urinary bladder is a circular structure with anechoic content. This finding is compatible with the absence of major rupture of the urinary bladder. Images obtained at the ventral part of the abdomen with a sectorial 3.2-MHz probe (maximal depth, 10 cm).
tests. Precise information is not yet available for accurately determining the prognosis about the outcome of an acute abdomen in ruminants.
In most cases, prognosis should be based on past experiences of other clinicians as well as one's own experience.Even though a precise diagnosis facilitates the institution of appropriate treatment and helps better predict outcome, emphasis should not be placed solely on the diagnosis. In addition, contrary to other species, the cost and risk associated with standing laparotomy are minor in cattle. Consequently, it could be more economical to directly perform a laparotomy and avoid additional diagnostic tests and procedures.
Abdominal Pain
Abdominal pain may be a consequence of excessive distention of a hollow viscus (excessive intestinal distention), spasms of intestinal smooth muscles, stretching of the mesenteric supporting structure, intestinal ischemia, or chemical irritation of the visceral or parietal peritoneum.1 Abdominal pain is classified into two main categories: visceral pain (hollow viscera and solid organs) and parietal pain (parietal peritoneum, abdominal muscles, rib cage).
Pain sensation from the parietal peritoneum travels through the peripheral spinal nerves and usually localizes over the affected area.1 Because parietal pain is exacerbated by pressure and tension modification, affected patients are reluctant to move and have tonic reflex contractions of the abdominal muscles.2 No active clinical signs of colic are present. This scenario is typically observed in cases of peritonitis. In addition to being reluctant the move, the animal has a splinted abdomen, and external palpation produces specific responses,3 such as a positive result of a xyphoid grunt test or not dipping the back when pinched over the withers.
Some pain fiber endings are located in the submucosa and muscle layers of hollow viscera (intestines, bladder) and in the capsule of solid organs (kidneys, liver). Consequently, distention, forceful contraction, or traction produces pain in a hollow viscus. Capsule stretching creates pain in solid organs.
Visceral pain is typically recognized by active manifestations of colic: kicking at the abdomen; treading with the rear feet; lying down, standing, and stretching out and grinding the teeth. Affected goats may also vocalize. Affected animals are anxious and have an apprehensive attitude. Contrary to parietal pain, visceral pain is transmitted via sensory fibers in the autonomic nerves.1 Visceral pain is often diffuse and difficult to localize.1A Concise but Precise Evaluation of the Animal
An animal with acute abdomen may need immediate medical assistance. Therefore the clinician should identify life-threatening problems and take appropriate action rapidly. Acute abdominal emergencies are often associated with either hypovolemic or septic shock, which should be treated promptly. Hypovolemic shock is characterized by increased heart rate, pale mucous membranes, slow capillary refill time, and dehydration. Increased heart rate and dehydration are also observed in case of septic shock, but mucous membranes are hyperemic or bluish in color, and scleral vessels are congested and dark. Intensive fluid therapy is the treatment of choice for both hypovolemic and septic shock. Pain control may also be necessary to allow a more complete physical evaluation (see Medical and Supportive Treatment, Fluid Therap, and Control of Pain and Inflammation sections). However, documentation of a complete history and meticulous physical examination should be performed before emergency medical therapy if the patient is stable.
HISTORY. History documentation should be focused on the identification of risk factors of specific conditions, as well as the description of pain and associated clinical signs.
Signalment may identify an animal at higher risk of particular diseases. Age, sex, breed, and production stage are important parameters to consider in establishing the differential diagnosis. For example, abomasal volvulus develops more frequently in dairy cows than in beef cattle.4,5 Similarly, uterine torsions are essentially observed at the time of parturition or in the last trimester.
Colic in a wether or a buck goat should be considered a result of urolithiasis until proven otherwise. Specific nutrition programs and management systems have also been associated with specific conditions such as hemorrhagic bowel syndrome.6 Paralytic ileus associated with hypocalcemia is reported to occur during estrus.7 Previous history of surgery can be associated with the development of adhesions and colic. Recent calving and obstetric manipulations may cause a full-thickness uterine tear and subsequent peritonitis.Description of the clinical signs observed by the owner and the chronologic sequence of events are of particular interest.
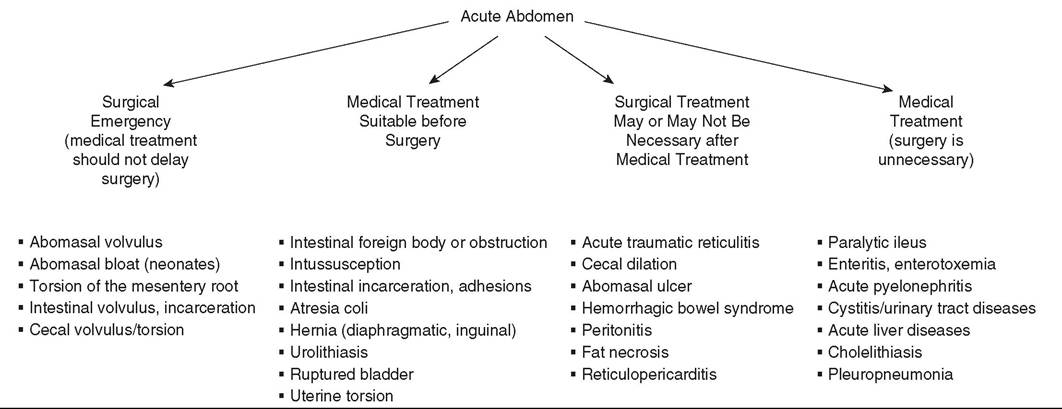
FIG. 32.125 Classification of abdominal causes of acute abdomen according to the need for surgical exploration or medical treatment.
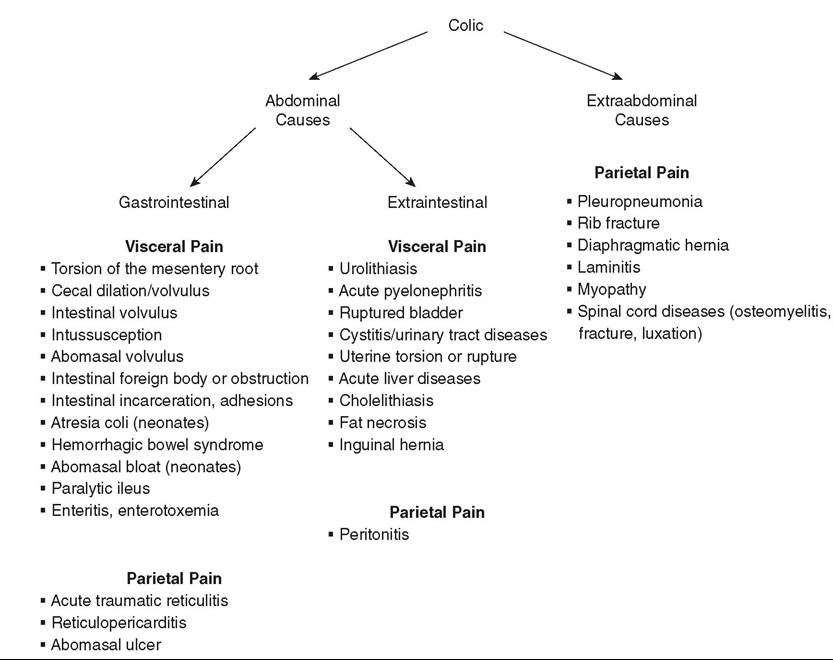
FIG. 32.126 Causes of colic (abdominal pain) in ruminants.
Abdominal pain is an important criterion in deciding whether surgery is necessary. Severe colic is classically associated with surgical intestinal conditions,3,8 although some animals with severe jejunal distention secondary to acute enteritis may have a similar clinical presentation.9 Intussusception in cattle is characterized by an acute onset of anorexia, decreased fecal output (often with dark feces containing blood) and milk production, and colic. However, even though the abdominal pain eventually becomes less severe, the depression progresses.3,10 Torsion of the mesenteric root has an acute onset with severe colic and rapid deterioration.3,11,12 Previous treatments, especially those that can modify clinical signs or the interpretation of laboratory results, should also be noted. Administration of analgesics such as NSAIDs may partially control abdominal pain, attenuate signs of colic, and decrease the heart rate.
Identification of associated clinical signs may help identify not only digestive but also nondigestive causes of abdominal pain. Fecal output, consistency, and appearance are relevant information. Stranguria manifested by unsuccessful micturition efforts is associated with urolithiasis. Pleuritis, pleuropneumonia, or rib fractures may mimic abdominal pain.
COMPLETE PHYSICAL EXAMINATION. A thorough and complete physical examination is the most important step in evaluating an acute abdomen.
Evaluation of Vital Parameters. Assessment of cardiovascular status (heart rate, mucous membranes, capillary refill time, and dehydration) is essential in the evaluation of an animal with an acute abdomen and is part of the rapid initial evaluation of the animal. Determination of rectal temperature, pulse or heart rate, and respiratory rate (TPR) should always be performed first because manipulations during the physical examination of an abdominal emergency can elicit pain and modify the heart rate.
The TPR and amount of pain exhibited may also be used to monitor the evolution of the condition and the response to the initiated treatments, as well as prognostic factors. Normal to moderately elevated heart rate and adequate hydration status are considered good prognostic indicators in abomasal volvulus.13 Combination of heart rate and lactate measurements has been reported to improve the ability to predict negative outcome of right-sided abomasal disorders.14
Once vital parameters have been evaluated and the animal appears hemodynamically stable, a thorough complete physical examination of all body systems is performed.
Visual Examination. The animal's abdominal profile or silhouette should be observed from the rear and both sides to detect and characterize abdominal distention. Bilateral ventral distention is associated with small intestine disorders, whereas distention in the right paralumbar fossa is associated with cecal and colon disorders.
In cases of abomasal volvulus, the distended abomasum can be observed caudal to the last rib in the right paralumbar fossa. Gas in the rumen causes distention of the upper left abdomen, whereas some forms of chronic indigestion have a “papple” shape (pear on the right and apple on left). Lateral views of the abdomen help determine whether the distention arises primarily from the paralumbar fossa or extends cranially under the ribs. An affected animal may arch the back in cases of cranial abdominal pain, sole abscesses, or laminitis (sore feet).Extraabdominal Examination. Examination of the thorax (pleuropneumonia, rib fractures) and the musculoskeletal system (laminitis, myopathy) are important in ruling out diseases that mimic abdominal pain.
Abdominal Examination. Abdominal examination is performed by auscultation, percussion, ballottement, and succussion of the abdomen. Pings are sounds of tympanic resonance caused by a gas-fluid interface in a distended organ and can be detected by simultaneous auscultation and percussion. Because rectal palpation may create an area of increased resonance on the right dorsal part of the abdomen, detection of pings should be performed before rectal palpation. On the right side of the abdomen, many organs may be responsible for pings. Determining the location, pitch characteristics, and variability of the ping is essential for establishing a differential and precise diagnosis. Pings localized from the thirteenth rib cranially to the ninth rib are typical of abomasal volvulus or rightward displacement of the abomasum.3 Cecal dilation or volvulus causes a ping in the right paralumbar fossa and caudal quadrant,3 often extending to the hip. Abomasal volvulus is more likely to cause a high-pitched ping, whereas animals with peritonitis may have a bilateral low-pitched ping in the upper paralumbar fossa. In normal animals, a monotone pinging area of 15 to 20 cm centered just under the last rib corresponds to gas in the spiral colon. Moving or constantly contracting viscera, such as gas in the descending duodenum or proximal colon, produce pings of changing pitch. For this particular reason, it is important to auscultate and percuss for a certain period of time to notice ping variation.
On the left side, pings are principally associated with left abomasal displacement, ruminal collapse, and pneumoperitoneum. Left abomasal displacement typically causes pings dorsally from the eighth to the thirteenth ribs. Pings associated with gas in the rumen, ruminal collapse, and pneumoperitoneum are localized dorsally in the left paralumbar fossa and extend cranially to the eleventh rib. Simultaneous auscultation and ballottement (succussion) of the abdomen may detect fluid-filled viscus with an interface of gas such as the rumen or the abomasum. The location of the fluid splashing sounds on auscultation-succussion may help confirm and differentiate among auscultation-percussion findings. Tense abdominal muscles, secondary to parietal peritoneum inflammation (parietal pain), may also be detected during succussion. Auscultation of ruminal contractions is also of importance. The number of rumen contractions should be counted and characterized over at least a 2-minute period. Three complete contractions per 2 minutes are considered normal. Incomplete and frequent contractions (>5 per 2 minutes) and complete absence of contraction for 2 minutes are abnormal. After initial treatment. the rumen auscultation should be repeated to evaluate the improvement.
Identincation or Abdominal Pain. Differentiation between visceral and parietal pain. as well as pain localization. should be attempted in order to investigate the cause. However, the task is often difficult in animals such as cattle whose behavior in response to pain is unpredictable.
Cranial peritonitis, secondary to traumatic reticuloperitonitis (TRP) or abomasal ulcers, is a common cause of parietal abdominal pain. Affected cattle are reluctant to move; they stand with the elbows abducted and an arched back.3 During examination, bruxism (grinding of the teeth) may be present.3 Pain can be elicited by pinching over the withers or applying forceful movement with the knee or upward pressure with a bar or pole over the xyphoid area or anterior abdomen. In response to pain, an animal may grunt or kick and be reluctant to dip the back when the withers is pinched.3 Sensitivity of this test may be increased by simultaneous auscultation of the trachea to better hear the subtle grunt.
As mentioned previously, the visceral pain is more diffuse and associated with active manifestations of colic.
Rectal Palpation. Rectal abdominal palpation of cattle is an essential part of the physical examination for acute abdomen. However, the size of the abdomen limits the systems or organs that can be palpated.
Cecal disorders are clearly diagnosed by rectal palpation. A firm mass palpated in multiple, dilated, turgid small intestine loops is a typical finding of intussusception10 or hemorrhagic bowel syndrome.6 Adhesions between the kidneys and the rumen, the intestinal convolutions, and decreased rectal mobility in the posterior abdomen are characteristics of a chronic peritonitis. Uterine wall integrity may be evaluated during rectal palpation, although examination per vagina may be necessary to confirm a full-thickness laceration in an early postpartum cow. In feedlot steers with urolithiasis, rectal palpation reveals a pulsatile pelvic urethra and a distended bladder. In cases of pyelonephritis, enlargement of one or both ureters may be palpated. Normally, only the left kidney can be palpated rectally: If infected, it will be painful to the touch and larger, and lobulation may become less obvious. Diseased right kidneys are exceptionally reached rectally especially if the animal is hydronephrotic. In small ruminants, urolithiasis is manifested by pulsations in the pelvic urethra that may be palpated by digital rectal examination. Bladder distention or kidney enlargement can be detected by deep abdominal palpation, and vocalization will be elicited during palpation of the distended bladder.
Fecal Output and Appearance. Presence and macroscopic appearance of feces can be evaluated during rectal palpation. Decreased or absence of feces is principally associated with intestinal stasis or obstruction, which may occur secondary to a direct mechanical obstruction (necessitating surgical treatment) or to gastrointestinal ileus (necessitating only medical treatment). However, feces may be present in the first few days after an intestinal obstruction.
ANCILLARY TESTS
Packed Cell Volume and Total Solids. Shock, sepsis, and toxemia cause hemoconcentration and dehydration and are associated with an increase in total solids. On the other hand, increased PCV and decreased total solids are observed during the formation of a third compartment filled with a protein-rich fluid, as in generalized peritonitis.15 In one study, total protein concentration was significantly lower in cows with septic peritonitis than in cows suffering from nonseptic peritonitis.16
Blood Gas Analysis and Electrolytes. Blood gas analysis and electrolyte measurement results are helpful in the institution and monitoring of fluid therapy. Most adult ruminants with acute abdominal diseases suffer from metabolic alkalosis.17 Metabolic alkalosis is often associated with abomasal volvulus, intussusception, cecal disorders, abomasal ulcers, peritonitis, renal diseases, and reticuloperitonitis.17 Hypochloremia and hypokalemia are frequently combined with metabolic alkalosis.18 Metabolic acidosis may be observed if urinary tract disease, small intestinal strangulation or obstruction, or enteritis with 17
severe diarrhea is present.17
Some parameters could also be used as prognostic indicators. Serum chloride concentration, anion gap, and base excess have been proposed as preoperative prognostic indicators in dairy cattle suffering from abomasal volvulus. Poor short-term prognosis was associated with serum chloride concentrations lower than 79 mEq/L,19 base excess values of -0.1 or less,20 and anion gap values of more than 30 mEq/L.21 However, a prospective study on the outcome of abomasal volvulus demonstrated that serum base excess and anion gap values did not differ between productive and nonproductive animals.13 In that study, serum chloride concentration was significantly lower in nonproductive animals, but the prognostic test yielded numerous false-negative results.13
Blood Lactate Concentration. Blood lactate concentration is frequently used to assess a compromised cardiovascular or respiratory system, to monitor the response to treatment, and to establish a prognosis for survival. Portable analyzers are available for the measurement of L-lactate, and so this diagnostic test is easily doable at the farm. In cattle, blood lactate concentrations have been reported as a predictor of uterine torsion22 and abomasal disorders.14,23-26 Blood L-lactate concentrations exceeding 6.5 mmol/L before correction of uterine torsion22 or exceeding 6 mmol/L before surgery for right abomasal disorders14 were associated with a poor prognosis. In the author's clinics, an early measurement (before any treatment) and a follow-up measurement after initial therapy (IV fluids, NSAIDs, or other) are performed. The author and colleagues have found that an increase in blood lactate or a very marginal reduction in blood lactate, despite aggressive therapy, indicates that surgery is needed or the prognosis is poor. However, in one study, short-term change (preoperative and postoperative values) in blood L-lactate concentrations did not appear to be a useful prognostic indicator.23
Serum Biochemistry Profile. Evaluation of specific enzyme activity or markers (e.g., hepatic enzymes, BUN, and creatinine) along with physical examination and other ancillary tests may be useful in establishing a diagnosis and assessing progress.
Complete Blood Cell Count and Differential. Hematologic findings are rarely specific to a condition and reflect the underlying inflammatory process. In most cases a minimal to moderate inflammatory process characterized by a neutrophilic leukocytosis is observed. Hematologic findings may also provide information about the acuteness of the disease and the severity of associated sepsis and toxemia. Severe sepsis is associated with neutropenia, degenerative left shift, toxic changes in neutrophil structure, and lymphopenia. Hematologic study is also an important ancillary test for monitoring the response to treatment.
Fibrinogen. In ruminants, increased fibrinogen concentration is an early indicator of inflammation. Studies in cattle have demonstrated that fibrinogen concentration may increase within 1 to 2 days after induction of inflammatory conditions. Normal fibrinogen concentration despite severe visceral involvement should be observed only in peracute cases (within a few hours; e.g., torsion of the root of the mesentery). Moderate to marked increased fibrinogen concentration is also the signature of chronic active localized inflammatory conditions such as reticuloperitonitis, liver abscesses, and pyelonephritis.
Urinalysis. Urinalysis is helpful in differentiating between colic of urogenital origin from gastrointestinal disorders. Urinalysis can be performed rapidly with a urinary dipstick (Chemstrip 9, Roche Diagnostics Corporation, Indianapolis, Ind.) and gross morphologic examination. Renal diseases are associated with proteinuria (>1+), glucosuria, and positive blood reaction. In cases of acute urethral obstruction, hematuria and proteinuria are consistently observed. Determination of urinary specific gravity before fluid replacement may help characterize azotemia.
Abdominocentesis. Abdominocentesis is considered an essential ancillary test in the approach to acute abdomen in many species,9,27 including cattle.3 Because of the ability of cattle to wall off and localize infections in the abdomen, a four-quadrant method of abdominocentesis is suggested by some authors.3 Ultrasonography can be used to find abnormal fluid location or quantity, which improves the precision of determining the abdominocentesis site. Fluid can be evaluated macroscopically for color, volume, odor, and turbidity. Normal and changes values are reported in the Peritonitis in Ruminants section of this chapter.
Different parameters may be evaluated in peritoneal fluid. Lactate, D-dimer, glucose, and ALP concentrations and pH of the peritoneal fluid have been reported to be indicators of intestinal ischemia and peritonitis in horses.28,29 In one cattle study, decrease in glucose concentration in peritoneal fluid was a sensitive and specific marker of septic peritonitis.16 D-Dimer level is also elevated in cases of ischemic and inflammatory abdominal conditions.16,24 L-Lactate measurement could also be a useful diagnostic tool for the evaluation of various abdominal ischemic conditions in cattle.24
Diagnostic Imaging
Ultrasonography. Ultrasonography is a very helpful diagnostic tool for the management of acute abdomen. It helps in identifying the structures involved, the extension of the lesions, and the presence of abdominal fluid, as well as in the monitoring of the cases. With advances in multifrequency abdominal transducers, ultrasonography is used more frequently in ruminant medicine. More detailed information this type of imaging is available in the Ultrasonography of the Ruminant Abdomen section.
Radiography. Radiographic images in adult cattle are obtained with powerful machines available only in referral centers. They are among the most helpful ancillary examinations for the diagnosis of reticuloperitonitis.30,31,32 Abdominal radiographs have been used for the diagnosis of intestinal atresia and intussusception in calves.3
A lateral view of the abdomen of small ruminants may help for the diagnosis of urolithiasis because stones in the urethra or in the bladder may be detected.
Medical or Surgical Decision
A differential diagnosis and a decision for surgical or medical treatment should be established on the basis of clinical signs and ancillary tests results (see Fig. 32.126). If a definitive diagnosis is made, specific treatment can be instituted. When a definitive diagnosis cannot be established, attempts should be made to differentiate surgical and medical cases (see Fig. 32.125). Every animals with elevated heart rate, with organ distention found on rectal palpation, and that is producing little to no feces are surgical candidates even if a definitive diagnosis cannot be established. Intestinal obstructions necessitate immediate surgery. A mechanical obstruction may be suspected when there is a suspicion of intestinal or cecal torsion on rectal examination, pings indicating a right abomasal displacement or volvulus, peritoneal fluid indicating bowel devitalization, severe active colic, or rapid deterioration in the animal's condition.8 If an intestinal mechanical obstruction is not suspected during the first examination, exploratory surgery may be delayed for up to 36 hours.33 However, frequent monitoring should be performed and appropriate medical treatment provided to the animal.
SURGERY. Most abdominal surgery in adult cattle is performed with the animal standing and with local or regional anesthesia. Sedation may be necessary in some cases, but the risk of lying down during surgery have to be considered. Cattle can tolerate intestinal resection and anastomosis standing if adequate local anesthesia and systemic analgesia are provided. However, some animals are reluctant to stand because of the primary condition or as a result of electrolyte imbalance. Any traction on the mesentery root is painful enough to make an animal go down during the procedure. Surgery should be performed with the animal in recumbency if it is in extreme pain or weak and likely to lie down. Because a right paralumbar fossa celiotomy provides the best exposure to the intestinal tract, left lateral or sternal recumbency should be favored. Other than the general status of the animal, the suspected affected organ, presence of aggressive behavior, surgeon preferences, and facilities should be considered in the choice of performing the surgery with the animal standing or in recumbency. If the animal is dehydrated or manifests signs of shock, preoperative fluid therapy and analgesics are recommended. For the prevention of surgical infection, appropriate preoperative antibiotic administration is also recommended.
MEDICAL AND SUPPORTIVE TREATMENT. The goal of therapy in an animal with acute abdomen is to initially correct the hemodynamic and metabolic imbalances associated with hypovolemic or septic shock, to control pain, and to correct or treat the primary cause of the disease, when identified. Consequently, medical treatment often includes fluid therapy, NSAIDs, and antimicrobial drugs.
Fluid Therapy. Crystalloid solutions (0.9% NaCl, Ringer's solution) are indicated initially to replenish fluid loss and improve the circulating blood volume. To resuscitate critically ill neonatal patients, recommended intravenous fluid administration rates of isoosmotic crystalloid solution are 80 to 90 mL/ kg of body weight per hour.34 However, such rates are difficult to achieve through a catheter in adult ruminants. The maximal flow rate usually achieved through a catheter (14G catheter) in an adult cow is 15 to 20 mL/kg/h. Studies demonstrated that perfusion rates of 40 and 80 mL of an isoosmotic crystalloid solution per kilogram of body weight per hour can be used safely in adult ruminants and dehydrated calves, respectively.35,36,37 If the animal is not critically ill, fluid and electrolyte deficits should be corrected over 2 to 8 hours.
Hypertonic solutions (7.2% or 7.5% NaCl) are also an alternative. Intravenous administration of hypertonic saline provides rapid resuscitation in dehydrated or endotoxemic ruminants.38 A rate of 4 to 5 mL of hypertonic solution per kilogram should be administered IV through the jugular vein over 8 to 10 minutes. Animals should be provided with a supply of fresh water immediately after the treatment, or an intravenous infusion of an isotonic crystalloid solution should be instituted. Cattle not observed to drink within 5 minutes should have 20 L of water pumped into the rumen.38 An administration rate for a hypertonic solution of over 1 mL/kg/min should be avoided because it induces a potentially fatal hypotension, coupled with a decrease in cardiac contractility.38
Correction of Acid-Base and Electrolyte Imbalances. Correction of electrolyte imbalances should be based on laboratory results when available. Previous treatments should be considered (e.g., intravenous calcium, orally administered magnesium hydroxide) to initiate the most appropriate fluid therapy if no laboratory results are available. Most animals with acute abdominal diseases suffer from metabolic alkalosis, hypochloremia, and hypokalemia.
Calcium homeostasis is fragile in postpartum dairy cattle. Hypocalcemia is common in ruminants with gastrointestinal disorders or simply anorexia, particularly in lactating cows.17,34 Moreover, metabolic alkalosis, frequently observed in cases of acute abdomen, is strongly associated with subclinical hypocalcemia.7,39 Calcium ions are of particular importance in gastrointestinal motility. First, in the gastrointestinal smooth muscles, the channels responsible for generating action potentials are calcium-sodium channels.40 Second, gastrointestinal smooth muscle contraction occurs in response to the entry of calcium into the muscle fiber.40
The Ringer's solution containing 8.6 g of NaCl per liter, 0.3 g of KCl per liter, and 0.3 g of CaCl2 per liter, yielding 147 mEq/L Na, 155 mEq/L Cl, 4 mEq/L K, and 4 mEq/L Ca, is the commercially available solution of choice. At the author's veterinary teaching hospital, a homemade solution (7.5 g of NaCl per liter, 1.5 g of KCl per liter, and 5.75 g of Ca2+ per liter [25 mL of 23% calcium borogluconate per liter], yielding 128 mEq/L Na, 148 mEq/L Cl, 20 mEq/L K, and 26 mEq/L Ca) is used for adult cattle. The author and associates usually begin fluid therapy with rapid administration of a 0.9% NaCl solution (15 to 20 mL/kg/h) for rapid ressucitation and then administer the homemade solution at a rate of approximately 4 to 5 mL/kg/h.
Control of Pain and Inflammation. Pain and inflammation are important causes of gastrointestinal hypomotility. Gastrointestinal pain increases sympathetic tone, causing general inhibition of the gastrointestinal tract.40,41 Numerous inflammatory mediators are released during disease of the gastrointestinal tract and alter intestinal motility.42 Peritoneal inflammation or irritation and associated pain may initiate ileus in several species.42 Release of proteinases, vasoactive substances, free oxygen radicals, and endorphins secondary to ischemia and reperfusion injury, or endotoxemia, impairs cardiovascular function and decreases gastrointestinal motility.42 Release of inflammatory mediators leads to a pain response and modulates the intensity of noxious stimuli.41 Consequently, analgesic and antiinflammatory drugs appear essential in the management of acute abdomen. These drugs must be used with caution; NSAIDs may induce abomasal ulcers, particularly in an anorexic patient, and analgesics may mask clinical signs (pain, fever) and thereby compromise adequate case management through a delay in surgery.
NSAIDs are the most commonly used drugs for gastrointestinal pain management in cattle. There has been no comparison of the efficacy of the different NSAIDs available in food animal medicine specifically in relation to their use in the management of acute abdomen. In some countries, meloxicam is approved for the reduction of pain associated with abdominal surgery. Preoperative and postoperative administration of flunixin, ketoprofen and meloxicam was demonstrated to have positive effects on animal recovery and pain control after left abomasal displacement surgery43,44 or fistulation surgery.45,46 However, no recommendation can be made about which one is most effective.44,47 Ketoprofen and flunixin appear to have similar activities in endotoxic calves.48 Meloxicam has been reported to decrease the severity of clinical signs and to reduce the production of thromboxane B2 in calves with experimentally induced endotoxmia.49 The choice of NSAID becomes a matter of previous experience, comparative medicine, legislation, and cost. In equine gastrointestinal pain, a poor or short-duration response to NSAIDs indicates a need for surgery.41 This principle can be applied to cattle with caution because of their different behavior in response to pain.
O2-Agonists that function as sedatives and analgesics, such as xylazine, detomidine, and medetomidine, could also be used to relieve pain in cases of acute abdomen. All are considered strong analgesics that can alleviate most visceral pain, at least temporarily, in equine medicine.41 There are few data on the use of α2-agonists for the management of acute abdomen in cattle. In a cow with a large intestinal obstruction, signs of abdominal discomfort disappear immediately for at least 1 hour after the administration of a single dose of xylazine (0.05 mg/kg IV).50 Different side effects must be considered before the administration of α2-agonists. Xylazine is reported to have significant effects on the gastrointestinal tract in cattle, decreasing reticuloruminal and intestinal motility.51 Because of the hemodynamic changes associated with the administration of α2-agonists, these drugs must be used with caution in hypotensive patients and those suffering from shock.52 α2- Agonists can mask surgical pain and delay the decision for surgery. This is particularly critical with the use of detomidine.41 Finally, dose and administration of α2-agonists should be used with care if standing surgery is planned, as they may influence the animal to lie down.
Opioids, morphine or butorphanol can also be used alone or in combination to control abdominal pain. Information regarding their use in this situation in cattle is lacking. To the author's knowledge, opioid usage was studied in cattle in castration, dehorning, and preoperative analgesia but never for abdominal pain control. In the author's clinic, after the diagnosis of a nonsurgical process or correction of a surgical process, clinicians administer morphine (0.1 mg/kg, IM or SC), or butorphanol (0.05 to 0.1 mg/kg, IV, IM, or SC) or a continuous- rate infusion of a combination of ketamine (0.2 mg/kg/h) and butorphanol (0.02 mg/kg/h).
Finally, lidocaine may be used for its analgesic and antiinflammatory effects, as well as its potential prokinetic effects. As described in horses, a continuous IV infusion of lidocaine at a rate of 3 mg/kg/h after an initial dose of 1 mg/kg (IV, over 15 min) can be administered. However, no data are actually available about its effect on the control of pain and inflammation and on the gastrointestinal motility in cattle.
Antimicrobial Drugs. Bacterial translocation from the intestines can occur in cases of mechanical or functional ileus secondary to bacterial overgrowth, inflammation, and impairment of barrier function of the intestinal wall. A systemic broad-spectrum antibiotic treatment should be instituted when a septic process is suspected. This initial antibiotic therapy should be effective against Gram-negative, Gram-positive, aerobic, and anaerobic pathogens. The choice of antibiotic should also take into consideration legal aspects and the cost of the treatment. β-Lactams, tetracyclines, and trimethoprim- sulfadoxine appear to be good choices. In ruminants, there is no accepted recommendation for the duration of treatment.
Other Medical Treatments. The use of laxatives (magnesium hydroxide, mineral oil, liquid paraffin) in cases of suspected gastrointestinal obstruction or ileus in cattle has no therapeutic basis. Moreover, these treatments may exacerbate the condition. Because the intestines are already filled with gas and fluid, laxatives only impose additional distention. In human medicine, laxatives are frequently used for the treatment of POI; however, no study could demonstrate their actual benefit.53 Braun and colleagues reported that the use of laxatives for the treatment of cecal disorders delayed the time to first defecation.54 Moreover, magnesium hydroxide may be responsible for detrimental effects such as decreased potassium absorption, metabolic alkalosis,55 sedation caused by hypermagnesemia,55 increased ruminal pH,56 and decreased ruminal microbial activity.56
Motility-modifying agents may be used in the management of gastrointestinal disorders. In most cases, intestinal motility is restored when pain is relieved and electrolytic imbalances are corrected. Steiner51 and Constable and colleagues57 reviewed the different prokinetics that can be used in ruminant medicine and their clinical implications. In cattle, according to their reviews, erythromycin (10 mg/kg, IM, bid for 2 days [Erythro-20051] or 8.8 to 10 mg/kg IM57) is the most effective drug for the treatment of abomasal hypomotility and can be used for the postoperative treatment of abomasal displacement or torsion. However, in a context of antimicrobial stewardship, the use of antimicrobial drugs for purpose other than antibacterial activity is controversial and should not be recommended. Bethanechol (0.07 mg/kg, SC, tid for 2 days, not approved for food animal use in the United States) alone or in combination with metoclopramide (0.1 mg/kg, SC or IM, tid for 2 days, not approved for food animal use in the United States), increased the contractility of abomasal smooth muscles, but no data on in vivo efficacy are available.51,57 Metoclopramide alone is ineffective in cattle and sheep for the treatment of abomasal hypomotility.51,57 Bethanechol (0.07 mg/kg SC tid for 2 days; not approved for food animal use in the United States) can be used for conservative or postoperative treatment of cecal disorders and treatment of paralytic ileus.51
In contrast to cattle and sheep, in goats metoclopramide (0.5 mg/kg IM or IV; not approved in the United States) has been reported to significantly increase myoelectric activity of the duodenum.51 Cisapride (0.5 mg/kg PO, not approved in the United States) was believed to be responsible for an increase in abomasal emptying rate in one study in calves.58 However, in vitro, cisapride did not demonstrate any significant effect on the contractility of smooth muscle of cows from the pyloric antrum, proximal duodenum, and proximal colon.59,60 Continuous infusion of neostigmine (87.5 mg in 10 L of sodium chloride-glucose infusion at 2 drops/sec per cow) was successfully used for the conservative and postoperative treatment of cecal disorders.54 In that clinical report, this protocol was preferred to those previously reported (neostigmine SC every hour over 2 to 3 days in doses that gradually decreased from 12.5 mg to 2.5 mg).54 Drug administration was easier and involved fewer disturbances for the animal.54 However, no control group was included in this study. Also, neostigmine has been reported to have a pronounced effect on intestinal contractility, causing uncoordinated spikes to become more frequent, thereby compromising the potential beneficial effect.60
No prokinetic drug is reported to directly increase ruminal motility. In cases of prolonged anorexia or acute indigestion, ruminal flora can be disturbed and reduced. Transfaunation may help rapidly reconstitute the ruminal flora and hasten return to normal function of the rumen and the digestive tract. The technique for and beneficial effects of transfaunation (reduction of ketonuria, increased feed intake, and higher milk yield) have been reported in the postsurgical treatment of left abomasal displacement.61
FOLLOW-UP. When a definitive diagnosis cannot be made, close monitoring of the animal may be indicated (Fig. 32.127). Follow-up must also be performed after to surgery to ensure
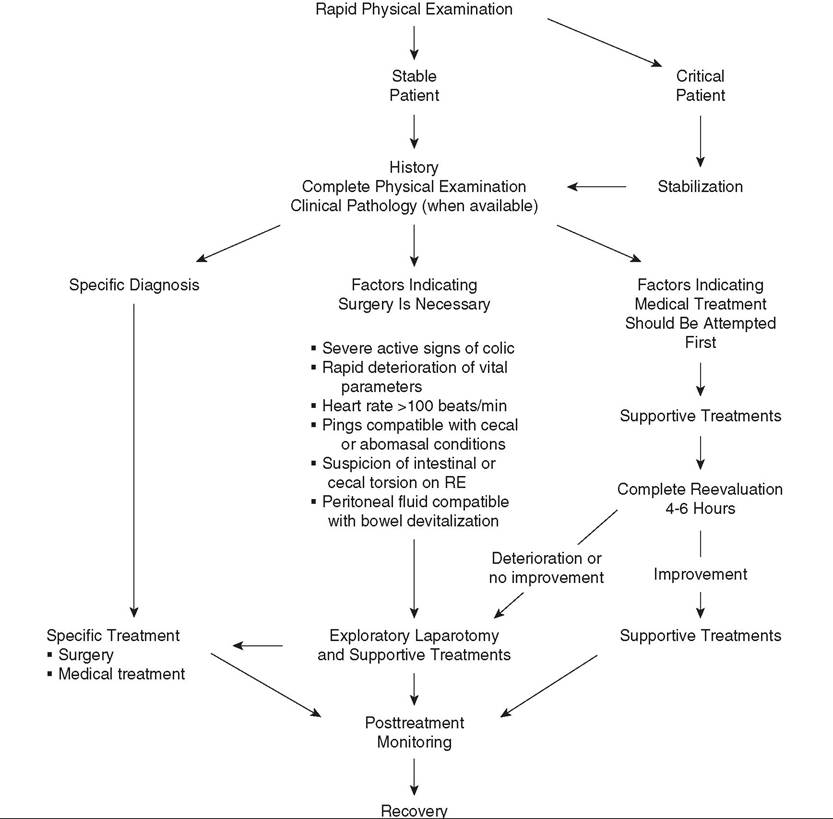
FIG. 32.127 Suggested decision tree for cattle with an acute abdomen. RE, Rectal examination.
adequate response to surgical treatment and to allow possible adjustment of treatment. In a referral hospital, the animal should be reevaluated every 4 to 6 hours. In field practice, vital parameters, rectal palpation, presence and consistency of feces, and pain may be reevaluated every 6 to 12 hours. A significant reduction of heart rate was observed 4 and 6 hours after the initiation of treatment in cases of cecal dilation.54 Feces are usually passed within 4 to 6 hours after surgery in cases of intestinal volvulus or cecal disorders. Failure to defecate for 24 hours or more is abnormal in cattle and therefore indicates persistence of intestinal obstruction and may adversely affect the prognosis. Deterioration or persistence of clinical signs despite the initiation of supportive treatment is also an indication for surgery. Surgical exploration is indicated if the following clinical signs are observed: persistence of colic, development of abdominal distention, heart rate exceeding 100 beats/min, scant feces, typical abomasal or cecal pings, or paracentesis results that indicate bowel devitalization.
The decision for surgery or medical treatment remains challenging in cases of acute abdomen in ruminants. Optimal management of acute abdomen prevents any unnecessary delay in cases requiring surgery and avoids unnecessary surgery. Knowledge of diseases associated with signs of acute abdominal pain is important, but no clinical signs are specific for a particular problem, and a specific diagnosis cannot be established postoperatively in many cases. On the basis of a systematic approach to clinical examination and a judicious use of ancillary tests, the clinician may be able to identify cases that necessitate immediate or delayed surgery, avoid unnecessary surgery, and establish a cost-effective management plan.