Indigestion in Ruminants
Franklyn Garry • Craig McConnel
Definition and Etiology
Indigestion is a general term for a group of diseases characterized by dysfunction of the reticulorumen. Some texts have limited the use of the term to a single, poorly defined entity that includes inappetence, decreased reticuloruminal motility, and abnormal feces, with a nonspecific cause that involves intake of abnormal feed.
The more generalized term applied here incorporates a pathophysiologic classification scheme of forestomach disturbances that was devised by workers in■ BOX 32.4
Classification of Ruminant Indigestion
Primary Indigestion
Reticuloruminal Motor Disorders or Diseases of the Rumen Wall
Traumatic reticuloperitonitis
Frothy bloat
Free gas bloat
ReticulitisZrumenitis
Ruminal parakeratosis
Obstructive (vagal) indigestion (failure of omasal transport, failure of pyloric outflow, and free gas bloat)
Obstruction of the cardia
Obstruction of the reticuloomasal orifice
Diaphragmatic hernia
Reticuloruminal Fermentative (Microbial and Biochemical) Disorders
Inactivity of rumen microbial flora (caused by poor-quality roughage that leads to rumen impaction)
Simple indigestion
Acute ruminal lactic acidosis
Subacute ruminal acidosis
Rumen alkalosis
Putrefaction of rumen ingesta
Secondary Indigestion (Secondary to
Systemic Illness)
Secondary reticuloruminal motor inactivity
Secondary reticuloruminal microflora inactivity
Abomasal reflux
Germany.43 An absolute division of the pathologic processes is impossible because the various forestomach functions are interdependent; that is, abnormal motor function affects microbial fermentation by altered mixing or passage of ruminal fluid out of the forestomach chambers, whereas abnormal fermentation products secondarily alter motor function.
Nevertheless, this classification provides a clinically useful diagnostic framework by emphasizing the underlying pathophysiologic mechanisms of different forestomach disturbances.The primary indigestions include diseases in which the reticulorumen is directly affected and responsible for the major clinical signs (Box 32.4). These problems can be divided into two categories:
1. Abnormal motor function of the reticulorumen, including disease of the reticuloruminal wall, its neuromuscular function, or impedance to the passage of ingesta
2. Abnormal contents of the reticulorumen, with dysfunction of microbial and biochemical fermentation
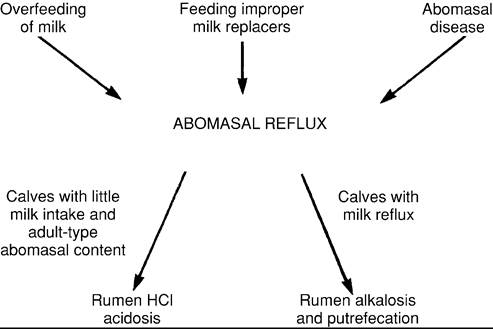
Secondary indigestions are the sequelae of systemic problems or disease in other organ systems. For example, problems such as endotoxemia, fever, or depression can produce anorexia, secondary ruminal hypomotility, and decreased microbial fermentative function. Primary abomasal disease can depress ruminal function, inhibit ruminal outflow, and cause reflux of abomasal contents back into the rumen.
With the exception of penetrating foreign bodies and sporadic infections of the forestomach wall (e.g., actinomycosis, mucormycosis), indigestions are due to abnormal physiologic function. In adult ruminants, one or more of the homeostatic processes of the fermentative environment are disturbed (e.g., an excessive carbohydrate intake generates an excessive amount of acid product; abnormal regulation of the ruminal motility pattern disturbs the mixing or aboral passage of ingesta). In young ruminants, the forestomachs are actively developing, and indigestions can result from disturbances of the developmental mechanisms. The forestomach diseases of young ruminants generally have received little attention, but they can be recognized and appropriately treated within a classification scheme similar to that for adult ruminants.44
Pathophysiology
Digestion of feedstuffs in the reticulorumen is accomplished by microbial fermentation.
The mucosal epithelium absorbs and exchanges products of fermentation but performs essentially no secretory function. Appropriate forestomach fermentation depends on the coordination of processes that provide a fairly constant reticuloruminal environment. The requirements include addition of appropriate amounts and types of feed substrate and water by ingestion; buffering of substances from the saliva to counteract the acid nature of fermentation products; eructation of the gaseous products of fermentation; coordination of reticuloruminal motility to provide mixing; rumination and remastication; aborad passage of ingesta; temperature maintenance; and exchanges of electrolytes and VFAs across the ruminal wall. Because these functions are intimately interrelated, abnormalities in any one of them can lead to digestive disturbances.CLINICAL SIGNS AND DIFFERENTIAL DIAGNOSIS OF INDIGESTION
General Signs. A general physical examination allows the practitioner to recognize signs of reticuloruminal problems (Table 32.14) and to assess whether a disease is present that could induce reticuloruminal dysfunction as a secondary phenomenon. General signs common to all forms of indigestion include a reduction in or absence of appetite, dullness or depression, and decreased animal productivity. The most common clinical signs of ruminal dysfunction are a decrease, absence, or abnormality of ruminal contraction sounds in the left paralumbar fossa or an abnormal left-sided abdominal contour. The left abdominal wall may show gauntness and decreased filling or display gross distention. It is often the failure to detect signs of another primary disease as the cause of ruminal dysfunction that directs attention to the forestomach as the possible primary site of disease. Indigestion in calves effectively produces a state of malnutrition, and additional signs in these growing animals include poor growth rate and long, rough hair coat. The acuteness of onset and the severity of these signs depend on the inciting cause of the indigestion.
Specific abnormalities in the ruminal motility pattern are discussed in more detail, but most indigestions are marked by decreased or absent ruminations (regurgitation and cud chewing) and depressed ruminal contractions.140 Only early cases of frothy bloat and some cases of obstructive (vagal) indigestion display increased ruminal motility.Body temperature usually is within normal limits because the causes of indigestion are mainly physiologic abnormalities. Exceptions include TRP and occasional cases of rumenitis with significant inflammation. Disturbances of heart rate, respiratory rate, hematologic parameters, and body fluid vary tremendously among different forms of indigestion and different cases of any one form of indigestion. For example, an acute onset of severe ruminal bloat might produce a stress leukogram and severe disturbance of the cardiovascular and respiratory systems, whereas mild or chronic bloat may produce no remarkable change in these systems. Rapid accumulation of fluid in the forestomach chamber in severe ruminal acidosis with grain overload can induce severe dehydration with hemoconcentration, an inflammatory response, systemic acidosis, and increased heart and respiratory rates, whereas slow fluid sequestration in some cases of obstructive (vagal) indigestion may not induce marked changes in these parameters.
■ TABLE 32.14
Clinical Signs Typically Associated With Primary Indigestion
Signs
Associated Problems
Fever
Decreased ruminal filling
Abdominal distention
Excessive fluid (or froth) in the rumen with loss of normal ingesta stratification
Excessive firm, fibrous material in rumen Firm, doughy ingesta in ventral rumen with
decreased ruminal filling Ruminal hypermotility Abdominal pain, either present or can be elicited Abnormal feces
Decreased quantity, firm, dry, with increased fiber length
Feces with abnormal amounts of whole cereal grains Greasy consistency with very fine particle size Foamy, fluid, yellowish color, acidic odor Pasty to fluid consistency with foul odor Decreased quantity, dry, otherwise unremarkable Vomiting (rare)
Traumatic reticuloperitonitis, reticuloruminitis
Fermentative indigestion and secondary indigestion (especially with chronic anorexia) in which passage of material from the rumen is not impeded See Fig.
32.119Acute ruminal acidosis, vagal indigestion, frothy bloat, anterior intestinal obstruction
Ruminal inactivity caused by poor-quality roughage
Prolonged ruminal stasis caused by chronic disease with anorexia Early cases of frothy bloat, some cases of vagal indigestion Traumatic reticuloperitonitis, abomasal ulceration, reticuloruminitis Traumatic reticuloperitonitis, omasal transport failure, ruminal inactivity with poor-quality roughage; also dental disease and some abomasal disease
Acute or chronic ruminal acidosis
Pyloric outflow failure, abomasal displacement
Acute ruminal acidosis
Fermentative indigestion, enteritis
Anorexia (various causes), acute indigestion before later development of abnormalities
Ruminal overdistention with vagal indigestion, inflammation of reticulorumen, reticuloomasal orifice obstruction, diaphragmatic hernia, some intoxications (differentiate from esophageal disease)
Most of the primary forestomach diseases do not induce remarkable changes in the serum biochemistry profile. In lactating or heavily pregnant animals, anorexia may induce a secondary form of ketosis, which is detected by the presence of urine or blood ketones. Affected animals must be carefully examined to differentiate ketosis with secondary anorexia and decreased ruminal activity from primary indigestion with secondary ketosis. Mild to moderate hypocalcemia and hypokalemia are commonly identified abnormalities in many cases of indigestion, especially when anorexia has been prolonged.
The history is important, especially with regard to the animal's feeding. Characteristics of the feed determine the type of fermentation pattern to be expected. Knowledge of the nutrient content thus allows an assessment of the biochemistry of microbial digestion. Consumption of a high-concentrate, low-fiber ration or legume pasture may lead to frothy bloat. A ration of poor-quality hay or straw may result in low microbial fermentative activity and accumulation of impacted indigestible roughage.
Overeating of carbohydrates or sudden access to concentrate feeds without adequate adaptation time can induce chronic or acute ruminal acidosis. The feeding history should agree with the findings from inspection of the ruminal contents, or the history should be suspected to be inaccurate. The amount and consistency of the feces should also provide supportive evidence of the type and amount of feed intake.Abdominal Contours and Animal Stance. Visual inspection of the abdominal contours allows assessment of the degree of forestomach filling (Fig. 32.128). Indigestions can be characterized by decreased, normal, or excessive filling of the reticulorumen. Most primary and secondary indigestions are associated with ruminal hypomotility and anorexia. Thus the rumen usually shows no obvious distention and may have less filling than normal, especially when the duration of the disease is prolonged. Forms of indigestion in which abnormal ingesta or abnormal ruminal motility prevents effective flow of ingesta (overfeeding of poor-quality roughage, obstructive indigestion) or in which fluid is actively sequestered in the reticulorumen (acute ruminal acidosis) typically cause some degree of forestomach distention (See Fig. 32.128).
A left-sided or bilateral ventral abdominal wall distention indicates ventral ruminal dilation, although advanced pregnancy and hydrops conditions must be considered. Distention of the dorsal left flank results from ruminal tympany with or without distention of the ventral rumen. Left abomasal displacement can produce mild distention of the dorsal left flank under the caudal ribs and extending into the paralumbar fossa, but the abdomen usually appears gaunt and empty when viewed from the side or the rear. Occasional cases of left displaced abomasum appear to inhibit eructation and produce gross ruminal tympany as the primary sign. Release of free ruminal gas through a stomach tube and reexamination for abdominal pings reveals this cause of secondary ruminal dysfunction. Frothy bloat in ruminants is discussed further in this chapter. Free gas accumulation is often secondary to the causes of ruminal motility inhibition and is an important sign of indigestion (Table 32.15). Right-sided abdominal distention suggests the various conditions of dilation, displacement, and obstruction or ileus of the intestines and abomasum. The diseases that cause obstruction and reflux of abomasal ingesta into the rumen may result in reticuloruminal distention. Prolonged cases of gastrointestinal obstruction at any site and generalized peritonitis can produce gross bilateral dorsal and ventral distention of the abdomen.
Affected animals should be studied for signs of pain. A pain-filled expression, reluctance to move, an abnormal stilted gait, an arched back with a tucked-up abdomen, and an extended neck are typical signs of anterior abdominal pain. These signs may indicate TRP, abomasal ulceration, or another source of pain. A similar stilted gait and reluctance to move are typical of laminitis, a common sequela of acute ruminal acidosis.
Palpable Findings. Deep palpation of the left side of the abdomen is used to determine the consistency of the ruminal contents and thus the nature and volume of the ingesta (see Fig. 32.128). In normal animals the organized contraction sequence produces a layering effect.155 A fluid consistency can be palpated ventrally, whereas the consistency is firm and doughy dorsally. The doughy layer consists of the fibrous portion of the feed. In general, an animal fed a high-roughage diet has a more prominent layer of doughy ingesta. The ruminal contents of an animal fed concentrate feed are softer. In sheep and
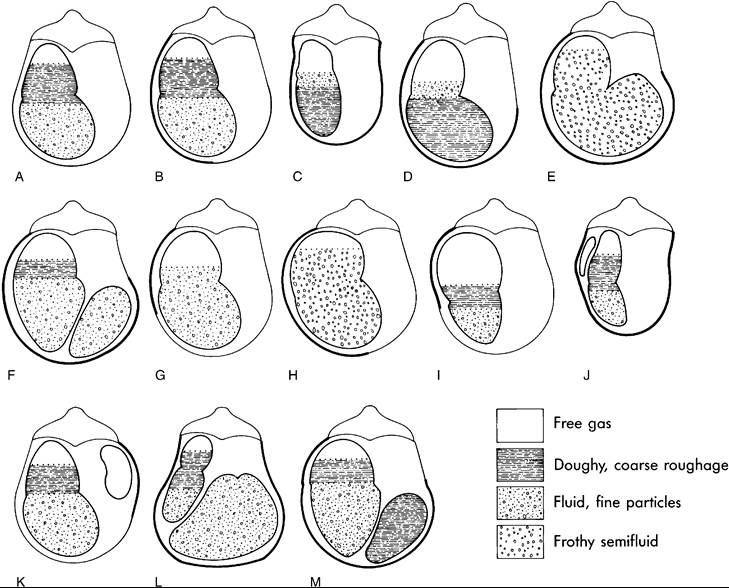
FIG. 32.128 Diagrams of abdominal contours (viewed from the rear) and abdominal palpation findings characteristic of cattle with various types of indigestion and other abdominal diseases. A thin line for the abdominal contour indicates the normal configuration. Bold lines indicate areas of the abdominal contour that typically deviate from normal in affected animals. A, Normal. B, Acute onset of rumen stasis with simple indigestion and traumatic reticuloperitonitis (findings: mild ruminal distention with normal layering of rumen content). C, Prolonged rumen stasis and anorexia: the most common results of subacute or chronic disorders such as microbial or fermentative indigestions, traumatic reticuloperitonitis, and secondary indigestions (findings: reduced rumen fill; “tucked-up abdomen”; firm, doughy contents that gravitate ventrally). D, Rumen inactivity with indigestible roughage (findings: rumen distended with firm, doughy contents that accumulate ventrally; recurrent free gas bloat often present). E, Omasal transport failure (findings: L-shaped rumen with gross accumulation of frothy ingesta; rumen hypermotility often present; free gas accumulation varies). F, Pyloric outflow failure (findings: fluid accumulation in abomasum; abomasal reflux to rumen common; doughy rumen content that usually accumulates dorsally until rumen stasis or anorexia is prolonged; abdominal contour similar to that for omasal transport failure). G, Acute rumen acidosis (findings: rumen distended with fluid; some free gas bloat common). H, Frothy bloat. I, Free gas bloat or chronic free gas bloat (findings: accumulation of gas in dorsal sac; layering or rumen contents usually normal; with chronicity, rumen fill often decreased; associated with some microbial or fermentative disorders and with esophageal and cardiac disorders). J, Left displaced abomasum (findings: gas-filled abomasum that often causes slight bulge of paralumbar fossa; rumen fill usually reduced). K, Right displaced abomasum, abomasal volvulus, cecal torsion (findings: distention of right flank with gas-filled viscus; rumen fill and consistency usually normal). L, Hydrops (findings: ventral abdomen distended with fluid-filled uterus: rumen fill usually decreased). M, Abomasal impaction (findings: abdominal contour similar to those in E and F; abomasum filled with firm ingesta).
■ TABLE 32.15
Differentiation of Types of Bloat Through Nasogastric Intubation
| Results of Intubation | Probable Causes of Bloat |
| Tube does not pass. | Esophageal obstruction |
| Tube passes with resistance and releases ruminal gas. | Esophageal compression caused by thoracic inflammatory or neoplastic disease |
| Tube passes easily and releases ruminal gas. | Distortion of the cardia caused by inflammation, neoplasia, or abnormal anatomy such as abomasal displacement Ruminal stasis caused by reticuloruminal fermentative disorder, hypocalcemia Obstruction of cardia with ingesta (overfilling of rumen) or pedunculated mass Rumenitis (reticulitis) Weakened ruminal contraction caused by chronic overdistention with ingesta (vagal indigestion, indigestion with poorly digestible forage) |
| Tube passes easily but does not release gas | Frothy bloat |
| or releases small amount of foamy ingesta. | Frothy ruminal contents caused by abnormal motility in some forms of vagal indigestion |
goats, the normal dorsal rumen is softer than that of cattle no matter what the feed. In the normal condition, a small layer of free gas is present in the most dorsal region. Distention with gas or foamy feed produces a taut, elastic tension. With free gas bloat, the doughy layer can still be appreciated ventral to the gas accumulation, but in cases of frothy bloat, the doughy layer is much less prominent. Most cases of obstructive (vagal) indigestion and some cases of proximal intestinal obstruction cause gross dilation of the rumen with fluid or foamy contents that may fluctuate on ballottement.
Overfeeding of indigestible poor hay or straw with resultant inactivity of ruminal microbial fermentation leads to accumulation of more fibrous material than normal that barely yields to deep palpation. With prolonged or severe ruminal stasis, as may occur in TRP, the lack of ruminal motility leads to failure to maintain the normal layering of the contents. In some instances the ventral portion of the forestomach is firmer than the area above. During severe ruminal acidosis, fluid accumulates in the forestomach. This can lead to some degree of abdominal distention, and on palpation the ruminal contents are fluid and may even splash with ballottement.
The rumen should also be palpated rectally; a comparison of these findings with those obtained externally may be revealing. Moderate degrees of free gas accumulation are often more easily detectable on rectal palpation. Rectal palpation is also useful in distinguishing the presence of an L-shaped rumen, in which the ventral sac of the rumen is grossly distended and extends toward the right ventral quadrant. It is important to differentiate an L-shaped rumen from either abomasal distention or impaction, which can manifest in a similar external abdominal contour. It is also important to palpate for the size of the lymph nodes in the longitudinal groove of the rumen. These can enlarge to prominent size when rumenitis is present. The organs in the right half of the abdomen should be assessed as sources of abdominal problems.
Rectal examination is impossible in small ruminants and calves. External palpation with both hands can be valuable in these animals. In calves and goats, it is the best method for detecting bezoars or clotted clumps of milk in the rumen and for palpating intussusception, umbilical abscesses, or grossly abnormal kidneys.
Palpation of the left paralumbar fossa reveals the presence of ruminal contractions. In a normal animal, three contractions should occur over a 2-minute period. One of these contractions should be associated with an eructation of gas, which can be appreciated both visually and audibly. The rate of eructation increases or decreases in proportion to the fermentative production of gas. Most indigestions produce decreased ruminal motility or ruminal stasis. Early cases of frothy bloat and some forms of obstructive indigestion can result in prominent hypermotility. The motility pattern is characterized by changes in both frequency and strength, and weak contractions can also be detected by palpation. Some cases of secondary indigestion, in which the decrease in ruminal function is a result of inappetence rather than an inhibition of ruminal motility, manifest a normal contraction frequency but decreased contraction strength. The duration and strength of ruminal contractions are primarily determined by the nature of the forestomach contents, whereas the frequency relies on medullary gastric center control. Decreased ruminal fill, decreased fiber content of the ingesta, or overdistention of the ruminal wall musculature results in reduced strength and duration of the contraction sequence. These distinctions can be important in determining the cause of decreased ruminal motility.
Auscultable Findings. Auscultation of abdominal sounds is performed over several sites in the left flank and rib areas. Initial auscultation is used to assess the nature, frequency, and strength of ruminal sounds. This information can be compared with the information about ruminal motility gathered on palpation. The sounds represent the friction of fibrous ingesta rubbing against the ruminal wall as the ruminal sacs contract and mix their contents. In healthy cattle on a roughage diet, the normal rustling sound is prominent and prolonged with each contraction cycle. The ruminal contents of animals fed a high-concentrate diet produce less sound because very low fiber rations induce weaker contractions, and less fibrous material is in contact with the ruminal wall.
As with palpation, both the frequency and the nature of the sounds yield information about reticuloruminal motility. The ruminal motility pattern is disrupted in obstructive (vagal) indigestion. Although contractions are present and may be more frequent than normal, their lack of normal coordination can lead to a churning of the ingesta without the usual progression of transport. This disrupts the normal stratification of the contents and produces abnormal sounds that are heard as a rumbling, bubbling, or splashing. When stratification is disrupted because of a hypoactive rumen and more fluid is present in the dorsal area of the rumen, contractions produce splashing sounds. The accumulation of gas under these circumstances may produce ringing tones as the fluid moves, similar to the pings found with a displaced abomasum.
Some circumstances necessitate a distinction between primary and secondary contraction cycles, and they can be differentiated by auscultating for reticular contractions. Holding the stethoscope at the seventh intercostal space at the level of the costochondral junction, the examiner can detect a tinkling fluid sound as the reticulum contracts. A hand held in the paralumbar fossa can detect the tensed bulging of the dorsal sac as it contracts, allowing the examiner to determine whether the ruminal contraction is associated with a reticular contraction. Reticular contraction and motility can also be assessed by transabdominal ultrasonography.15,17,19 Hyperactivity of primary cycles associated with feeding or the immediate postprandial period is normal. Mechanical stimulation of buccal sensory receptors can lead to an approximate doubling of the primary cycle rate. Hypermotility that results from excessive secondary contractions, without the normal mixing and propulsion of primary contractions, is abnormal and represents ruminal dysfunction.
Ruminal features related to the size and stratification of ingesta, echogenicity and thickness of the wall, size of the dorsal gas cap, and ruminal height at different intercostal spaces can be achieved with ultrasonography.23 Combining ultrasonography and auscultation with percussion or ballottement allows assessment of gas or fluid accumulations. The sounds heard in the left flank should be compared with those in the left rib area and right side of the abdomen. High-pitched pings and fluid tinkling sounds suggest a viscus filled with gas and fluid. In the left flank this may represent a displaced abomasum, gasforming abscess, pneumoperitoneum, or static rumen. Careful comparison of the sounds heard at different sites, combined with the results of rectal palpation, should enable localization of the source. In general, the rumen can be ruled out as the source of pings if palpation reveals normal doughy ruminal contents, no ruminal tympany is palpated rectally, and sounds of normal ruminal contractions are heard in the paralumbar fossa. Prolonged anorexia associated with infectious or inflammatory diseases such as pneumonia or mastitis can result in a static, underfilled rumen, and occasionally a prominent ping can be auscultated in the left flank, where a filled rumen normally would be found. This condition has been called “ruminal collapse,” and careful evaluation is necessary to distinguish it from leftward displacement of the abomasum. Ballottement of the rumen may reveal splashing fluid sounds without a high pitch when the rumen has accumulated significant fluid. This occurs frequently in cases of severe ruminal acidosis. It may also occur in cases of marked inactivity of the ruminal flora with loss of the normal stratification of ruminal contents.
Pain Elicitation. Tests of pain sensitivity in the anterior abdomen (percussion, deep palpation, withers pinch, xyphoid pressure) are performed to detect localized peritonitis caused by TRP or abomasal ulceration. The same procedures, especially percussion or application of pressure to a localized area in the ventral portion of the abdomen, can be used to localize pain associated with rumenitis or ruminal abscessation or perforating abosomal ulceration.25
Fecal Abnormalities. The rectal examination presents an opportunity to assess the volume and nature of the feces. The feces are abnormal in most cases of forestomach dysfunction. In adult cattle, passage of ingesta through the digestive tract requires 1l∕2 to 4 days. Changes in the feces caused by acute diseases are thus often delayed by a day or longer beyond the first appearance of other clinical signs. Mature cattle typically pass a total of 30 to 50 kg of feces per day, divided into 10 to 24 defecations. The color and consistency of feces are influenced by the feed and should be assessed in view of the feeding history.
Diseases that reduce the flow of ingesta from the rumen to the lower gastrointestinal tract typically result in feces of reduced volume that are firm and dry. These findings are also present with reduced feed or water intake. If normal intestinal function is present, a decreased flow of ingesta from the forestomach allows longer retention in the bowel with greater resorption of water. In severe instances, the feces form into firm disks or balls with a dark, shiny mucus covering. These findings are typical of obstructive indigestion and forestomach diseases that produce ruminal stasis without a grossly abnormal fermentative pattern. Indigestions with abnormal fermentation may produce decreased quantities of dry feces initially but usually result in other fecal abnormalities as the abnormal ingesta passes into the lower tract. Intestinal obstructions also decrease fecal passage to the point of absence, but usually the material passed also has other gross abnormalities such as blood, melena, or discolored mucus.
The particle size of fecal material depends on the frequency and duration of rumination, the activity of the ruminal flora, and the function of the rumen in appropriately sorting out material for passage through the reticuloomasal orifice. Abnormalities of these digestive functions lead to passage of ingesta of inappropriate particle size. Plant fibers in normal bovine feces measure up to 0.5 cm. Particles with inadequate breakdown may measure 1 to 2 cm or longer. This long particle size may be seen in the feces of cattle with TRP, some cases of obstructive indigestion, and poor-quality roughage with insufficient microfloral activity.18,125 Similar findings occur with tooth disease and some cases of abomasitis or cellulitis at the cardia or esophageal groove, in which rumination or activity of the reticuloomasal orifice is inhibited. Whole cereal grains (especially whole corn) may pass in the feces of normal cattle, but excessive amounts of grain should raise suspicion of excessive intake and acute ruminal acidosis. Feces with an abnormally fine particle size and greasy-pasty texture are associated with delayed passage from the forestomach. These are common findings in most cases of obstructive indigestion and abomasal displacement.
The odor of bovine feces is relatively inoffensive in healthy individuals. Foul odors are the result of abnormal fermentation or decomposition. Thus abnormal odor typically occurs when the ruminal fermentation pattern is altered, as in simple indigestion caused by abnormal feed, ruminal acidosis, ruminal alkalosis, or ruminal content putrefaction. A repugnant odor is also typical of enteritis when blood products, inflammatory products, or tissues decompose in the intestinal tract (e.g., Salmonella enteritis). Foamy, fluid feces with a yellow-brown color and acidic smell are typical of ruminal lactic acidosis in adult cattle. Abnormal ruminal fermentation not only produces feces with abnormal odor but also typically leads to a pasty or fluid consistency as well. Exceptions occur in acute cases, when ruminal stasis or the delay in the passage of ingesta from the forestomach can result in normal or firm feces during initial stages of the disease.
Heart Rate. Bradycardia of 40 to 60 beats/min is frequently associated with certain types of indigestion. This sign suggests reflex vagotonia to the heart and has been considered indicative of obstructive indigestion associated with vagal nerve damage. The bradycardia can be alleviated by subcutaneous administration of 30 mg of atropine, which differentiates increased vagal nerve tone from a primary cardiac conduction disturbance. The atropine test is not especially useful because only a minority of obstructive indigestion cases are caused by vagal nerve damage or show bradycardia.18 Advanced cases with severe abdominal distention or fluid imbalances (or both) frequently manifest elevated heart rates (over 80 beats/min). In most cases the other physical signs are more reliable for establishing the diagnosis of obstructive indigestion. Moreover, bradycardia may be observed in other forms of indigestion when ruminal hypomotility is prominent and no significant fluid or electrolyte imbalances are present. Even in normal cattle, postfasting heart rates may drop below 50 beats/min.106 Therefore bradycardia in association with other signs of ruminal dysfunction is probably most useful as evidence that tachycardic stimuli, such as inflammatory, infectious, or fluid balance disturbances, are not prominent factors in the individual disease occurrence.
Vomiting. Vomiting is uncommon in ruminants, but when it does occur, it generally reflects forestomach disease. Regurgitation from the abomasum frequently occurs with abomasal or intestinal disease. Abomasal reflux is not manifested externally and is discussed elsewhere because it is related to forestomach disease. Small volume regurgitation and remastication are routine and normal ruminant functions that do not result in expulsion of material from the mouth. Explosive vomiting of fluid ingesta in large quantity occurs when the reticulorumen is irritated and occasionally when it is overdistended. Vomiting may accompany diaphragmatic herniation of the reticulum, inflammation of the reticulorumen caused by actinobacillosis, obstructive indigestion, or obstruction of the reticuloomasal orifice. Animals are more prone than normal to vomiting around an orally passed stomach tube when they have almost any digestive disturbance. Vomiting also occurs with certain intoxications, most notably azalea, rhododendron, and sneezeweed toxicity and some organophosphate toxicities.
Disorders of Reticuloruminal Motor Function
NORMAL MOTOR ACTIVITY. The two reticuloruminal contraction sequences function independently. The primary cycle of contraction occurs approximately once a minute but more often during feeding and rumination. It consists of a biphasic contraction of the reticulum followed by a contraction that runs caudally across first the dorsal and then the ventral ruminal sacs. At the height of the second reticular contraction, the omasal orifice relaxes and fluid, mostly composed of reticular ingesta, passes into the omasum. This reticuloruminal motility pattern directly influences ruminal fermentation by mechanically mixing the ingesta to provide contact with the microbes and to macerate the particulate matter. The mixing function prevents local accumulations of substrate or end products of fermentation, distributes the buffering saliva for neutralization of acids, and provides increased contact of the fluid with the ruminal wall to promote VFA absorption. The coordinated sequence of contraction of various parts of the ruminal wall maintains a stratification of fluid and particulate matter that selectively sorts the ingesta by particle size. The sorting function serves to retain large particles for further digestive breakdown while promoting passage of small particles (smaller than 6 mm) into the omasum and lower gastrointestinal tract.19,32,155
■ TABLE 32.16
Factors Influencing Vagal Motor Discharge From the Gastric Centers of the Medullaa
| Input | Location | Stimulus |
| Excitation of the Gastric Centers (Causes Increased Rumen Motility) | ||
| Low-threshold tension receptors | Reticulum, medial wall | Mild distention; tension generated during contractions |
| Buccal receptors | Mouth | Feeding (only during chewing) |
| Acid receptors | Abomasum | Increased acidity as abomasum empties |
| Tension receptorsb | Medial wall of cranial rumen sac | Increased rumen gas pressure |
| Inhibition of the Gastric Centers (Causes Decreased Rumen Motility) | ||
| High-threshold tension receptors | Reticulum and cranial rumen sac | Bloat or other severe ruminal distention |
| Tension receptors | Abomasum | Abomasal distention |
| Chemical receptors | Reticulum, rumen | Increased concentration of undissociated volatile fatty acid with rumen acidosis; also locally activated by some toxins |
| Pain receptors in body increase | Anywhere in body; can act directly | Pain, especially abdominal |
| sympathetic tone and adrenal | and through medullary gastric | |
| secretory activity | centers | |
| Gastric centers | Medulla | Anesthesia, depressant drugs, toxins, endotoxins, fever, acidosis |
| Hypocalcemia | Reticuloruminal smooth muscle | Hypocalcemia |
aThere is no inherent reticuloruminal motility such as that found in the intestines. bSecondary cycle activity; independent of primary cycle activity.
The secondary contraction cycle does not involve the reticulum. It begins in the caudal blind sacs, and a wave of contraction runs cranially across the dorsal rumen, pushing the gas cap into the cardia region. Eructation ensues, eliminating the gases generated by fermentation. Typically one secondary cycle contraction follows two primary cycles, so that three contractions occur every 2 minutes.33 Two additional special contractions have been identified in sheep: primarysecondary contractions and prosecondary contractions.9 These contractions appear when intraruminal pressure increases and allow ruminal gas to be evacuated. The primary-secondary and prosecondary contractions appear to help minimize free gas bloat when gas production is excessive.
Maintenance of the motility patterns requires well- coordinated neural control. The pathophysiologic mechanism of the first group of primary indigestions (i.e., diseases of the reticuloruminal motor function) involves disturbance of the mechanisms of normal ruminal motility, which secondarily affects ruminal fermentation.
The ruminal contraction sequences described rely almost completely on motor nerve activation arising from the medulla oblongata, in contrast to the intrinsic segmental and peristaltic movements of the intestine. Gastric centers in the medulla integrate sensory input and generate motor impulses, both of which are carried in the vagus nerves. The gastric centers have neither spontaneous activity nor an inherent rhythm. Generation of motor impulses relies on greater excitatory input than inhibitory input from the sensory nerves to determine the rate, magnitude, and duration of primary cycle contractions. During the quiescent period between the primary contractions, while the medulla collects the sensory information, there are no tonic vagal motor impulses.94,153
The splanchnic nerves also affect reticuloruminal motility by direct innervation and by neurohumoral effects of adrenal secretion. These nerves are not required for generation of normal contractions. The effect of splanchnic stimulation is inhibition of reticuloruminal motility. Splanchnic sensory nerves innervate sensory receptors in other areas of the gastrointestinal system, and some abnormalities such as intestinal distention or surgical manipulation produce reticuloruminal inhibition by means of reflex from splanchnic afferent activity.153
Primary Cycle Activity. A decrease in or absence of normal primary cycle activity (i.e., ruminal hypomotility or stasis) implies either a decrease of vagal motor discharges originating from the gastric centers or an ineffective motor response after motor impulse, as in cases of hypocalcemia. Causes of decreased motor discharges include the following:
1. Decreased excitatory input to the gastric centers
2. Increased inhibitory input to the gastric centers
3. Depression of the gastric centers
4. Defective vagal transmission of motor impulses
5. Other factors
Decreased Excitory Input. The three most important excitatory inputs to the gastric centers are from (1) low-threshold tension receptors in the reticulum, (2) buccal receptors in the mouth, and (3) acid receptors in the abomasum (Table 32.16). The tension receptors are located in the musculature of the medial wall of the reticulum. They are stimulated by mild distention during the resting phase and thereby influence contraction frequency. They are further stimulated by the tension generated during contraction and thus increase amplitude and duration of the primary cycle contraction. This mechanism is probably responsible for the increase in motility after feeding or during incipient bloat. Any cause of anorexia leading to decreased ruminal fill decreases this excitatory input, which results in ruminal hypomotility. Feeding mechanically stimulates buccal sensory receptors, providing a potent stimulus to both primary and secondary contraction cycles. This reflex can double the rate of primary contractions but is short-lived and declines as soon as chewing activity ceases. Thus anorexia effectively eliminates this potent excitatory input. Abomasal acidity increases as the abomasum empties, and this too provides excitatory input to the gastric centers. The resultant increased reticuloruminal motility leads to increased flow of ingesta to the abomasum, diluting the abomasal acid and maintaining normal filling of the abomasum. Certain types of abomasal disease such as abomasal distention associated with abomasal displacement or abomasal impaction diminish this stimulus to forestomach motility.,,
Stimuli of reticuloruminal motility that are not as well defined include the physical and chemical characteristics of the ruminal ingesta. Fiber and water content, as well as the normal chemical products (i.e., VFAs) of fermentation, are important for normal ruminal contraction. The exact mechanisms through which these factors enhance ruminal motility have not yet been clearly defined,81 but low levels of any of these ingesta characteristics impair normal function, causing decreases of both rumination and primary cycle activity. That these excitatory stimuli are decreased or absent in some feeding regimens and with some of the diseases attributable to abnormal fermentation may account for the impression of hypomotility observed clinically.50
Increased Inhibitory Input. Inhibitory inputs to the gastric center arise from (1) high-threshold tension receptors in the reticulum and cranial dorsal ruminal sac, (2) tension receptors in the abomasum, (3) epithelial receptors that detect high concentrations of nondissociated VFAs in the rumen, and (4) pain elicited at any site in the body (see Table 32.16). The high-threshold tension receptors are sensory nerve endings below the epithelial basement membrane of the reticulum and cranial dorsal ruminal sac. They respond to extreme distention of the wall and serve to modify the end stage of reticuloruminal contraction. With severe bloat or gross ruminal distention from other causes, such as overfilling with indigestible fibrous roughage, they can be continuously activated producing ruminal stasis. Abomasal distention can inhibit primary ruminal contraction cycles presumably through tension receptors in the abomasal wall.78 In normal circumstances this activity serves to decrease the flow of ingesta to the abomasum when it is full. With abomasal displacement or impaction, this reflex may partly account for the observed ruminal hypomotility. Epithelial receptors in the reticulum and cranial dorsal ruminal sac are sensitive to increased concentrations of nondissociated VFAs. Inhibition of forestomach contractions occurs when conditions of excessive fermentation or acidosis increase the concentrations of these substances. Pain can reduce forestomach motility by increasing sympathetic nervous and adrenal secretory activity and by inhibiting the gastric centers. Although painful stimuli in the abdominal viscera are particularly potent, pain from anywhere in the body can inhibit or abolish reticuloruminal motility.94,96,153
Depression of the Gastric Centers. Depression of the gastric centers reduces vagal motor activation of forestomach motility and can be induced by central nervous system depressant drugs and anesthetics such as barbiturates, inhalant anesthetics and xylazine. Endotoxemia, fever, and possibly blood pH and electrolyte abnormalities can induce ruminal hypomotility or stasis through central effects on the gastric centers. These factors may also inhibit ruminal motility by increasing sympathetic nervous activity. In addition, some toxins or other abnormal fermentation products reduce ruminal motility. These substances may act locally at the ruminal epithelial receptors to generate inhibitory impulses, as do increased VFA concentrations, or they may act centrally after absorption into the blood. For the most part, the nature of the substances capable of chemically suppressing ruminal function is unknown, but abnormal fermentation end products are the likely cause of ruminal stasis in indigestion associated with abnormal ruminal contents.50,94,95,155
Defective Vagal Innervation. Failure of vagal nerve transmission of motor impulses has been implicated as the cause of a reticuloruminal contraction abnormality that leads to failure of aborad flow of ingesta (hence the often-used name vagal indigestion). The left and right vagi in the thorax divide into dorsal and ventral branches that unite to form dorsal and ventral vagi as the nerves enter the abdomen. The ventral vagus innervates the cranial and medial parts of the reticulum, the omasum, and the abomasum. The dorsal vagus innervates the rumen and parts of the other segments of the ruminant stomach. Sectioning of more than 50% of the vagal nerve trunks leads to impaired motility function, but in most naturally occurring cases of obstructive (vagal) indigestion, it is not possible to demonstrate nerve involvement. The importance of vagal nerve lesions in the pathogenesis of forestomach disease has been a subject of considerable debate and is discussed later in this chapter.94
Other Factors That Affect the Primary Cycles. Other influences on forestomach motility have been identified. Hypocalcemia inhibits motility by preventing contraction of the musculature after motor nerve discharge. This may explain the reduced ruminal motility seen in early cases of milk fever.77 Low environmental temperatures97,157 and milking7 have been shown to increase ruminal motility mildly, whereas some drugs,24,68,139 hyperglycemia,149 and gastric hormones66 are effective in decreasing reticuloruminal primary cycle contractions. These factors are not discussed further in this text.
Secondary Cycle Activity. The secondary cycle activity responsible for eructation is elicited independently of the primary cycles. An increase in ruminal gas pressure stimulates tension receptors in the medial wall of the cranial dorsal ruminal sac. This triggers relaxation of the cardia and eructation of the gas accumulated in the cardia region by the secondary contraction cycle. Receptors that apparently distinguish gas from fluid or solid matter inhibit opening of the cardia if it is covered by material other than gas. This reflex inhibition of cardia opening is responsible for bloat in cases in which abnormal ingesta cover the area, (as in recumbent animals), in frothy bloat, and when abnormal motility or overfilling of the rumen precludes clearing of the cardia. Under such circumstances and when ruminal distention is not yet extreme, both primary and secondary cycle contractions may increase in frequency. In other forms of bloat, hypomotility is a prominent feature, and the gas accumulates as a result of the poor motility function. This is the most probable cause of bloat in some of the disturbances of fermentative function.
Gross overdistention of the ruminal wall may inhibit motility by stretching the musculature beyond its ability to contract forcefully. If the process leading to the distention develops slowly, the high-tension receptor inhibition of motility appears to adapt, and complete inhibition of motor impulses does not seem to occur. Rather, in these cases motility is present but weak and relatively ineffective. This motility disturbance is likely to occur when poorly digestible roughage accumulates in the forestomach. Patients with this condition often have mild to moderate chronic free gas bloat, which may result from poor ability of the weakened rumen to clear the cardia and dispel the gas.43
Reticulitis and rumenitis. The most important inflammatory problem is reticuloperitonitis caused by sharp foreign body punctures (TRP, hardware disease).108 This disease is discussed elsewhere in this chapter. The localized infection established by reticuloruminal perforation causes inflammation of the forestomach wall and adjacent peritoneal cavity and pain in the anterior abdomen, inhibiting forestomach motility, appetite, and aborad flow of ingesta. Other causes of ruminal wall inflammation can cause acute or chronic forestomach dysfunction. Neutrophilia and hyperfibrinogenemia are routine findings of TRP or rumentis and can aid in differentiating them from other forestomach diseases that do not generally feature hematologic abnormalities.
Most infections of the ruminal wall follow primary mechanical or chemical damage to the mucosa. The secondary invaders colonize the damaged areas and may gain access to the circulation and invade other tissues as well. The ruminal wall may be the niche for some of these microorganisms, and isolates from the ruminal wall have been matched with those isolated from liver abscesses.113 Probably the most common cause of the initial mucosal injury is acute ruminal acidosis produced by grain engorgement (discussed later). Chemical damage resulting in ruminal ulcers also occurs in oak or acorn toxicosis and with ingestion of caustic chemicals. Common secondary ulcer invaders include T. pyogenes, Fusobacterium necrophorum, and several mycotic species.113,151 Mycotic rumenitis can follow ruminal acidosis and septic diseases, especially after the use of oral antibiotics. It also can occur after feeding spoiled and moldy feeds and without apparent predisposing causes.30,76 Diseases that cause anorexia and abomasal reflux of gastric acids may predispose an animal to mycotic rumenitis and omasitis. Mycotic rumenitis can be severe, with vascular thrombosis, infarction, mural necrosis and gangrene sufficient to cause death. Less frequently occurring, specific infections of the ruminal wall include atypical forms of actinobacillosis, actinomycosis, and tuberculosis. These infectious inflammatory diseases of the ruminal wall may be distributed widely throughout the forestomach, depending on the initial site of mucosal injury, but they tend to localize in the ventral regions of the reticulorumen. The granulomatous inflammatory lesions of actinobacillosis and actinomycosis are most commonly found in the cranial forestomach in the area of the esophageal groove.
Neoplastic growths in the rumen have also been identified. These uncommon lesions include papillomas, myxomas, fibromas, carcinomas, and lymphosarcoma.62 These lesions are most commonly localized in the reticulum and cranial rumen near the cardia and esophageal groove.
The importance of these inflammatory reticuloruminal lesions depends on their extent and location. Acute and extensive lesions have been associated with signs similar to those of reticuloperitonitis caused by foreign body puncture, including pain, inappetence, impaired forestomach function, and in some cases death. The more chronic cases may cause forestomach motility disturbances and signs of obstructive indigestion. Pedunculated masses especially, but not exclusively, may obstruct the cardia or reticuloomasal orifice and lead to bloat or reticu- loruminal outflow disturbance. Reticuloruminal inflammation can also result from certain generalized infections. These include BVD, FMD, MCF, and rinderpest. In these cases the forestomach problems are unlikely to be the most important clinical manifestation.
Diseases of the ruminal wall may be differentiated on the basis of the physical examination findings and results of a CBC, abdominocentesis, and ruminal fluid analysis. In many cases exploratory laparotomy is needed to confirm the diagnosis. Rumenitis or reticulitis may respond to antibiotic therapy, but the prognosis in these cases is guarded. Not only is the forestomach inflammation difficult to resolve, but also the hematogenous spread of infection to other organs often causes intractable disease in multiple organ systems.
RUMINAL PARAKERATOSIS. In parakeratosis the papillae are darkly colored, enlarged, thickened, and clumped together. Histologic changes of the epithelial cells include a thickened, cornified layer with abnormal retention of nuclei in the cornified cells. These morphologic changes appear to represent a reaction to persistently high concentrations of VFAs. The changes occur predominantly in animals on pelleted or very finely ground rations, especially when the ration contains a high amount of energy. These rations tend to increase the proportions of propionate and butyrate, reduce the proportion of acetate generated by microbial fermentation, and lower ruminal fluid pH. The growth of the ruminal papillae is promoted by contact with the VFAs, especially butyrate, and secondarily propionate.155 It appears that a disproportion of the concentrations of these VFAs may be the cause of an excessive change in the epithelium of the papillae.55,147,160 Initial changes in the epithelium under these conditions appear to increase the absorption of the VFAs, but in severe cases the absorption decreases. This disease of the ruminal wall is not usually diagnosed as a primary problem. Although it may lead to impaired performance of the animal, the disease signs that lead to its discovery are usually those of chronic ruminal acidosis, a disease with which it often coexists. Parakeratosis can predispose to other injuries of the ruminal wall because the abnormal papillae are more easily traumatized, which leads to chronic inflammatory disease of the wall, as discussed previously. In calves the problem is also associated with the development of hairballs (trichobezoars) because of the propensity of calves fed rations associated with parakeratosis to lick their hair coat.147
Parakeratosis is best treated by correcting the causal feeding error (reducing the amount of concentrate and increasing the feeding of long-stemmed forage). The ruminal papillae can grow or regress in a period as short as 3 weeks when the feed is changed from low- to high-concentrate content or vice versa. Exactly how long it takes for parakeratotic papillae to return to normal remains uncertain, but it probably depends on the degree of change of the diet. The prognosis of this problem is good if inflammation of the ruminal wall is not present.
OBSTRUCTIVE (VAGAL) INDIGESTION. Obstructive indigestion syndrome (vagal indigestion, Hoflund's syndrome) comprises a group of motor disturbances that hinder passage of ingesta out of the reticulorumen or abomasum or both. It is a syndrome, meaning a constellation of signs of disease, but with diverse potential causes. The disease signs are those that would occur if there were a physical obstruction of the reticu- loomasal orifice or the pylorus. The author uses the term obstructive indigestion for this reason. Historically the term vagal indigestion has been used, but this has led to confusion because it implies that the vagal nerve is involved in the development of the syndrome, and this is true only in a minority of cases. Furthermore, damage to the vagal nerve can sometimes cause acute onset of free gas bloat as the most prominent disease sign, so some authors have felt obliged to develop a naming scheme for “vagal indigestion” that includes free gas bloat, even though this occurrence does not fit the syndrome that mimics obstruction of the reticuloomasal orifice or pylorus.
An animal with obstructive indigestion syndrome has progressive abdominal distention, characterized by distention both dorsally and ventrally in the left abdomen and ventrally in the right abdomen, and demonstrates overfilling and enlargement of the dorsal and ventral ruminal sacs with or without overfilling of the abomasum. Appetite gradually diminishes to complete anorexia. Body mass gradually decreases, and the animal may become weak and eventually unable to rise. Fecal output is scant, demonstrating little movement of ingesta through the gastrointestinal tract. In some cases free gas bloat occurs, adding to the abdominal distention. No single pathogenesis produces these signs of disease, and various investigations have yielded conflicting information. ,,42,,4,,,146 It is the combination of all of these signs of disease that define the syndrome. Other disease conditions may cause some of these disease signs individually, but are distinguished from obstructive indigestion because the entire grouping of signs does not occur. For example, frothy bloat produces exactly the same abdominal distention, but it occurs rapidly, it does not lead to chronic loss of body condition, and feces are typically not scant. As an alternative example, free gas bloat can occur in a variety of circumstances but often is not accompanied by gross overfilling of the rumen and apparent obstruction of ingesta passage.
The term vagal indigestion was introduced by Hoflund, who hypothesized that the vagal nerve was damaged and experimentally produced motor defects and disease signs similar to those seen in clinical cases by transecting various branches of the abdominal vagal nerve.72 On the basis of his experimental results, he defined the functional disturbance of stomach motor activity with obstruction of ingesta flow at two sites:
1. Omasal transport failure (anterior or proximal functional stenosis, reticuloomasal stenosis), which impairs flow of ingesta through the reticuloomasal orifice and occurs with atony of the reticulorumen (often associated with chronic recurrent bloat), or normal to increased ruminal motility.
2. Pyloric outflow failure (posterior or distal functional stenosis, pyloric stenosis), which impairs flow through the pylorus and occurs continuously, or in an intermittent, recurrent pattern (incompletely).
Hoflund's description of the syndrome is convenient for explaining the observed functional defects, but its presumed pathogenesis is not supported by the findings of later investigators..53,146 Later, a classification scheme of four types of vagal indigestion was proposed in which type 1 is associated with a failure of eructation. Animals with type 2 present with bilateral distention of the abdomen as the result of a failure of rumen outflow and fluid accumulation in the rumen. Type 3 manifests similarly to type 2, but the distention is due to a failure of abomasal motility and outflow. Type 4 is a syndrome of partial pyloric obstruction or generalized ileus, not as well defined as the other types.52,53 Unfortunately, this classification scheme is also flawed. Types 2 and 3 in this scheme align well with Hoflund's description, but type 1 can be construed to include all forms of gaseous bloat. Failure of eructation can result from vagal nerve involvement in inflammatory processes in the thorax, but there are numerous other causes of free gas and frothy bloat, most of which are not chronic or associated with animal tissue wasting, characteristic of this syndrome. Type 4 in this scheme is not described in a way that clearly distinguishes it from type 3. Therefore in this text the terms omasal transport failure and pyloric outflow failure are used because they encompass the problems described here as obstructive indigestion.
Similar to the use of vagal indigestion as a descriptor is the use of the term stenosis, which has also led to some confusion, although it was appropriate in its original context. “Functional stenosis” suggested that the defect was a functional one that mimicked a stenosis at the site of outflow. This paralysis or muscular dysfunction can be appreciated in some experimental and clinical cases.
Failure of Omasal Transport. Failure of omasal transport with hypermotility of the rumen is the most common naturally occurring form of the disease. Accumulation of ingesta in the reticulorumen leads to gradually progressive distention of the forestomachs, whereas the omasum and abomasum remain relatively empty. The animal's appetite diminishes as the rumen becomes overfilled, producing one of the most characteristic signs of the disease: inappetence with gross distention of the rumen in the left flank. Continued dilation of the rumen eventually leads to a marked and almost pathognomonic overfilling of the ventral ruminal sac. The rumen assumes an L shape because the ventral sac occupies both the right and left ventral quadrants of the abdomen. The resultant characteristic abdominal contour often is called a “papple” shape (see Fig. 32.128, E) because the left side of the abdomen is distended and assumes the appearance of an apple, whereas the right side assumes the contour of a pear. The reduced passage of ingesta results in low fecal volume. The normal ruminal process of selective retention of fibrous material is disturbed, which causes feces to have increased fiber length and a greasy or pasty consistency. In some cases, feces are firm with large particle size.18,125 Affected animals often continue to drink water, but absorption from the rumen is poor, and the water accumulates in the forestomach while the animal becomes mildly dehydrated. Vigorous contractions of the rumen can be palpated in the left paralumbar fossa in most affected animals, although some display almost complete atony. The contraction pattern does not produce the typical stratification of material in the forestomach; rather, it churns the ruminal contents into a uniform frothy fluid.124,125
The signs just described, with abnormal flow of ingesta and normal or increased forestomach contractions, can be experimentally reproduced by sectioning of the ventral vagal trunk at the cardia and the dorsal trunk just distal to the branching of the ruminal nerves.72 The forestomach distention, empty omasum and abomasum, and stasis of the forestomach with resultant free gas bloat can be reproduced by sectioning of both abdominal vagal trunks along the esophagus. The paralysis produced by vagal denervation can explain the failure of ingesta flow into the omasum by two mechanisms. First, the lower end of the esophageal groove is formed by two muscular lips. These overlap in a manner that allows a passive valve effect that blocks flow into the omasum when they are relaxed or paralyzed. Second, it appears that the flow of ingesta into the omasum is accomplished by an active pumping motion of the omasum that maintains a negative pressure gradient toward the omasum and draws fluid through the reticuloomasal orifice. Paralysis of the omasal musculature after denervation would eliminate the pressure gradient effect. Decreased reticular motility caused by paralysis may contribute to the changes in 124125 ruminal content and the alteration in particle passage.124,125
The most common predisposing cause of naturally occurring omasal transport failure is TRP. Other causes of omasal transport failure include abscesses, adhesions, and peritonitis around the reticulum (especially the right side of the reticulum) or reticuloomasal area without identification of an offending foreign body; hepatic abscesses; diffuse peritonitis; neoplasia of the ruminoreticular fold and esophageal groove; inflammatory disease of the reticular and ruminal walls; papilloma or other mass at the reticuloomasal orifice; herniation of the reticulum through a diaphragmatic defect; or chronic bronchopneumonia in calves. Foreign bodies that physically obstruct the reticuloomasal orifice cause this syndrome and can be identified in exploratory rumenotomy.62 To reconcile the experimental findings with those from clinical cases, Hoflund hypothesized that the development of omasal transport failure resulted from involvement of the vagal trunks in the inflammatory process at the reticulum. Several findings make this an unlikely explanation in most clinical cases94,146:
1. Although sectioning the vagus nerves as described reproduces the syndrome, disturbance of only one of the two trunks still allows normal cyclic contractions in most cases. For a clinical lesion to produce disease development, the vagal nerves would have to be massively involved. In contrast, fewer than a third of examined cases reported show actual lesions in the nerve branches.
2. The ratio of sensory to motor nerve fibers in the abdominal vagi is approximately 9:1, which suggests the important sensory role of the nerve.
3. Inflammatory lesions of the reticuloruminal wall reported in clinical cases are predominantly in the area of important tension receptors that send afferent excitatory impulses to the gastric centers. Induration of the right (medial) wall of the reticulum and in the esophageal groove region may affect intramural nerves and ganglia and reduce the tension receptor activity and therefore the drive for primary cycle activity.
These considerations allow an explanation of some of the inconsistencies found in various cases. Omasal transport failure may occur with insufficient vagal sensory excitation, which in turn reduces excitatory input to the gastric centers, diminishes primary cycle motor drive, and results in paralysis of the omasum and reticuloomasal orifice. Alternatively, substantial reticular adhesions that develop after TRP could prevent normal delivery of small particle ingesta, with fluid consistency, to the reticu- loomasal orifice.124 Because this reduces or abolishes flow into the omasum, both the omasum and abomasum would remain relatively empty, a common finding in these cases. The hypermotility observed in these cases may be the result of secondary rather than primary cycle contractions.20 Distention of the cranial ruminal sac would still be able to induce the secondary contractions if this region is not involved in the induration. Without normal primary cycle activity, the typical stratification of the ingesta would be disturbed, as is usually observed in clinical cases. The existence of hypermotile secondary contractions with absence or severe reduction of primary contractions can be detected clinically. In occasional cases, damage to the thoracic or abdominal vagi by inflammatory or neoplastic lesions may lead to both omasal transport failure and atony of the forestomachs, with resultant free gas bloat. This would be similar to the experimental sectioning of both vagal trunks.
Pyloric Outflow Failure. Failure of pyloric outflow (posterior or distal functional stenosis) causes accumulation of ingesta in the abomasum and omasum. Advanced stages of this form of the syndrome also display gross distention of the reticulorumen. In general, the motility of the forestomach is not markedly affected in the early stages, and normal stratification of ingesta is maintained. With severe distention, forestomach motility is reduced, and the ruminal contents become more fluid.20
Obstructive indigestion may cause no significant blood biochemical abnormalities or can result in severe disturbances of fluid and electrolyte homeostasis. Measurement of the serum electrolyte concentrations provides important clues about the site of obstruction of ingesta flow and is useful in adjusting fluid therapy. When the primary problem is a gradual failure of flow through the reticuloomasal orifice, the rumen fills and grossly distends with fluid but any dehydration tends to be mild, and significant abomasal reflux does not occur. The ruminal fluid maintains a normal chloride content, and affected patients generally show mild or no serum electrolyte abnormalities.18,124 In contrast, overfilling of the forestomach as a result of pyloric outflow failure (internal vomiting) with reflux of high-chloride abomasal ingesta may result in marked dehydration, elevated ruminal chloride concentrations (normal is less than 30 mEq/L), and associated hypochloremic, hypokalemic metabolic alkalosis. In some instances these abnormalities can be dramatic. Prolonged or severe hypochloremia and hypokalemia may also result in paradoxic aciduria associated with avid renal sodium resorption in the presence of low concentrations of chloride and potassium.
Failure of pyloric outflow can be experimentally reproduced by sectioning the ventral vagus trunk at the cardia and the continuation of the dorsal trunk as it crosses the omasum.72 This mimics the usual clinical form of the disease, which is characterized by complete inhibition of flow from the abomasum. Combinations of more distal resections of the nerves produce the syndrome of recurrent atony of the abomasum as it occurs in natural clinical cases. Again, the term stenosis is a misnomer because a true stenosis or spasm of the pylorus is not identified. Rather, the experimental vagal nerve resection and the naturally occurring cases cause a flaccid paralysis, and ingesta accumulates as a result of failure of propulsive activity. The dilation of the abomasum is in the fundus and body and not in the pyloric part.72
A common predisposing cause of pyloric outflow failure syndrome is abomasal volvulus. Other abomasal disturbances, including right and left displacements of the abomasum and abomasal ulceration, can cause the disease as well. After surgical correction of a volvulus, the abomasum remains atonic, and the disease may develop within several days. Clinical signs compatible with obstructive indigestion may arise from gross distention and twisting of the abomasum and lesser omentum, which result in potentially coexisting but distinct injury to the vagal nerves or structural damage to the gastric wall, with or without peritonitis. Although focally extensive vagal nerve lesions have been associated with concomitant vascular damage, which indicates that even with nerve regeneration there may not be a return to normal function, the damage appears reparable in some cases as a return to normal function has been observed.129
Inflammation and adhesions involving the abomasal fundus and reticulum have been associated with pyloric outflow failure in some studies.124 Inflammation of the reticular wall may account for the reticular atony reported in some cases. This form of obstructive indigestion may be more frequently associated with true vagal nerve impairment than appears to be the case in omasal transport failure. Alternatively, reticular adhesions may prevent normal motility, alter the flow of ingesta to the omasum and abomasum, and lead to abnormal filling of the abomasum because of decreased fluidity of abomasal 124
contents.124
Another predisposing cause of pyloric outflow failure is advanced pregnancy with a large fetus. An exact pathogenesis has not been clearly defined. Presumably the large, gravid uterus distorts the positioning of the abomasum or physically compresses and obstructs the anterior small bowel, preventing outflow of ingesta from the abomasum. In affected patients the gravid horn typically occupies most of the space in the omental sling. In support of these conclusions, the problem can be resolved by inducing delivery of the calf or performing a cesarean section. Supportive care may be required for severely affected cows, but the gastrointestinal system returns to normal function, which suggests that it was secondarily affected by the pregnancy. This problem is referred to as a form of obstructive indigestion because it appears as a pyloric outflow failure. Some patients have such severe obstruction of ingesta passage that they may be given the diagnosis of anterior bowel obstruction. This disease has been called indigestion of late pregnancy.
Animals affected with any form of obstructive indigestion for a prolonged time lose body condition because the failure to pass ingesta into the intestinal tract produces a state of malnutrion. The weight loss may be overlooked because of the impression of full body size produced by the abdominal distention, and in these instances a mild to moderate anemia may develop that may be attributable to micronutrient or macronutrient deficiencies.
Chronic Recurrent Bloat. Chronic recurrent bloat is commonly identified with obstructive indigestion in any of its forms. It is mild to moderate in severity, commonly waxes and wanes, and adds to the visual impression of gross abdominal distention. The pathogenesis of this ruminal tympany varies. Experimental resection of both abdominal vagal trunks stops eructation by causing complete forestomach stasis. In naturally occurring cases in which lesions of the vagal nerve truly inhibit motor impulse transmission, bloat may arise from this mechanism. When vagal nerve damage does not appear to be involved, other mechanisms may explain the bloat (see Table 32.17). Overfilling of the reticulorumen with frothy ingesta, a common finding, can inhibit the cardia dilation reflex that is a prerequisite of eructation. Gross distention of the forestomach can also weaken the contractile ability of the rumen, so that the contractions are not strong enough to clear the cardia before eructation.
Bradycardia is often identified in association with obstructive indigestion but can also occur with other forestomach diseases. The origin of the vagotonia is unclear. When vagal nerve lesions are present distal to the cardiac innervation, reflex excitatory discharges may cause bradycardia. Naturally occurring obstructive indigestion shows bradycardia as a feature in only a third or fewer of the cases.18 These variations may exist because the experimental and natural cases have different causes or because the disease varies in duration. Once the forestomach
■ TABLE 32.17
Causes of Rumen Tympany (Bloat)
| Mechanism | Cause | Disease Examples |
| Obstruction of eructations | Esophageal obstruction Cardia obstruction Failure to clear cardia of fluid or ingesta | Choke, tetanus, thoracic inflammation or neoplasia with swollen mediastinal lymph nodes Papilloma, fibroma, actinobacillosis Lateral recumbency, reticulorumen overfilled with ingesta (as in vagal indigestion, ruminal microbial inactivity with poorly digestible roughage, obstruction of the reticuloomasal orifice) |
| Ruminal motor | Gas trapped in stable foam | Frothy bloat |
| dysfunction | Failure of smooth muscle contraction Weakened muscle contraction | Hypocalcemia Chronic ruminal distention with indigestible roughage, outflow obstruction, or vagal indigestion; hypokalemia |
| Chemical | Abomasal distention | Displaced abomasum (especially in calves) |
| inhibition | Vagus nerve damage Ruminal stasis | Thoracic inflammation (especially in calves and with neoplasia) Rumen acidosis, rumen alkalosis, abnormal fermentation products with simple indigestion |
has become severely distended, the heart rate tends to be elevated, probably as a result of pain and discomfort and deterioration of hydration and cardiovascular parameters.
Obstruction or the Cardia or Reticuloomasal Onhce. True mechanical obstruction of the forestomach is an uncommon occurrence. The obstruction can be either full or partial and occur at either the cardia or the reticuloomasal orifice. The inflammatory and neoplastic conditions described previously can appear to be obstructive indigestion when the tissues are sufficiently distorted and lesions involve one of these orifices. Papillomas are most prone to causing an obstruction when they become pedunculated. A variety of foreign bodies create obstruction. In calves, trichobezoars are most commonly the cause, occurring predominantly in animals on a low-roughage diet that consequently lick their hair coats vigorously. In adult cows, ingestion of the placenta occasionally results in an obstruction. Curious ruminants, especially goats, sometimes consume plastic bags or discarded rectal palpation sleeves. These and other nondegradable materials can lead to obstruction even after considerable time has passed.
Cardia obstruction leads to the signs typical of esophageal obstruction, with free gas bloat as a prominent, perhaps lifethreatening development. Obstruction of the reticuloomasal orifice produces the classic syndrome of obstructive indigestion. Failure of ingesta flow beyond the rumen results in accumulation of fluid material in the forestomach and diminished or no passage of ingesta through the intestines. The degree and duration of obstruction determine the severity of associated problems such as dehydration, depression, elevated heart rate, forestomach stasis, colic, and muscular weakness. Only rumen- otomy can effectively differentiate these obstructive diseases from other problems with similar signs.69 Removal of pedunculated masses or foreign bodies at the reticuloomasal orifice can promptly correct such problems.
Diaphragmatic Hernia. Defects in the diaphragms of cattle are uncommon. Most cases involve a tear through which the reticulum can herniate. Other abdominal organs may also be involved if the rent is large. The diaphragmatic defect may be congenital or an acquired lesion caused by a local inflammatory process (TRP), sudden external trauma (fighting, hanging up on a fence), or internal pressure (parturition, acute tympany).92 Entrapment of the reticulum may lead to acute changes in intrathoracic pressure and cause sudden dyspnea, tachycardia, and poor venous return to the heart. In general, however, this reticular problem causes the classical syndrome of obstructive indigestion with omasal transport failure.43 Failure of flow through the reticuloomasal orifice may result from vagal nerve damage, or the anatomic distortion alone may explain the motility defect. Entrapment of the reticulum hinders normal reticular movements and distorts the esophageal groove and reticuloomasal orifice. Reticular ingesta can be heard moving inside the thorax, therefore complete reticular paralysis is unlikely to be the problem. Motility disturbance is reflected by hypermotility of the rumen, generation of frothy ingesta, persistent or recurrent moderate tympany, and overfilling of the rumen. Signs of pain may also be present, as in cases of TRP. Rumination usually is impaired, some affected animals develop a megaesophagus, and large volumes of ingesta may be vomited, especially after eating. Surgical correction of a diaphragmatic hernia involving the reticulum can be attempted but has usually proved unrewarding, especially if the lesion is chronic, involves a large defect, or is accompanied by inflammatory reaction.
Indigestion of Poor-Quality Roughage. Ruminants fed roughage of extremely low quality, without supplemental nutrition, may develop prolonged inactivity of the rumen microbial flora. Many such animals simply fail to thrive and develop protein energy malnutrition, and some may develop specific nutrient deficiencies. This feeding pattern induces a form of indigestion, described later as one of the disorders of fermentative function. However, it is mentioned here because the extreme cases, seen as “Haybelly,” appear as obstructive indigestions. When the fibrous feed that is not adequately fermented accumulates in the forestomachs at an excessive level, affected animals show the typical signs of obstructive indigestion syndrome, including gradually progressive gross abdominal distention, body tissue loss, reduced fecal passage of abnormal feces, and sometimes chronic recurrent free gas bloat. This condition can be differentiated from other cases of obstructive indigestion by ruminal palpation that reveals very firm and uniform rumen contents, history or observation of the feeding regimen, and rumen fluid analysis described later.
Treatment of and Prognosis for Obstructive Indigestion. Obstructive indigestion is a chronic and insidious problem that generally warrants a guarded to poor prognosis. The syndrome of abdominal distention with an L-shaped rumen and possibly ruminal tympany has several different causes. Exploratory laparotomy and rumenotomy are essential for establishing an accurate assessment (see Fig. 32.128).99 The two most common causes of obstructive indigestion syndrome are inflammatory lesions of the reticuloomasal region and abomasal diseases that involve gross distention, twisting, or vascular impairment of the organ. Obstructive indigestion caused by abomasal disease carries a poor prognosis, whereas the prognosis for cases with reticular involvement is more
■ BOX 32.5
Principles of Treatment of Obstructive (Vagal) Indigestion
1. Determine likely cause, often by means of exploratory laparotomy.
2. Administer specific therapy (e.g., give antibiotics or antiinflammatory agents, remove foreign body or relief of obstruction, drain abscesses) for causative lesion.
3. Relieve forestomach distention; this often must be performed repetitively.
4. Limit feed and water intake; feed palatable, high-fiber rations.
5. Transfaunate.
6. Cannulate rumen if chronic bloat (free gas) is a problem.
variable. Animals in either category may respond favorably with appropriate therapy124,129 (Box 32.5). Surgical exploration not only allows an assessment of the cause of the problem but may also allow repair. When abscesses are identified at the reticulum or liver, surgical drainage may help resolve the forestomach motor disturbance.124 Identification of adhesions and active inflammation indicates that broad-spectrum antibiotic therapy may be beneficial, and as a preventive practice, some clinicians have advocated aggessive antimicrobial therapy before and after the surgical correction of a right-sided abomasal displacement or volvulus.129 Gross abomasal distention, which indicates pyloric outflow failure, usually worsens the prognosis, as does the presence of granulomatous or neoplastic processes or generalized peritonitis and adhesion formation.124 When the presence of a large gravid uterus appears to be the inciting cause of outflow failure, parturition or cesarean section usually resolves the problem completely.
The evaluation of animals with obstructive indigestion with a large fluid-filled rumen should include assessment of the fluid and electrolyte status. Abnormalities such as dehydration, hypocalcemia, hypochloremia, and hypokalemia should be addressed with supportive fluid therapy. Treatment should be administered parenterally because oral treatments are ineffective or deleterious. The forestomach should be emptied of the excessive ingesta accumulation either during surgery or with a large-bore stomach tube. This procedure may have to be repeated if the recovery period is prolonged. Relief of persistent forestomach distention is crucial for the reestablishment of normal motility. Limited feed and water should be offered to prevent repeated accumulations in the reticulorumen, and intravenous fluid therapy should be continued until reticulo- ruminal motility is reestablished and oral fluid intake can be allowed at normal levels. Once the ruminal distention has been alleviated, several liters of ruminal fluid transfaunate from a healthy donor should be administered.122 The limited diet must be palatable and should consist primarily of long-stemmed hay or green feed for maximum stimulation of the normal forestomach motility pattern. A temporary rumenostomy may be indicated if tympany is a prominent sign.26
Response to treatment of obstructive indigestion usually is a slow process and may take several weeks. Favorable signs include a return of the normal primary and secondary contraction patterns, improvement in appetite, maintenance of normal forestomach dimensions, weight gain, and increased fecal production. Repeated development of forestomach distention, continued scant fecal output, poor ruminal motility, and recurrent bloat are indications that the animal is not responding to treatment, and the prognosis is grave.
FREE GAS BLOAT. Accumulation of free gas in the dorsal rumen should not be considered a primary disease entity but rather a sign of disease (see Table 32.17). However, because free gas bloat often is the most prominent sign and because it accompanies several different forms of indigestion, its pathogenesis is reviewed briefly here.
Ruminal microbial fermentation and neutralization of acids by salivary bicarbonate continually produce gas as an end product (primarily methane and carbon dioxide) in proportion to the rate of fermentation. Normally the ruminant can eructate volumes of gas that exceed the amount produced even at maximum rates of fermentation.9 Thus an excessive production of gas is not the cause of bloat. Bloat develops either because the evacuation of gas is limited by a physical obstruction or because the mechanisms that expel the gas are inhibited.28
As in choke, physical obstruction of the esophagus by a foreign body can produce dramatic and peracute bloat. Other forms of esophageal occlusion (which may additionally involve inflammation of nerves or ruminal muscle malfunction) include muscular spasm (as in tetanus), swollen mediastinal lymph nodes (as in chronic pneumonia or thymic lymphosarcoma), and tumorous or inflammatory swellings of the cardia region (as in papilloma or actinomycosis). These problems tend to show that bloat has a progressive or chronic nature, although the degree of bloat may be marked.
Bloat is a common feature of indigestions caused by microbial fermentative disorders. When ruminal hypomotility occurs, the fermentative rate may decline, but weak ruminal contractions may be inadequate to move the gas layer and to clear the cardia preparatory to eructation. Thus dietary, microbial, or metabolic factors that affect the excitability of the gastric centers or the reticulorumen can result in bloat. Ruminal stasis can result in bloat because eructation occurs only with ruminal contraction. Bloat also accompanies indigestions that produce gross distention of the reticulorumen with fluid or solid ingesta (i.e., obstructive indigestion, ruminal acidosis, and microfloral inactivity caused by indigestible roughage). The cause of bloat in these cases may be a combination of ruminal stasis, weakening of the ruminal wall caused by the gross distention, and failure to clear the cardia.
As is the case in adult cattle, it appears that free gas bloat in calves has numerous causes, including fermentative indigestions, ruminal wall disturbances, and esophageal involvement in an intrathoracic inflammatory process.45,86 Chronic bloat in calves has also been attributated to a form of vagal nerve damage resulting from mediastinal inflammation, often caused by lymphadenopathy as a consequence of pneumonia. Distinguishing between vagal nerve impairment and esophageal compression or inflammation as the cause of free gas bloat requires a thorough assessment of ruminal motor function.
When ruminal tympany is a prominent sign, it necessitates very critical assessment. Frothy bloat and free gas bloat can be differentiated by a thorough physical examination and knowledge of the feeding history. Passage of a stomach tube to help in this differentiation is very important and may alleviate the acute problem if free gas is present (see Table 32.15). Evidence of respiratory or cardiovascular distress indicates that the bloat is an acute, life-threatening problem that necessitates emergency treatment. With the exception of cardia or esophageal obstruction, the free gas bloat associated with indigestive disturbances is mild to moderate in severity and chronic or recurrent in nature. It does not represent a major threat to the animal and can be handled by treating the primary forestomach disturbance. Chronic free gas bloat does not respond to the antifermentatives or surfactants commonly used for frothy bloat. Only the restoration of physiologically normal reticuloruminal function corrects this type of bloat.
Inhibition of eructation caused by lesions of the cardia region can usually be confirmed only by exploratory rumenotomy. This approach also determines whether the lesion is surgically correctable. Inflammatory lesions may respond to long-term administration of broad-spectrum antibiotics. This is also the treatment of choice when chronic pneumonia appears to be the cause of the bloat. Failure to respond within approximately 3 weeks suggests that the treatment is not effective, and slaughter should be recommended after an appropriate withdrawal time. Detection of abnormal forestomach ingesta should direct treatment to the primary fermentative or feeding disorder.
The various causes of chronic or recurrent bloat usually necessitate chronic treatment for correction. It follows that the bloat also does not completely resolve until the underlying disturbance is corrected. Repeated relief of the bloat may be accomplished by passage of a stomach tube during the treatment regimen. In many cases this proves too tedious or too traumatic for the animal, and the most viable alternative often is the establishment of a temporary rumenostomy.26 Several devices are manufactured for this purpose, or the rumenostomy can be created by suturing the rumen to the skin. Release of the fermentative gas in this manner is important for the reestablishment of normal forestomach motility, which is inhibited if distention is extreme. When free gas bloat is the result of an obstruction of eructation or another gastrointestinal tract disease such as abomasal displacement, surgical treatment of the primary problem may be necessary. The tympany responds rapidly in these cases, and rumenostomy and cannulation are not required.
Signs such as ruminal tympany, ruminal hypomotility or stasis, and forestomach distention can all result from a number of causes. Ruminal hypomotility, for example, is commonly a physiologic response to problems such as abnormal ruminal contents, a ruminal wall lesion, pain, or overdistention. In many cases the ruminal motility disturbance serves as a protective role for the animal. Former treatments that were directed at stimulating ruminal motility without addressing the causative disturbance included rumenatorics (i.e., nux vomica, ginger, tartar emetic) or parasympathomimetics (i.e., neostigmine, carbamylcholine). Such agents are not indicated under these circumstances. Likewise the treatment of indigestions with alkalinizing agents such as magnesium hydroxide is indicated only when the pH of ruminal contents is low.
Disorders of Reticuloruminal Fermentive Function
FORESTOMACH MICROBIAL POPULATION. The continuous culture system of the rumen involves an ongoing selection of microorganisms best adapted to grow in a variety of ecologic niches that are in a dynamic state. Numerous control mechanisms govern the environment and the resultant microbial population. Some of these mechanisms are related to the animal itself, such as salivation, mixing and rumination, removal of substances by absorption or diffusion, outflow through the reticuloomasal orifice, and eructation. Others are related to the diet, including nutrient quality of the substrate (feed), balance of required elements, solubility, particle size, presence of inhibitory substances, nutrient quantity, and rate of delivery to the rumen. Control of fermentation (see Box 32.4) also results from microbial interactions such as competition and symbiosis: cross-feeding between species, removal of inhibitory end products, and maintenance of the oxidation-reduction potential. The complexity of the system tends to promote an overall stability. Changes in the controlling factors create selective pressures that lead to population changes in the rumen.100,155
The rumen contains large numbers of bacteria, ciliated protozoa, anaerobic ruminal fungi, and bacteriophages.100 Ruminal bacteria are predominantly anaerobes, with some coexisting facultative anaerobes. Although the facultative organisms are not important in normal ruminal function, they may be associated with some forms of ruminal dysfunction. Some microbes ferment the primary nutrients in the feed such as cellulose, hemicellulose, pectin, starch, and simple sugars. Other species ferment the products from the primary nutrient fermentation such as pentoses, glucose, lactate, succinate, and formate. Many species are very specialized and have numerous growth requirements that may be supplied by the general fermentation. Other microbes are important for their role in removing end products and cycling essential factors back to the other organisms.71,101,155
EFFECTS OF FEED CHARACTERISTICS. The concentrations and proportions of the microbial species vary with the composition of the diet (Table 32.18). An abundant supply of a certain substrate tends to favor a microbial population with a predilection or high capacity for utilizing that material. The most important factors in the rate of digestion are the properties of the carbohydrates and protein in the feed. High-protein diets favor proteolytic organisms, whereas high-starch, low-fiber diets favor amylolytic bacteria.111 Cellulolytic bacteria are prominent in a high-fiber diet, but their numbers also depend on the fiber size as this factor determines the rate of passage or retention in the forestomach. Cellulolytic species can be abundant with a high-concentrate diet if some long-stemmed roughage is included because the retention time of the fiber is prolonged. Diets with readily fermentable carbohydrates and low fiber favor species capable of rapid metabolism and tolerant of low pH. Acid production is rapid, and populations of microbes less tolerant of such changes decline.85,101,144
■ TABLE 32.18
Effects of Feed Characteristics on Ruminal Digestion and Health
| Feed | Rumen Content | Effect on Health |
| Primary forage of high-quality, long fiber length, crude fiber > 18% of dry matter; with concentrate supplement at 20% to 50% of total intake, moderate protein level | pH, 5.5 to 7 VFA, 60 to 120 mmol/L Acetic acid level > propionic acid level > butyric acid level | Normal, healthy, productive |
| Excessive forage of low nutrient value | pH, 6.5 to 7 | Poor production or growth, microfloral |
| (late cut) with little concentrate or | VFA, decreased | inactivity and rumen impaction, |
| protein supplementation | Microbial activity, decreased | malnutrition caused by protein, energy, mineral, and vitamin deficiency |
| High level of concentrate feeding (>60%) | pH, 5 to 6.5 | High production, rapid growth; possible |
| with decreased forage or fiber length | VFA, increased Microbial activity, increased | chronic rumen acidosis, milk fat depression, chronic laminitis, ketosis, ruminal parakeratosis, excessively fat condition |
| Extremely high level of concentrates (especially with sudden exposure to ration), low intake of forage | pH, 4 to 5.5 VFA, increased Lactic acid level, increased | Acute ruminal acidosis |
| Normal levels of forage intake, concentrate with very high protein or NPN supplementation | pH, 6.5 to 7.5 VFA, decreased Ammonia level, increased | Ruminal alkalosis, possible urea toxicity |
NPN, Nonprotein nitrogen; VFA, volatile fatty acid.
The microbial population is also influenced by the limits of supply of certain feed substrates.154 High rates of fermentation and microbial growth on the abundant substrates depend on sufficient amounts of the more limited nutrients. Optimum carbohydrate use requires adequate sources of nitrogen, sulfur, and essential mineral nutrients.46 When any essential nutrient is deficient, the rate of digestion and thus the digestibility of the feedstuff decrease. The presence of signs of nutrient deficiency or forestomach dysfunction with microbial and forestomach inactivity depends on the limiting nutrient and relative requirement of the host and bacteria for the nutrient. Substances and conditions that inhibit fermentation further reduce digestibility.
The feed material also affects ruminal fermentation by influencing the rate and extent of digestion and passage from the reticulorumen. Grains vary in average starch content; corn and sorghum contain the most starch (71 to 76%), followed by wheat (62 to 65%), barley (57 to 59%), and oats (44%).117 Each grain also has unique features related to the protein matrix surrounding the starch, and the total quantity and rate at which starch molecules are converted to ruminal VFAs, lactate, and and gas are determined by the interaction of starch content, grain processing method, and degree of processing.107 Fine grinding and pelleting of feed increase the rate of passage of the particulate matter from the reticulorumen. Very finely ground rations also reduce the stratification of fibrous material in the rumen. This affects the ability to sort material in the rumen selectively by particle size and density, so that larger particles less thoroughly fermented pass more readily into the lower bowel. Microbes associated with the feed particles are passed out of the rumen with the feed. Thus a faster rate of passage competes with the generation time of the organisms. Populations of slower growing microbes tend to be most influenced by changes in the retention or passage times. Slow- growing cellulolytic bacteria decline in numbers as the passage rate increases (retention time decreases). High passage rates usually produce faster digestion rates. Although these factors are primarily important to the feed efficiency of the animal, they also affect ruminal function and the adaptation of microbes to feeding changes.155
Adaptation of the microbial flora to dietary changes may require a week or longer.51,65 The abruptness of a dietary change determines the degree of alteration of the ruminal microbial population and fermentation pattern and the potential for digestive disturbances. With abrupt and dramatic shifts to higher carbohydrate diets, the facultative species may overwhelm the more normal flora by producing excessive acid and lowering the pH. The importance of microbial adaptation to a particular diet is evidenced by the reduction in forestomach disturbances seen when the rumen is inoculated, before a feeding change, with fluid from animals already adapted to the new ration.51,150
The end products of microbial fermentation influence not only the microbial population but also ruminal function. High concentrations of nondissociated VFAs excite sensory epithelial receptors that reflexly inhibit ruminal motility. Ruminal stasis occurs if a sudden increase in concentrate feeding induces lactic acid fermentation. The ruminal pH suddenly declines, and a greater proportion of the VFAs shift to the nondissociated state with the degree of ionization governed by the rumen pH and the logarithmic acid dissociation constant (pKa) of each particular acid.35,111 A consistently high level of concentrate feeding produces rapid fermentation, a high concentration of VFAs, and low pH, and the nondissociated VFA level may reach the threshold for stimulation of the inhibitory epithelial receptors. The ruminal stasis reduces the fermentation rate. Mild cases of ruminal acidosis may show spontaneous recovery of ruminal functions as the absorption of VFAs reduces the concentrations to a noninhibitory level. With more severe ruminal acidosis, the generation of acid continues despite the ruminal stasis, giving rise to more severe complications of the disease.
In some instances the effects of ruminal microbial metabolism and microbial end products extend beyond impacts on nutritional status and digestive system function. Several ruminant diseases are due to rumen-generated toxic effects. These have extremely variable manifestations and include toxicoses from ammonia, nitrate and nitrite, 3-methylindole, dimethylsulfide (Brassica spp., onion toxicity), and sulfur-associated polioencephalomalacia.36,63,130,133
In summary, excesses, deficiencies, or rapid changes of feed substrate can cause imbalance in the microbial population and the fluid milieu. The result can be bacterial overgrowth and overproduction of microbial end products or insufficient microbial growth and fermentation. The effects of these abnormalities on animals range from ruminal motility dysfunction to poor growth and performance and to outright toxicity and organic damage.
INACTIVITY OF RUMINAL MICROBIAL FLORA (CAUSED BY POOR-QUALITY ROUGHAGE, HAYBELLY, OR RUMINAL IMPACTION). When ruminal microbial flora inactivity occurs, the microbial populations and their metabolic and fermentative processes are diminished as a result of deficiencies of one or more nutrients. This occurs most commonly with poor-quality roughage deficient in protein and readily digestible carbohydrates (late cut, highly lignified hay or straw). Microfloral inactivity can also occur when specific mineral nutrients are deficient or when inhibitory substances such as antibiotics or some plant products are present in the feed.155 Microfloral inactivity also occurs with prolonged anorexia, which abolishes the intake of all nutrients and is the primary pathogenesis of many cases of secondary indigestion.21,41,79
When microbial digestive processes decline, the breakdown of ingested feedstuffs is prolonged. Failure to reduce the particle size of the ingesta leads to a prolonged retention in the forestomach and gradual accumulation of the undigested feedstuff. Gradual distention of the reticulorumen is commonly observed (haybelly). In extreme cases, this produces the signs of obstructive indigestion. Forestomach distention can result in weak contractions and moderate recurrent tympany. Ruminal hypomotility alters the normal stratification of the ruminal contents, and the fibrous components are found mixed in the fluid or compacted ventrally on the ruminal floor. Abnormal passage of ingesta from the forestomach results in decreased fecal passage, and the feces usually are dried and contain undigested plant fibers. Other effects on animals are those of generalized or specific nutrient deficiencies (e.g., decreased growth or production, ketosis, emaciation, and a poor hair coat). When anorexia is the cause of the microbial inactivity, the ruminal fill decreases and the lack of normal distention also induces ruminal stasis.43
ACUTE SIMPLE INDIGESTION. Acute simple indigestion is the most common sequela of an abrupt change in the ration. Such feed changes present the ruminal microflora with nutrient substrates (1) to which they are not metabolically adapted, (2) to which they are adapted but in lesser quantities, or (3) that contain or produce substances that inhibit microbial growth and fermentation. The result is an imbalance in the microflora and its fermentation products. The difference between this problem and some of the other fermentation disorders is mostly a matter of degree. In general, this disease is relatively mild and self-limiting. Most affected animals show anorexia for 1 to 2 days, develop diarrhea in approximately 24 hours, and return to a normal appetite without treatment when the ruminal fermentation has stabilized and inhibitory substances have been eliminated. Ruminal motility is reduced but usually not absent, the filling of the rumen is not remarkably altered, and bloat, if it occurs, is mild. In some cases the ruminal fluid pH may change, but usually not dramatically. Mild acidosis or alkalosis of the ruminal fluid may develop, depending on the nature of the causative feedstuff and its resultant fermentative degradation. Signs of ruminal microfloral inactivity are common. Simple indigestion is an acute problem, in contrast to the microfloral inactivity discussed in the previous paragraphs, in which deficiencies produce microfloral inactivity over prolonged time.
Feeds commonly implicated as causes of simple indigestion include moldy or overheated feeds, frosted forages, and partly fermented, spoiled, or sour silages. This form of indigestion also occurs in animals fed high-quality feed, usually after an increase in the rate of feeding or after a change of one of the feed constituents. Thus these mild forms of indigestion can range from a mild acidosis to an excess of VFAs and to the generation of some bacterial inhibitory products. Because the rumen and its fermentative bacteria are very adaptable, the ways, if any, in which animals given a certain feed experience the problem vary considerably. It is not unusual to observe only one or several animals from a group on the ration may have signs.
ACUTE RUMINAL LACTIC ACIDOSIS (GRAIN OVERLOAD, TOXIC INDIGESTION). The various forms of indigestion may be manifested as acute, subacute, or chronic illness. In general they do not appear as critical emergencies with fulminating systemic signs and life-threatening conditions. The exceptions to this are frothy bloat and acute ruminal lactic acidosis. Acute ruminal acidosis is the most dramatic of the forms of ruminal microbial fermentative disorders and in some cases is lethal in less than 24 hours. It has also received the most research attention; therefore the events in its pathogenesis are more clearly defined than those of the other forestomach disorders. The condition has been known as lactic acidosis, acute ruminal impaction, ruminal overload, acid indigestion, toxic indigestion, grain engorgement, grain overload, and D-lactic acidosis.
Cattle examined a few hours after engorgement of grain may yet be alert but anorexic with a mildly distended rumen, weak ruminal contractions, and mild signs of colic. If the acidosis is mild, affected cattle show the signs of indigestion discussed previously and with or without treatment may recover their appetite within a few days. The severe form of this indigestion leads to severe systemic involvement, with depression, severe dehydration, weakness, recumbency, profuse diarrhea, and eventually death. The temperature usually is normal to subnormal. The heart rate elevates with the progression of dehydration and systemic acidosis; rates above 100 beats/min are usually associated with a poor prognosis. Respiration generally is increased (60 to 90 breaths/min) and shallow. The rumen accumulates fluid. Animals capable of rising may show a staggering gait and appear blind. The pupillary light reflex may be slower than normal. Recumbent animals usually lie quietly and may be stuporous. As the cardiovascular system becomes more severely affected with increasing dehydration and acidosis, the extremities become cool, and mucous membranes dry. Anuria may follow poor renal perfusion. Rapid progression of signs leading to recumbency bespeaks a poor prognosis, and affected animals may die within 24 to 72 hours. Therefore if the progression of signs is rapid, emergency therapeutic measures are mandatory.
Acute ruminal lactic acidosis is the result of excessive consumption of readily fermentable carbohydrates, which causes a rapid fermentation with production of lactic acid and a decrease in ruminal pH to physiologically inappropriate levels. This occurs when animals consume an excess of concentrate feeds (e.g., if animals are suddenly exposed to the feeds without prior adaptation; if animals already on such feeds suddenly consume an excessive quantity because of accidental access; or if animals that have been off feed return to feed and are offered unrestricted access to concentrates). The problem is more common when animals are grouped than when they are separate, probably because the psychological aspects of competition induce them to overconsume. In general the feeds involved include the cereal grains commonly used in high production rations and fruit and root crops (e.g., feed beets, sugar beets, potatoes) where they are available. Starch and soluble sugars promote an overgrowth of bacteria that produce glucose and organic acids. The acid end products increase ruminal acidity and osmolality, inhibit or destroy other ruminal microbes, and cause forestomach dysfunction and metabolic disturbances.93,111,119,132
Dramatic alterations of the blood biochemical characteristics may accompany severe ruminal acidosis. Usually the laboratory findings correlate with the degree of severity assessed on physical examination. Affected animals have metabolic acidosis with decreased blood pH and plasma bicarbonate. Blood lactate levels rise with the acidosis. The urine pH falls into the acidic range as the kidneys excrete some of the excess acid, but eventually severe dehydration results in renal failure and anuria, eliminating this route of acid excretion. Decreased renal function is reflected by elevated serum creatinine and urea nitrogen concentrations. Other findings commonly include increased serum phosphate concentration, possibly caused by massive cellular destruction, and mildly decreased serum calcium concentration, presumably the result of decreased gut absorption. Other serum electrolyte abnormalities, such as changes in the sodium and chloride concentrations, may reflect fluid balance changes in response to ruminal fluid hyperosmolality (a third space phenomenon).132 Concentrations of serum enzymes of muscle and liver origin rise when acidosis and dehydration produce cardiovascular impairment with poor tissue perfusion, increased recumbency, and cellular destruction. Portal bacteria and toxins from the damaged ruminal mucosa contribute significantly to the increased serum liver enzymes: aspartate aminotransferase, sorbitol dehydrogenase, (orthinine carbomyltransferase), and γ-glutamyl transferase.
Specific characteristics of the feedstuffs contribute to acidification of the ruminal fluid. Cereal grains inherently possess less buffering capacity than do the fibrous forages. Low structured fiber content and decreased forage particle size induce less salivation during ingestion and less rumination subsequently; therefore salivary buffering declines when concentrate feeds are consumed. Some silages contain both high carbohydrate and lactic acid and thus introduce more acid at both ingestion and fermentation.55,88,119
Feeding regimens that include significant fibrous roughage limit carbohydrate availability and rates of microbial fermentation and growth. Carbohydrate fermentation efficiency relative to the amount of ATP derived from each sugar provides competitive survival value. Slower growing cellulolytic bacteria use substrate most efficiently. When starch or sugar is available in excess, the faster growing species such as S. bovis metabolize carbohydrate faster and produce more ATP per unit time, even though they are less efficient in ATP production per carbohydrate molecule. Under these conditions they can overgrow, and lactic acid is their end product.119
The severity of ruminal acidosis and disease signs vary considerably, depending on the amount and type of carbohydrate-rich feed consumed and the degree of prior ruminal microbial adaptation to the carbohydrate substrate. The disease can range from a mild form of indigestion to an overwhelming toxemia that may be difficult to distinguish from other acute toxic conditions or various diseases with endotoxemia.
If consumption of fermentable carbohydrate is only mildly excessive, S. bovis proliferation decreases when the carbohydrate has been fermented, pH rises toward normal, and the efficient fermenters reestablish dominance. If the carbohydrate source is abundant and its supply is not exhausted, the acidosis becomes more severe. Continued production of lactate by S. bovis reduces the fluid pH to the range of 5 to 5.5, and the ruminal fluid osmolality rises concurrently. Both these factors inhibit or kill the ruminal protozoa, which normally use starch and small sugars and help limit increasing lactic acid levels. There are also numerous species of lactate-using bacteria, of which Megasphaera elsdenii and Selenomonas ruminantium are the primary examples. These bacteria, which increase in numbers when animals slowly adapt to a high-concentrate diet, are eliminated by abrupt changes and generation of excessive acid; therefore lactate use decreases when the acid is generated too quickly.51,119
The lactobacilli are the major group of lactic acid producers in the rumen. The increasing acidity of the fluid enhances the growth of these organisms. Because the lactate-using bacteria are killed off before the lactobacilli overgrow, their diverse end products are unavailable as substrate for other bacteria. The lactobacilli are left as the predominant organisms to use the available carbohydrates. Even the S. bovis organisms that began the lactic acid production are inhibited below a pH of 4.5, leaving the lactobacilli, as the most acid-resistant species, to generate more lactic acid.111,156
The acidification of the fluid milieu enhances the lactic acid production by altering microbial metabolism.119 The loss of the fluid bicarbonate buffer and the increase in available hydrogen ions block the conversion of lactate to propionate even before the lactate users die off. Also, when the pH is above 5 but declining, ruminal fluid amylase activity increases and liberates more free glucose from starch. However, glucose use is reduced, and ruminal glucose accumulates. Apparently the lactate-using bacteria such as S. ruminantium degrade less lactate to acetate in the presence of increased glucose concentra- tions.,1, Thus not only does the microbial population change but also the characteristics of the fluid accelerate the lactic acid production when the available carbohydrate is excessive.119
The effects on the animal from the ruminal fluid changes are numerous and detrimental. In the early stages of the acidic fermentation, the VFAs are produced in abundance. Although VFA production decreases as the microbes are increasingly inhibited, VFA concentrations remain elevated in advanced acidosis. The VFAs are much weaker acids than lactic acid; thus as pH drops, they accept hydrogen from lactic acid and serve as buffers in the fluid, so that a greater proportion of the VFAs exist in the nondissociated state. This form is more readily absorbable than free ions through the ruminal wall. During absorption some VFAs undergo metabolism by the ruminal wall epithelium, which results in the release of lactate and ketone bodies into the circulation. Excessive absorption of the VFAs leads to systemic acidosis, and circulating lactate and VFAs may also directly damage the liver. In addition, the high concentration of nondissociated VFAs at the ruminal epithelium provides a strong inhibitory effect on reticuloruminal motility and leads to ruminal stasis. This effect tends to protect the animal because it reduces the absorption of detrimental fermentation products from the rumen.36,63,93,119,130,133
The osmotic pressure of the ruminal fluid increases as lactic acidosis develops.55,93,119 In a normal animal, ruminal osmolality remains relatively constant at approximately 280 mOsm/L, but osmolality may double in some cases of acute acidosis. Lactic acid accounts for a major fraction of the increase, but some of the components of this change remain unidentified. The increased osmolality inhibits and kills some of the microflora and draws fluid into the rumen, mostly from the extracellular compartment. This accounts for the increased ruminal fluid volume, ruminal distention, and severe dehydration observed clinically. The loss of circulating fluid volume leads to circulatory impairment, decreased renal blood flow and glomerular filtration, and in some cases leads to anuria. Poor peripheral circulation results in hypoxic metabolism and contributes to systemic acidosis.
Although it has been assumed that the systemic acidosis that develops with this disease is attributable to lactic acid absorption from the rumen, such absorption does not appear to occur readily.119 Lactate is absorbed from the rumen at a much slower rate than are the VFAs because it is highly ionized at a pH near physiologic normal, which tends to inhibit absorption. At lower pH the rumen becomes static, thereby also inhibiting absorption. The hypertonicity of the ruminal fluid further limits absorption of lactate and other substances.132 It appears that the peak entry of lactate into the circulation occurs in the early phases of the disease. Some lactate may be absorbed from the intestinal tract from fluid passed before the onset of complete stasis. Many experimental trials have not shown the development of severe systemic acidosis in the early phase of the disease. It may be that a large component of the later severe systemic acidosis is attributable to circulatory insufficiency rather than to absorption of lactic acid.
Some absorption of the lactic acid does occur, however, as evidenced by the appearance of D-lactic acid in the circulation. Microbes produce both the levorotational (L) and dextroro- tational (d) forms of lactic acid, whereas animal tissues produce only L-lactic acid.111 The animals’ pathways for metabolism of D-lactic acid are not as efficient as those for L-lactic acid; therefore absorption of both forms leads to an accumulation of predominantly D-lactate in the animals’ system.98 The lactate is eliminated by oxidation, gluconeogenesis, and renal excretion. An animal’s hydration status, liver and muscle metabolism, and renal function determine how rapidly it can eliminate excess lactate. Animals that survive ruminal acidosis often have metabolic alkalosis after the acidotic phase, as a result of lactate metabolism and production of bicarbonate.
Lactic acid is a strong corrosive agent that can destroy the ruminal epithelium, giving rise to the name toxic rumenitis. The increased ruminal fluid osmolality also damages the epithelium as extracellular water influx across the epithelium occurs in response to osmotic pressure imbalance and disturbed Na transport.132 The effects of epithelial destruction can be far-reaching because the damage persists after resolution of the acute acidosis.55,91 Some yeast and fungi that are resistant to the high acidity readily colonize the damaged sites, invade the vasculature, and cause thrombosis or spread to the liver and other organs.30 Ruminal acidosis is considered one of the primary causes of mycotic rumenitis (discussed earlier in the Reticulitis and Rumenitis section) and mycotic omasitis, although other predisposing causes have been identified.30,76 Bacterial rumenitis can also result from the chemical damage and may lead to abscess formation, diffuse cellulitis, or perforation and peritonitis. If the animal survives the acute acidosis, it may succumb to secondary ruminal damage.30 Alternatively, the rumen may heal uneventfully, leaving scars in the ruminal wall, but bacterial access to the circulation through these chemical lesions can result in hepatic abscessation, a common problem of animals fed high-concentrate rations.110,112
In addition to lactic acid, several toxic factors have been implicated in acute ruminal acidosis.111,119 The altered metabolism of the ruminal microflora has been shown to generate increased quantities of histamine, ethanol, methanol, tyramine, and tryptamine. Although conlusive evidence is lacking, these may play a role in the pathogenesis of the disease. For example, histamine been implicated as an agent in the development of laminitis that sometimes accompanies ruminal acidosis.56 Histamine-producing microbes such as Allisonella histamini- formans thrive at low pH, and histamine can be absorbed through the rumen wall when the epithelium is damaged, as occurs in acidosis.8 In addition, the destruction of ruminal Gram-negative bacteria has been suggested to release large quantities of endotoxin for absorption through damaged epithelial surfaces. Endotoxin would contribute to most of the signs of the disease such as ruminal stasis, poor tissue perfusion with cardiovascular deterioration, weakness, and depression. Increased ruminal and blood concentrations of endotoxin and increased blood arachidonic acid metabolites have been found in cattle with experimentally induced ruminal acidosis, but their importance in naturally occurring disease remains uncertain.1,4-6 With liver impairment and ruminal wall damage, toxin absorption and clearance are likely to be altered. Premature delivery and retained placenta may occur in pregnant animals after acute ruminal acidosis, possibly as a result of from the effects of these circulatory toxins and metabolites.123
Severe grain overload requires prompt and aggressive treatment. Animals showing severe depression, an unresponsive condition, apparent blindness, and gross ruminal distention warrant a grave prognosis. Immediate slaughter should be considered for animals with similar signs but still able to stand. Emergency rumenotomy and removal of the acidic ruminal contents may be life-saving if the procedure can be performed before significant amounts of ingesta have passed into the lower gastrointestinal tract.99 An alternative treatment in less severe cases is repeated flushing of the rumen with warm water through a large-bore stomach tube. Administration of magnesium hydroxide into the rumen and sodium bicarbonate solution (5%) intravenously is necessary to counter the acidosis. Intravenous fluid therapy should be continued until the animal has recovered to provide support against hypovolemic shock.138 Other treatments that may be considered include NSAIDs. Additional therapeutic measures such as transfaunation and dietary adjustment should be continued during the recovery phase.
SUBACUTE RUMINAL ACIDOSIS. Like acute ruminal acidosis, subacute ruminal acidosis (SARA) is caused by feeding of excessive quantities of concentrate or low levels of well- structured fibrous roughage. However, SARA results from continued ingestion of these feeds over a prolonged period rather than sudden exposure without adequate adaptation. Beef feedlot cattle may be chronically exposed to a ruminal pH between 5.0 and 5.5 from the start of the intensive feeding period until slaughter. Dairy cattle are more probably limited to short periods of low ruminal pH, typically between calving 89118
and approximately 5 months post partum.89, In early lactation, dairy cattle may be exposed to energy-dense rations too rapidly, whereas the high feed intake of cows in midlactation renders them particularly susceptible to sudden ration changes or faults in feed delivery or composition.48 The ruminal microbial population adapts to a high grain ration, and large numbers of lactate-using and lactate-producing organisms are found. The proportion of cellulolytic bacteria decreases, whereas the starch- and glucose-fermenting species proliferate. The overall effect of the adaptation is development of a microbial population that rapidly ferments the ingested feedstuffs. Lactic acid does not accumulate because it is further metabolized by the bacteria. The increased rate of fermentation instead produces high concentrations of VFAs and results in moderately acidic ruminal fluid with pH values usually ranging from 5 to 5.5,59 although pH values between 5.5 and 5.8 may suggest that cows are at risk for SARA.48 Ruminal buffering of the increased acid load is impaired because the fine particle size of the high-energy rations induces less chewing and less saliva production.40 As the name implies, the effects on the animal are chronic and insidious.
Along with the high concentration of VFAs and the low pH, a shift occurs in the proportions of the VFAs in the ruminal fluid. The proportions of butyric and propionic acids increase, and acetate decreases. Butyric and propionic acids stimulate dramatic structural changes and proliferation of the ruminal papillae epithelium within a few days of an acidotic insult. When this process is exaggerated it can progress to parakera- tosis.141 The ruminal papillae develop an excessively keratinized epithelium and clump. The parakeratotic changes are associated with decreased absorption of the VFAs and increased susceptibility to trauma and inflammation.91 Epithelial damage and the acidic nature of the ingesta appear to be responsible for inflammation of the deeper tissues of the ruminal wall in some cases. The damage to the ruminal mucosa can lead to mycotic rumenitis or ruminal wall abscessation or can disseminate infection through the bloodstream to other organs, most notably the liver, which results in the formation of abscesses.110 Liver abscesses usually have no pathognomonic signs. Affected animals tend to show poor productivity and may have signs of a chronic inflammatory response.48,55,63,84,89,110
The diagnosis of SARA is made on a herd level rather than on an individual cow basis. Cattle afflicted with SARA may demonstrate numerous clinical signs, including reduced appetite and ruminal hypomotility.118 High ruminal VFA concentrations can inhibit ruminal motility by stimulating the inhibitory receptors in the epithelium. The finely ground ingesta also induces less active ruminal motility because it lacks the physical bulk of high-roughage diets that stimulate strong and sustained contractions. Although the bacterial population is metabolically very active, the number of species of bacteria is reduced,73 with losses to both ruminal and epimural bacterial community diversity.61,158 Likewise, the protozoal population is inhibited when the pH remains in the lower end of this range. The microfloral environment is less stable when fewer species are present and is thus more susceptible to sudden changes in the diet.
A continual high acid load may also reduce metabolic efficiency and overall animal performance. Cows may produce less milk, increase milk fat percentage, and demonstrate a positive deviation in the milk fat-to-lactose ratio.83 High- concentrate diets also have been associated with poor use of dietary protein.101 Other pathologic conditions have been attributed to SARA, including acute or chronic laminitis114,134 and cerebrocortical necrosis. These conditions may be induced by some of the toxic by-products of acidic ruminal fermentation, such as endotoxins and hydrogen sulfide.1,4-6,36,63,84
FROTHY BLOAT. Frothy bloat results from the formation of stable foam in the rumen. Ruminal tympany is synonymous with bloat. The condition may be fatal if the distention is extreme enough to compromise ventilation by compressing the thoracic viscera. Cattle are more susceptible than sheep, but the disease does occur in small ruminants.
The degree of forestomach enlargement varies from that producing an even filling of the left paralumbar fossa to that causing a uniform, extreme abdominal enlargement when the animal is viewed from the rear. With intermediate degrees of distention, the left paralumbar fossa bulges beyond the contours of the last rib and the tuber coxae. Clinical signs of colic may be seen, including kicking at the abdomen, treading, frequent lying down and rising, and vocalizations. Some animals adopt a stretched stance with the rear feet placed far back. In sheep with heavy fleece, significant bloat may not be apparent because the changes in abdominal contour are not obvious. As the forestomach enlarges and compresses the diaphragm, breathing
becomes more labored. Open-mouth breathing, cyanosis of mucous membranes, and collapse that leads to death may occur within a few minutes if the animal becomes frantic from the abdominal pain and respiratory distress. Other conditions to consider in the diagnosis of frothy bloat in ruminants include other causes of ruminal enlargement: free gas bloat and obstructive indigestion. Many systemic conditions influence the motility of the forestomach and thus may produce mild bloat coincidentally.
Clinical pathologic measurements are not necessary for the diagnosis and management of most cases of frothy bloat in ruminants. Evaluation of a sample of ruminal contents may provide useful information for prescribing treatment and prevention. The presence or absence of froth and the pH are critical features relating to the cause that influence the choice of therapy. The normal pH of the rumen varies with time after feeding but should be between 5.4 and 6.8.
Regardless of the cause of forestomach distention, the process may become self-perpetuating because of reflex inhibition of motility. Low-threshold stretch receptors in the ruminal wall augment cyclic forestomach contractions when stimulated. However, stimulation of high-threshold stretch receptors leads to inhibition of motility. Thus beyond a certain degree of stretching of the ruminal wall, further contractions that may relieve the distention through eructation are prevented.126
Frothy bloat is caused by the retention of gases of fermentation within the mass of ingesta that fail to rise and coalesce into a dorsal gaseous layer. This condition can arise from diets of lush legumes or winter wheat pasture or may be seen with high-concentrate finishing rations in the feedlot. In the case of legume-induced disease, bloat has occurred after grazing or feeding of fresh-cut forages or the feeding of alfalfa hay. The structure of stable froth in the affected ruminal contents is not true foam. The ingesta in the septa between adjacent bubbles form a complex structure that prevents coalescence. The viscosity of the fluid may prevent gravitational flow through the septa that would lead to the bubbles' rising and coalescing. Frothy ruminal fluid is higher in chloroplast membrane fragments, soluble protein, and very fine particles than is nonfrothy ruminal fluid.74 The presence of the resulting frothy ingesta at neural receptors believed to be near the cardia prevents the reflex relaxation of the cardia during the secondary contractions of the forestomach that ordinarily lead to eructation.67 In addition, the viscosity of the frothy ingesta is such that the cardia may become plugged during attempts to eructate.
Risk factors associated with the occurrence of frothy bloat can be categorized as animal risk factors, plant characteristics (species and maturity), and weather conditions.74 Individual cattle have been classified as having either high or low susceptibility to legume bloat. Highly susceptible cattle have been shown to have larger ruminal volumes and specific salivary proteins in consistently different proportions in comparison with bloat-resistant cattle. There is a relationship between plant factors associated with bloat and the rapidity with which leaf structure is disrupted after ingestion.74 Bloat-inducing plants are more readily macerated, which provides quicker bacterial access to the inner leaf cells. Less bloat-predisposing cultivars of the main bloat-causing species, such as alfalfa (Medicago sativa), red clover (Infolium pratense), and white clover (Trifolium repens), have a thicker leaf cuticle, smaller stomata, and a more fibrous leaf structure. Ionophore antibiotics such as monensin inhibit ruminal protozoa that normally ingest chloroplasts, which leads to a reduction in the bloat potential of some forages.13,80
Grain bloat occurs in a manner similar to that caused by legumes; a stable froth is produced from high-concentrate rations. Particle size and the rate of fermentation are thought to be the determining factors in the froth production. A mucoprotein slime composed of bacterial by-products stabilizes the froth.13,128 This material tends to be stable at a lower pH than is found in non-grain-fed ruminants, so grain feeding promotes slime accumulation by lowering ruminal pH. Animals (such as dairy cattle) that are fed grain and then legumes may be particularly susceptible to frothy bloat because all the factors that lead to froth production and accumulation are present. Both legume bloat and grain bloat may resolve spontaneously if the animal stops consuming the bloat-producing feed and microbial digestion eliminates the froth-stabilizing factors.
Acute distress, often appearing as abdominal discomfort, is caused by overdistention of the forestomach that stimulates pain receptors in the ruminal wall. As the abdominal distention increases, an affected animal's ability to achieve normal respiratory movements of the diaphragm and rib cage is impaired. This exacerbates the animal's anxiety and distress. Death from asphyxia ultimately results as the lungs are compressed by the cranially expanding diaphragm, and venous return via the posterior or caudal vena cava is compromised.
Frothy bloat often occurs as an epidemic. Pasture bloat may occur wherever alfalfa, red clover, or white clover is grazed. Environmental conditions that produce rapid, early growth lead to a higher incidence of bloat. Frothy bloat also occurs when stocker cattle are grazed on winter wheat pastures in the southern Great Plains of the United States. Death rates at pasture range from 0.5% to 2.5% of cattle at risk on an annual basis. The incidence of feedlot bloat has been estimated at approximately 1%, with death rates of approximately 0.1%.74
The finding of tenacious froth in the rumen, along with other evidence of bloat, is grounds for a presumptive diagnosis of frothy bloat. The challenge for the diagnostician is to determine whether the bloat occurred before death; this may not be possible if the animal was not observed before death. The increase in intraabdominal pressure prevents venous return from the hindquarters and may lead to obvious edema in the intermuscular areas. Unfortunately, this is not a consistent finding; other evidence of impaired circulation or a differential degree of edema between fore and hind parts must be used to make a diagnosis.
Passage of a stomach tube is indicated to determine the cause of the ruminal distention and possibly initiate treatment. A sample of the ruminal contents for pH measurement should be obtained at this time. Care must be taken to exclude saliva from the tube by blowing into the rumen, flushing water through the tube, or using a ruminal sampling device that carries the tip of the stomach tube down into the liquid ingesta. If no gas can be released with a stomach tube, the tube should be withdrawn after suction has been applied and should be examined for the presence of froth. If the animal is not in respiratory distress or extremely colicky, surface-active agents should be administered by means of a stomach tube. Poloxalene or mineral oil can be given.
Some cattle are in violent pain with bloat but not in respiratory distress. Sedation with xylazine may be necessary for further examination and treatment. Animals with extreme distention of the forestomach and in respiratory distress require immediate surgical intervention. A trocar introduced through the left paralumbar fossa after local anesthesia relieves bloat caused by free gas accumulation but may not be adequate for frothy bloat. An emergency rumenotomy may be necessary to evacuate frothy contents.
Prevention of frothy pasture bloat relies on the general principle of decreasing the rate of rumen fermentation. To significantly modify the rate of rumen fermentation, grazing management strategies and controlling pasture yields and quality remain the most common methods applied to a population. Cattle could be fed other feeds before being turned out and could be allowed limited access to the problem forages. Accurately predicting when forages are safe has not been reliable. Strip grazing, another option, allows cattle a reduced amount of new forage every few days. The choice of forages and the stage of growth are also to be considered. Agronomists are selecting cultivars of the bloat-producing forages for slower rates of initial fermentation. These are likely to become more widely used in the regions in which bloat is a regular occurrence. When grazing strategies and pasture management are not enough, then as an alternative, cattle at risk have been treated with supplemental surface-active agents such as poloxalene or mineral oil. In Australia and New Zealand, oils and tallows have been drenched daily, sprayed on fields, and smeared on the flanks to be later licked off, to prevent pasture bloat. Although poloxalene has proved effective, it is more expensive than oils. It can be fed in molasses blocks or individually administered. Ionophore antibiotics such as Rumensin (monensin; 1 mg/kg daily) greatly reduced the incidence of legume bloat. Beginning treatment before exposure to the bloat-inducing feed was more effective than waiting until bloat occurred. Providing adequate fiber in feedlot rations and slowly introducing higher proportions of concentrates, particularly corn, barley, and soybean meal, enable ruminal adaptation that helps prevent bloat.
RUMINAL ALKALOSIS. An alkaline ruminal fluid pH occurs most commonly when microbial fermentation is reduced while the animal continues to ingest saliva. A ruminal fluid pH between 7 and 7.5 is found with prolonged anorexia, microfloral inactivity caused by poorly digestible roughage, and some cases of simple indigestion. The low rate of fermentation does not generate enough acid to neutralize the alkaline pH of the saliva. In addition, the absorption of VFAs through the ruminal epithelium proceeds with the generation of bicarbonate in the ruminal fluid. Acetate absorption is associated with greater generation of bicarbonate than is absorption of the other VFAs, and acetate is the predominant VFA produced during fermentation of roughage. Although the fermentation rate is low, the VFA absorption contributes to the ruminal alkalinity. Ruminal alkalosis occurring with these diseases is not the primary problem; therefore these entities are discussed separately.
Ruminal alkalosis can occur with the generation of excessive ammonia. Ammonia concentrations rise when high-protein diets are fermented. The pH usually does not increase above neutral because these diets also contain sufficient readily fermentable carbohydrate to maintain a slightly acidic pH.
More dramatic elevations in the ammonia concentration, with a ruminal fluid pH above 7.5, occur with overfeeding of nonprotein nitrogen sources such as urea, biuret, and ammonium phosphate (see Chapter 54). Accidental ingestion of some common fertilizers that contain ammonium salts can produce the same results. For the purpose of this discussion, it is important to realize that some of the signs of urea poisoning involve ruminal dysfunction. Severe cases of urea poisoning result in generalized signs such as muscle tremors, incoordination, weakness, tachypnea, and central nervous system excitation, and affected animals die quickly. Signs of forestomach dysfunction such as ruminal hypomotility, bloat, vomiting, and abdominal pain are also present. In milder cases, diminished appetite, ruminal hypomotility, recurrent tympany, and diarrhea may be the most prominent signs, along with muscular weakness and incoordination. Thus the disease may appear as a form of forestomach disease. The ruminal fluid shows an alkaline pH between 7.5 and 8.5 and has a strong odor of ammonia.130
PUTREFACTION OF RUMINAL INGESTA. Putrefaction of ruminal ingesta infrequently results from overgrowth of a microflora that decomposes feed material in a putrefactive manner. A high ruminal fluid pH, as exists with high-protein feeds, and repeated inoculation with abnormal bacteria allow the development of the putrefactive decomposition. Fermented feeds undergoing spoilage, feed and water contaminated with feces, and spoiling, contaminated concentrates supply the offending microflora, which includes the coliform group and Proteus spp.43 This type of abnormal decomposition is ordinarily inhibited by the existence of an active physiologic microflora. Thus most cattle are remarkably resistant to aberrant digestive patterns even when spoiled feeds are ingested. This form of indigestion typically follows a chronic course. Ruminal motility declines, appetite is poor, and recurrent tympany develops, sometimes with the generation of frothy ruminal contents. The ruminal fluid characteristically has a blackish green color, a foul, putrefactive odor, poor protozoal and bacterial activity, and a pH in the neutral to alkaline range of 7 to 8.5. The cause of the forestomach hypomotility may be inhibitory products generated by the abnormal fermentation. In cases of prolonged duration, animals lose weight and display a poor hair coat, probably as a result of dietary deficiencies in the abnormal fermentation products.
Rumen Fluid Analysis. Evaluation of ruminal fluid characteristics is an essential procedure in establishing the cause of the indigestions of abnormal fermentation.22,119 Several important determinations can be made at cowside in an ambulatory practice. Acquiring an appropriate sample is simplified with proper equipment. The advantages of various collection techniques and devices have been discussed.57,116 Needle puncture of the ventral ruminal sac (ruminocentesis) may yield a satisfactory fluid sample, and studies demonstrate that rumenocentesis samples provide the most reliable evaluation of ruminal fluid pH for field evaluation of subacute ruminal acidosis.49,57,116 Oral or nasal passage of a collection tube produces more fluid volume with no risk of peritoneal contamination but with an increased risk of saliva contamination. The ideal site for collection of rumen fluid for pH evaluation is the ventral rumen sac, where saliva is minimal, whereas investigators examining analytes such as VFAs and ammonia have suggested that sampling in the central rumen is appropriate.135
An adequate tube for aspiration of a ruminal fluid sample should be at least 2.3 m long to reach the ventral ruminal sac and should have an internal diameter of 1 cm or larger to reduce the incidence of plugging with ingesta. To adapt a plastic stomach tube for use in passing orally or nasally, multiple holes can be cut into the ruminal end of the tube. A digital examination glove can be placed over the end during passage to limit saliva contamination of the sample and then is forcefully blown off before sampling. The sample can then be withdrawn by a dose syringe. This technique is successful when ruminal fluid is accessible in the dorsal rumen, but the flexibility of the tube is disadvantageous when a prominent layer of fibrous feed is present. Several instruments with a flexible steel outer tube are commercially available (Dirksen Rumen Fluid Tube, Allschwil, Switzerland; Geishauser probe, Hamburg, Germany; Select-Collector, Hamberg, Germany) and have the advantage of enough stiffness and weight to penetrate the overlying firm layer of ingesta for collection of fluid from the ventral rumen.143
Ruminal fluid samples collected in an expeditious manner yield the most useful results. When the animal strongly resists sampling and a prolonged time is required from introduction of the tube until the fluid is obtained, saliva contamination of the sample increases. This contamination alters the pH and consistency of the sample. The specially designed ruminal fluid collection tubes reduce this problem. If the sample must be collected with a standard nasogastric tube, passing the tube nasally avoids the presence of a device in the mouth. This reduces the amount of struggling (once the tube has passed the pharynx) and thus reduces excessive salivation.
The sample should be evaluated as soon as possible after collection to minimize the effects of cooling and air exposure on protozoal activity and pH. Some chemical tests such as chloride, and ammonia concentrations can be delayed up to 9 hours on a room temperature sample and up to 24 hours on a refrigerated sample and still yield reliable results.41 Ruminal
■ TABLE 32.19
Diagnostic Ruminal Fluid Analysis
| Parameter | Normal |
| Color | Olive, brownish-green |
| Consistency | Slightly viscous |
| Odor | Aromatic, strong |
| pH | 6 to 7 on roughage |
| Sedimentation/ flotation | 5. to 6.5 on grain diet 4 to 8 min |
| Redox potential | 3 to 6 min |
| (methylene blue reduction time) Protozoal activity | Multiple forms, active motion |
| Gram stain | Predominant Gram-negative |
| Chloride concentration | bacterial population result in rising pH values in these cases as well and that the ruminal pH of a cow with ruminal acidosis can be normal if a sufficient period of anorexia precedes the ruminal fluid analysis. Conversely, a ruminal pH of 5.5 to 6 is abnormal for a cow fed a roughage diet and may be indicative of unobserved access to grain and resultant lactic acidosis. Subacute or chronic ruminal acidosis usually is accompanied by a ruminal pH in the range of 5 to 5.5.57,89,93,119 Abomasal reflux into the reticulorumen caused by abomasal disease, obstructive indigestion, or intestinal obstruction can cause mild decreases in ruminal pH because of the acidic nature of abomasal contents. However, ruminal pH measurement is a poor means of detecting abomasal reflux because the pH often remains within the wide range of normal values. Abomasal reflux is better assessed by measurement of reduced buffer capacity or the ruminal chloride concentration. Sedimentation. The sedimentation time, or sedimentation/ flotation test, provides a quick evaluation of microfloral activity. It must be conducted promptly after collection of the sample. The aspirated fluid is allowed to sit in a tube, and the time for completion of sedimentation and flotation of the solid particles is measured. Normally the finer particles settle to the bottom and the coarser particles float, buoyed by the gas bubbles of fermentation. Some of the finer particles sink and then rise again when the fermentation is very active. The normal time for completion of this activity is 4 to 8 min. Grossly inactive fluid shows very rapid sedimentation, and none of the material may float. This occurs with ruminal acidosis, prolonged anorexia, and microflora rendered inactive by indigestible roughage. When the ingesta is particularly frothy, as in cases of frothy bloat or some cases of obstructive indigestion, there may be no appreciable sedimentation or flotation. This test provides a crude evaluation of microfloral activity but does not differentiate well among the different forms of indigestion. Redox Potential. The redox (reduction-oxidation) potential of ruminal fluid is a biochemical characteristic that reflects the anaerobic fermentative metabolism of the bacterial popula- tion.155 A clinician can determine the redox potential indirectly by measuring the time required by ruminal fluid to decolorize methylene blue dye. A mixture of 1 mL of 0.03% methylene blue with 20 mL of ruminal fluid at normal body temperature is observed in a tube and compared for color with another unaltered tube of the ruminal fluid. With highly active microflora from an animal fed a hay and grain diet, the initial dark blue color of the mixture decolorizes within 3 minutes, leaving a narrow ring of blue color at the top of the decolorized sample. Fluid from a diet of hay alone requires 3 to 6 minutes to decolorize, and that from a mostly grain ration requires as little as 1 min. Reduction times up to 15 min and longer occur with diets of indigestible roughage, in anorexia of several days' duration, and after ruminal acidosis.22 Thus the methylene blue reduction time provides an assessment of the degree of bacterial fermentative activity. Microscopic Examination. Evaluation of the number and activity of protozoa in the ruminal fluid provides a sensitive indicator of the normality of the sample.155 This is easily accomplished by microscopic examination of a drop of fresh, warm fluid. The examination requires only low magnification (?40 to ?100) and no special stains. In very active fluid samples, the largest protozoa can be seen with the naked eye. They are detectable in a tube as small gray specks of material in active motion in the fluid, and they tend to localize above the sedimented particulate matter. Both ciliate and flagellate forms of varying sizes and shapes can be observed microscopically, with ciliates usually outnumbering the flagellates. The protozoa are normal inhabitants of a healthy ruminant's ruminal fluid, although their specific function is not completely clear and their presence does not appear to be a prerequisite of normal digestive activity.159 The importance of the protozoa from a clinical viewpoint is their sensitivity to abnormalities in the fluid milieu. Normal ruminal fluid should contain protozoa in a wide variety of sizes, in large numbers that are easy to see, and with active motility. Numbers of protozoa are reduced in inactive fluid samples. The larger species are more susceptible to abnormalities; thus a predominance of small protozoa would suggest a mild indigestive disturbance. All protozoa are killed off when the ruminal pH drops below 5. Thus a recent bout of acidosis results in lack of protozoal activity, even if the pH has subsequently risen back into the normal range. Fluid from such an animal should also show other abnormalities of color and consistency. Very recent disturbances of the fluid may result in the observation of a large number of dead protozoa. Although elaborate isolation methods for evaluating ruminal bacterial growth are not clinically applicable, examination of an air-dried, Gram-stained smear of ruminal fluid can be useful in diagnosing ruminal acidosis. Normal ruminal fluid should contain a variety of morphologically distinguishable bacterial forms, with a predominance of Gram-negative organisms.41 After the overconsumption of readily digestible carbohydrate (grain engorgement), a population of streptococci and lactobacilli proliferates as ruminal lactic acidosis develops. This shift in the bacterial population can be distinguished microscopically, and a predominance of Gram-positive cocci and rods are seen. The findings are best confirmed by comparing a smear from a herd mate. Ruminal Fluid Chloride. The chloride concentration in ruminal fluid can be determined from the supernate from a centrifuged sample through the use of standard chloride titration devices. A delay in measurement does not appreciably affect the value. Saliva contains concentrations of chloride similar to those of normal ruminal fluid, so that saliva contamination has minimal effect on the results. The normal ruminal fluid chloride concentration is less than 30 mEq/L, with elevated values demonstrating reflux of abomasal ingesta into the rumen or administration of chloride in the feed or as therapy. Accurate assessment of measured values requires information about possible previous oral administration of electrolytes. In the clinical evaluation of forestomach dysfunction, an elevated level of ruminal chloride suggests secondary indigestion caused by abomasal disease or obstruction of intestinal flow. This test can be very helpful in differentiating abomasal reflux from ruminal lactic acidosis as the cause of low ruminal pH and abnormal fluid accumulation in the reticulorumen. With obstructive indigestion a high level of ruminal chloride suggests that the failure of aborad flow is posterior at the pylorus rather than anterior at the reticuloomasal orifice.124 In general, cattle with elevated levels of ruminal chloride also have hypochloremia and metabolic alkalosis as a result of the chloride sequestration in the forestomach, although very slow development of the sequestration may allow the animal to maintain normal plasma levels by altering other excretion rates. Numerous other tests of the ruminal fluid have been described for the evaluation of digestive activity of the ruminal microflora. These include cellulose digestion, glucose fermentation, nitrite reduction, and measurements of titratable acidity, VFAs, lactic acid, and ammonia concentration.41 These procedures can more clearly define the nature of the ruminal fluid but are not generally used in a clinical setting. TREATMENT, PROGNOSIS, AND PREVENTION OF FERMENTATIVE DISORDERS. With the exception of severe acute ruminal acidosis, the disturbances of reticuloruminal fermentation generally are not fatal unless the disease is undiagnosed for a prolonged period, which leads to extreme debility. Treatment of fermentation disorders centers around restoring a normal ruminal fluid environment that allows normal microbial metabolism. Identification of ruminal fluid parameters (see Table 32.19) and the nature of the forestomach ingesta directs the appropriate treatment (Box 32.6). Feeding. The first and most important step in treatment of nutritionally related indigestions is correction of the specific causal feeding error. Because the imbalance may have gone on for weeks, especially in cases of calf indigestion, correction of the problem may also take some time. The evolutionary development of the ruminant has adapted it to be a grassland grazer. Economic pressures in the animal industry have caused managers to institute feeding practices that diverge widely from a pasture setting. Fresh green grass, however, remains one of the best means of stimulating normal forestomach digestion and motility. The second best type of diet includes a balance of palatable and digestible sources of energy, protein, fiber, and mineral nutrients. Fiber requirements should be determined by considering both the physical effectiveness of fiber and the production of fermentation acids. The content of structured roughage should not fall below 10% of the ration dry matter, and a crude fiber component above 17% is desirable for any ration. ■ BOX 32.6 Principles of Treatment of Fermentative Indigestions Alteration of Ruminal Contents. When the viability or activity of the ruminal microflora is in question, as in the primary fermentative disorders and most cases of secondary indigestion, ruminal transfaunation is indicated.39,122 The material should be obtained from a healthy individual that preferably is adapted to a ration similar to the one the patient is expected to consume. The fluid can be obtained from an animal with the rumen cannulated, by removal with a stomach tube, or from a local abattoir. After the large particulate matter has been strained from the fluid (cheesecloth or large stockinette can be used), it can be administered through a stomach tube. The transfer from donor to recipient is best accomplished immediately, but fluid that contains active and healthy microflora remains viable for up to 9 hours at room temperature or 24 hours under refrigeration.109 Some clinicians add mineral oil to the fluid, which rises to the top and minimizes exposure to air in order to maintain anaerobic conditions. In calves, inoculation with 1 L is appropriate to reestablish microbial populations, whereas 3 L is minimal in an adult cow, and 10 to 16 L is more desirable. Similarly, transfaunation of sheep or goats with 1 to 4 L of fresh rumen fluid can reestablish normal microbial populations.39 Many animals with indigestion exhibit decreased ruminal fill. As discussed, one of the primary stimuli for active ruminal contraction is mild forestomach distention. In addition to the administration of ruminal transfaunate, it is usually beneficial in these cases to administer enough oral fluid to produce mild ruminal distention. This can be accomplished with water warmed to body temperature, and 20 to 30 L of fluid administered through a tube may be needed to achieve the desired effect. The addition of salt (sodium and potassium chloride) in amounts sufficient to produce an isotonic solution (≈2 teaspoons per liter) supplements deficiencies and promotes rapid turnover of the fluid from the rumen to the lower tract. Cathartic agents such as magnesium sulfate have been used but do not serve to supplement the common electrolyte deficiencies. Correction of pH abnormalities to the normal range of 6 to 7 is important when ruminal acidosis or alkalosis is detected. Alkalinizing agents such as magnesium hydroxide and sodium bicarbonate are indicated for treatment of acidosis at an initial dose of 1 g/kg. Magnesium hydroxide is commonly used by some as a routine treatment for any animals in which ruminal hypomotility has been identified. This practice is not justifiable in most cases of ruminal hypomotility because the fluid pH is commonly at or near neutral. The use of magnesium hydroxide in such settings may induce a mild systemic alkalosis, and the agent is better reserved for true cases of acidosis. Ruminal alkalosis can be corrected with the infusion of acetic acid (vinegar, initial dose of 2 mL/kg, up to 12 L). These agents are best administered in several liters of warm water to ensure good distribution throughout the ruminal fluid. Overdistention of the ruminal wall may be a primary inhibitor of forestomach motility in some cases of indigestion caused by abnormal fermentation. Treatment of free gas bloat has been discussed. When the distention is caused by accumulation of abnormal ingesta, normal contractions do not return, and the ruminal tympany is not resolved until the distention is relieved. This situation is best exemplified by cases of microfloral inactivity caused by poor-quality roughage and is the underlying problem in calves with haybelly. One approach to this problem is to restrict the animal to small quantities of readily digestible feed given several times a day. Between meals the animal can be kept in an unbedded stall or muzzled. This process is continued until the accumulated ingesta has passed out of the forestomach. Repeated transfaunations during this time help reestablish a more normal microflora. This approach relies on motility and microbial activity sufficient to break down the ingesta and pass it to the lower tract. An alternative approach is to remove the accumulated ingesta by means of rumenotomy, after which the animal is transfau- nated and allowed access to moderate amounts of feed until normal motility is restored. Emptying the rumen surgically is the treatment of choice when spoiled milk, putrefactive ruminal ingesta, or severe ruminal acidosis is detected. Prolonged cases of microbial inactivity or anorexia (or both) with ruminal hypomotility can result in loss of the normal stratification of forestomach ingesta. The fibrous, floating layer sinks to the ventral ruminal sac in these cases, forming a dense, firm mass. Return of normal forestomach motility is delayed unless the accumulation of material can be eliminated. This can be accomplished during the process of microfloral reestablishment by massaging of the mass through the lateral and ventral body wall. Dissolution and passage of the material can be enhanced by the administration of mineral oil (4 L), or dioctyl sodium sulfosuccinate (4 to 6 ounces in 2 to 3 L of water). Because dioctyl sodium sulfosuccinate kills ruminal protozoa when given in amounts greater than necessary to saturate the fibrous matter, at least one ruminal transfaunate should be given 1 to 2 days after the last application of this agent. Animals with prolonged anorexia caused by a depressant or febrile disease that produced secondary indigestion may not return to feed or have normal ruminal motility even after the ruminal contents has been restored to normal. Chewing activity is one of the strongest stimulants for ruminal motility, and these animals sometimes benefit if palatable hay or grass is placed forcefully into the mouth by hand. An alternative is to give such animals access to pasture. In fact, during a bout of SARA, cows have been shown to self-regulate their dietary preference for physically effective higher fiber and slower starch fermentability.104 Both the ruminant and its ruminal microflora have trace mineral requirements that are often not met by the type of diets that may induce microfloral inactivity. The ruminal microflora is also responsible for supplying animals with their vitamin B requirements. The stunted, poor body condition of calves affected by chronic indigestion may reflect these deficiencies, as well as protein energy malnutrition (see Chapter 9). Oral supplementation of minerals and parenteral supplementation of the B vitamins may be helpful until normal ruminal digestive function is established. Adult cattle, especially lactating animals with high metabolic demands, may also benefit from B vitamin supplementation when ruminal function is impaired. Feeding changes and ruminal transfaunation are effective in inhibiting undesirable microbial populations, and inoculating the desirable population. When spoiled milk, putrefactive ingesta, or extremely acidic ruminal contents are found on ruminal fluid analysis, the desirable treatment is rumenotomy, removal of the contents, and flushing of the rumen. Supportive Treatments. Indigestion often is accompanied by varying degrees of dehydration and electrolyte imbalance. When these abnormalities are only mild or moderate, the animal's fluid homeostasis may correct itself as the normal digestive processes are restored. More rapid recovery is achieved if these problems are addressed during the initial treatment, and animals must be treated if the imbalance is severe. Restoration of normal fluid balance improves attitude, appetite, and gastrointestinal motility. When laboratory facilities are available and the specific electrolyte imbalances can be assessed, fluid therapy can be tailored to the individual case. Empirical treatment with a balanced electrolyte solution administered intravenously is sufficient in most cases because extreme disturbances of the body fluid electrolytes are uncommon in most indigestions. Exceptions include severe ruminal acidosis and obstructive indigestion with pyloric outflow failure and sequestration of abomasal chloride. These problems should be identified during the examination. Hypocalcemia and hypokalemia are routinely present in many cases of indigestion. Low serum concentrations of these elements can produce muscular weakness and impair gastrointestinal motility. Both calcium and potassium should be included in the administered fluids. As an alternative, calcium salts should be administered subcutaneously if intravenous fluid administration is not elected. Oral preparations of calcium salts are commercially available but seem less desirable as a means of treatment without normal rumen function. When anorexia has been prolonged, an additional oral dosage of potassium chloride (120 g/day) may be required even after adequate hydration has been achieved and fluid therapy has been discontinued. Prevention. Some of the sporadically occurring diseases of the forestomach wall such as granulomatous infections, neoplastic invasions, and diaphragmatic herniation cannot be foreseen or prevented. The most common cause of vagal indigestion is inflammation of the perireticular area caused by TRP. Prevention of this disease by keeping metallic foreign bodies out of the feed, removing them from the feed through the use of a metal retriever or magnet, or prophylactic administration of a ruminal magnet is highly effective. The microbial-fermentative forestomach disorders are best prevented by proper feeding management. A well-balanced diet of palatable feeds with an adequate amount of well-structured roughage (not finely ground or pelleted) prevents most problems. Dietary changes should be introduced slowly (over 2 to 3 weeks) to allow adaptation of the microbial flora to the new substrate. Calves undergoing ruminal development and cattle fed high- production diets or changing between production groups are at risk of oversights in proper feeding management. Feed-grade buffers are used widely in both dairy and beef cattle production, in which high-concentrate diets are fed to maximize production. Dietary buffering is largely explained by dietary cation-anion difference; diets high in sodium and potassium in relative to chlorine and sulfur demonstrate a higher dietary cation-anion difference and promote higher ruminal pH.75 These buffers stabilize the ruminal pH and alter the mechanics of ruminal fluid outflow, thus decreasing the chances of overgrowth of the lactate-producing organisms. Commonly used “buffers” include sodium bicarbonate, sodium sesquicarbonate, sodium bentonite, magnesium oxide, and calcium-magnesium carbonate, of which only the sodium carbonates are truly buffering agents in the chemical sense. The other agents do tend to stabilize ruminal pH, however, and all of these have shown some benefit in reducing the disease problems associated with heavy grain feeding and diets that are low or marginal in effective fiber. The ionophore antibiotics (e.g., laidlomycin, lasalocid, monensin) and some other antibiotics (e.g., the sulfur-containing peptide antibiotic thiopeptin) have also proved effective in reducing lactate production in animals fed high-grain diets. The effect of these agents is to suppress the lactate-producing organisms while not appreciably affecting the lactate users. The ionophores are in common use in feedlot cattle and dairy heifer rations because the selective effects of these agents on the ruminal microbes alter the ruminal metabolism in a manner that promotes increased animal weight gain.107 In 2004 the U.S. Food and Drug Administration approved the use of the ionophore monensin for lactating cattle in the United States. Although approval was based on increases in milk production efficiency, ionophore use may also reduce the risk of ruminal acidosis and ketosis.4,60 A number of other feed additives have proven effective in preventing the overgrowth of high acid-producing ruminal microflora and reducing the risk of disorders related to reticu- loruminal fermentive function.3,10,29,38,105 Research has increased the understanding of the importance of ruminal microbial diversity and the functional capacity of rumen microbial ecosystems under different dietary environments.87 Molecular biological advances have been used to profile microbial communities with the use of techniques such as terminal restriction fragment length polymorphism analysis, 16S ribosomal DNA libraries, and metagenomic approaches.90 The application of these tools in the evaluation of manipulators of ruminal fermentation can provide added value in optimizing feedstuff and 105 minimizing digestive disorders.105 Forestomach Diseases of Calves Normal forestomach development and diseases of the forestomachs of calves have been reviewed.11,37 The newborn ruminant has the same anatomic division of the stomach into four compartments as the adult ruminant. The abomasum is functional as a secretory digestive organ, like the stomach of monogastrics, and has a capacity approximately twice that of the other compartments. The remaining stomach compartments are small and do not perform digestive functions in the first days of life. The reticulorumen may not develop an adult-type function until the age of 4 months or later and does not completely develop proportional dimensions similar to those of the adult until the ages of 9 to 12 months.37,43,44,54,155 Traditionally, preruminant calves have been viewed as functionally monogastric animals, and little importance has been attached to diseases of the forestomachs. Under most management conditions, however, the forestomachs have begun to develop their digestive function within the first week or two after birth. During the development process, a calf's forestomach is susceptible to problems different from those of adults. After the rumen has developed a functional status similar to that of the adult, a calf is susceptible to the diseases discussed previously. Typically the feeding management of maturing young stock includes pasture or a mainly forage diet and does not predispose to digestive disturbance. ESOPHAGEAL (RETICULAR) GROOVE FUNCTION. Liquid feed bypasses the reticulorumen in the young ruminant, flowing directly into the abomasum through the esophageal groove. The groove consists of two lips that extend from the cardia to the reticuloomasal orifice. These lips close together, forming a tube to shunt liquid material to the abomasum when the soluble proteins and salts of milk stimulate a reflex through specific receptors in the oropharynx. Other salt solutions and even water can stimulate the reflex in very young animals, but the reflex weakens with age, especially after weaning. The response to stimuli varies among individuals, but generally milk produces the strongest response and plain water the weakest.127,131,152 Both nipple and bucket feeding stimulate closure in very young calves, but beyond 12 weeks of age, closure is weak unless stimulated by nipple feeding. In older, weaned animals, the reflex can be stimulated weakly for short durations by orally administered strong solutions such as copper sulfate or sodium salts. Intravenous vasopressin can induce more profound closure of the groove and has been advocated to aid ruminal bypass of orally administered treatment.131 Milk replacers that contain nonmilk protein appear to stimulate a weaker closure of the esophageal groove than do whole milk or milk replacers containing real milk protein. Likewise, unpalatable fluids and spoiled milk do not seem to induce normal closure of the groove. Even in healthy calves that consume unspoiled whole milk, some overflow into the forestomach may occur. Failure of esophageal groove closure allows these fluids to pass into the rumen rather than bypassing it. Milk or other fluid administered through stomach tube or esophageal feeder does not contact the pharynx; therefore the reflex closure is not stimulated and the fluid deposits in the forestomachs. Under normal conditions fluid in the forestomach of neonatal calves younger than 2 weeks of age overflows into the abomasum when more than 400 mL has accumulated.27
FIG. 32.129 Causes of abomasal reflux in calves. HCl, hydrochloride. Reticuloruminal Milk Accumulation (Ruminal Drinking Syndrome). Milk can gain access to the reticulorumen by several means. Failure of esophageal groove closure, just discussed, is one possibility. In addition, if calves are maintained as preruminants for longer than 3 to 4 months, groove closure weakens and may allow greater escape of fluid to the reticulorumen. Fluid can also accumulate in the forestomach from abomasal reflux (Fig. 32.129). Overfeeding fluids beyond the capacity of the abomasum (≈2 L in the newborn, 35-kg calf) promotes backflow into the reticulorumen. Certain fluids affect abomasal motility and emptying times, prolonging their retention in the organ. These include acidic and hypertonic fluids and severely heat-treated skim milk powder. Nonmilk protein does not curd in the abomasum, as does casein, when it contacts the abomasal enzyme renin. Prolonged fluid retention and failure of curd formation in the abomasum may promote backflow into the rumen, especially when more fluid feed is consumed. Abomasal inflammation or ulceration may also inhibit normal emptying and promote abomasal reflux. In any case, ultrasonography may be useful for detecting milk in the reticulum and rumen of calves with ruminal drinking syndrome.16 Some amount of milk reflux from the abomasum appears to be a physiologically normal occurrence. In fact, this route supplies some of the inoculum for ruminal microfloral development and strongly influences the species distribution of the microbial population. But prolonged, repeated, or excessive retention of milk in the forestomach can lead to the development of abnormal fermentation patterns. Although amounts of fluid greater than 400 mL do not normally accumulate in the forestomach of neonates, more fluid can accumulate when the abomasum is already filled and when ruminal size has increased during the development process. In some cases, milk flow into the rumen accumulates significantly over prolonged periods. The predominant organisms that constitute the forestomach microflora of 1- to 4-week-old ruminants are the coliforms and lactobacilli. These lactose-fermenting, facultative anaerobes tend to maintain the ruminal pH in the acidic range before the adult-type, anaerobic, cellulolytic flora becomes established. The high fat and protein content of milk in the rumen can predispose to a flora that decomposes these constituents and produces spoiled and rancid ruminal ingesta. Problems associated with ruminal milk accumulation are compounded when the milk or other fluid ingested is already contaminated or spoiled. The abnormal microflora established under these circumstances does not supply the young animal with the necessary digestive end products, and signs of dietary insufficiency develop. Affected animals fail to grow normally, show a poor hair coat potentially with widespread alopecia, and may have a depraved appetite. The stimuli for normal forestomach development are also deficient; affected animals have a potbellied appearance, and the rumen is distended with fluid and clots of milk. Ruminal motility is poor, and recurrent bloat is a common sequela. The ruminal fluid pH may be alkaline as a result of the proteolytic formation of ammonia, but in most cases the ruminal pH is acidic (cause obstructive disease or abrade the parakeratotic papillae or the abomasal mucosa, predisposing 44 the animals to ulcers and inflammatory lesions.44 Acute ruminal acidosis is not typically recognized in young, developing ruminants, probably because feed consumption is limited and because the predisposing adult-type ruminal microflora have not yet developed. An opposite extreme can occur when the young calf is fed dry forage to the exclusion of more readily digestible carbohydrates. Concentrates and grass contain soluble carbohydrates and are well digested by the developing ruminant. Hays contain much less soluble carbohydrate and an abundance of the structured, slowly digestible forms. These substances are not as well digested by calves because the appropriate cellulolytic microflora are not fully developed. With moderate hay intake and the supply of other sources of nutrition, problems are rarely encountered. When dry roughage is the only available feed, and particularly when the hay is of poor quality, adequate breakdown of the fiber is prolonged. The low availability of nutrient substrate that results from delayed digestion of the structured carbohydrates decreases microbial proliferation and fermentation. Inadequate fermentation of the feedstuff deprives animals of required nutrients as well and results in poor performance and growth. When the only available feed source is the hay ration, calves continues to consume while the long undigested fiber accumulates in the rumen. The rumen continues to expand as a result of the increased filling, eventually becoming grossly distended. Recurrent bloat is common in these animals because of the overfilling and poor ruminal contractility. This phenomenon is a frequent occurrence under some management conditions and has commonly been called “haybelly.” Affected animals display a typical abdominal contour, with gross distention of the abdominal wall that is more prominent on the left side. The ruminal contents are very firm, the fluid has a pH around neutral and shows little microbial activity or odor, ruminal motility is poor, and, despite the full abdomen, the animal is thin. This form of microfloral inactivity is more common in calves than in adults because the young ruminant is less able to ferment fibrous roughage.43,44 Recurrent Bloat (Ruminal Tympany). Moderate gas distention of the rumen is a common sign of disease in calves, usually as a result of free gas accumulation, whereas frothy fermentation is very uncommon in young ruminants. The pathogenesis of free gas bloat has been discussed, and the same principles hold for young ruminants. The differences between free gas bloat in adults and in young calves are more a matter of chronicity and frequency of occurrence than cause. Digestive disturbances of the adult rumen tend to develop more rapidly and are more readily identified than those of the calf rumen. Because of the involvement of ruminal developmental processes in the pathogenesis of calf indigestion, in young ruminants the diseases are often more chronic than acute in nature. In most cases the calf continues to consume feed, and the abnormal ruminal function and development may be easily overlooked. Ruminal tympany seems to accompany indigestion in calves more often than in adult cattle and also assumes a more prominent appearance in calves than in adults. These factors may be reflections of the juvenile anatomy and the incomplete development of adult function. For instance, left-sided abomasal displacement, although uncommon in young calves, almost invariably is accompanied by marked ruminal tympany. In contrast, in adults the disease is common, but ruminal tympany is an infrequent sign of the disease. Purulent lung infections appear to be a common cause of bloat in calves, probably as a result of intrathoracic compression or irritation of the esophagus or possibly the vagal nerves.45 However, other causes of bloat that are associated with abnormal ruminal function are also common in calves with indigestion. They include overdistention of the rumen, insufficient clearing of the cardia, and inhibition of motility by abnormal fermentation products. Thus a thorough examination is necessary to determine the underlying cause of the individual case. Abomasal dilation and tympany in calves (acute bloat syndrome) is often associated with forestomach distention as well. Although the exact pathogenesis is unknown and appears multifactorial, large amounts of fermentable carbohydrate in the abomasum along with fermentative enzymes probably lead to gas production and bloat.103,120,136 This syndrome is discussed in detail elsewhere (see Chapter 20). One presumed cause of bloat in calves that is not a cause of adult bloat is sudden filling of the abomasum by milk feeding during weaning. Calves not yet completely converted to a diet of solid feed still consume milk eagerly. In some cases, acute free gas bloat occurs immediately after the milk feeding. Because the esophageal groove directs the milk into the abomasum but the abomasum is already partly filled by ingesta from the developing rumen, acute overdistention of the organ can occur and reflexly inhibit forestomach motility. Feeding smaller milk meals or discontinuing the milk feeding resolves the problem in these cases, which is evidence of the presumed cause.
More on the topic Indigestion in Ruminants:
-
Veterinarian -
|