Acute Renal Failure in Foals
Thomas J. Divers • Alexandra J. Burton • Lisa E. Fultz
Acute tubular necrosis (ATN) is the most common pathologic lesion causing ARF in neonatal foals. Many cases develop during or after episodes of diarrhea, likely caused by poor renal perfusion (vasomotor nephropathy) subsequent to varying degrees of dehydration.
Surprisingly, the diarrheal disease in some affected foals does not appear to be serious, but the foals may still develop ARF. Similar to adult horses with ARF, the prominent clinical signs are depression and development of edema. Abnormal laboratory findings include azotemia, hyponatremia, hypochloremia, and hypocalcemia. In foals with ARF, both serum BUN and potassium in ARF tend to be significantly higher than in foals with spurious hypercreatine- mia.96 Foals are more likely to develop significant hyperkalemia and hyperphosphatemia than are adult horses with ARF. A USG of less than 1.018 and microscopic hematuria are also typical of foals with ARF. Urine output of sick neonates should be monitored closely because they may become oliguric to anuric 12 to 24 hours before significant depression or azotemia is recognized. In addition, fluid retention during incipient ARF is another cause of inappropriate weight gain (e.g., >2 kg in 24 hours), which can often be detected before obvious edema or other clinical signs develop.Nephrotoxicity, most often due to aminoglycoside (AG), tetracycline, or NSAID administration, is a cause of ARF (usually nonoliguric) in neonatal foals, particularly those that are dehydrated. As in adult horses, the recent change to once-daily dosing appears to have decreased the incidence of AG-induced ARF in foals. Seriously ill and/or premature foals appear to be at even greater risk of nephrotoxicity than term foals, owing to reduced renal clearance.102 Although there is a general impression that amikacin may be less nephrotoxic than gentamicin in foals, no data exist to support this notion.
Regardless of which AG is selected, TDM (24-hour trough concentrations causes of CRF in one retrospective study of 99 horses with CRF.2 It is thought to result from deposition of circulating immune complexes along the glomerular capillaries or in situ formation of immune complexes along the glomerular basement membrane (GBM). Deposition of immune complexes causes activation of complement and vasculitis (type III hypersensitivity response). In one study, deposits of immunoglobulin (Ig)G and complement along the GBM were found through immunofluorescence (IF) staining in a large proportion (22/53) of horses at necropsy.3 However, only 1/53 horses had developed CRF. Thus, although immune (antigen-antibody) complex deposition and subclinical GN may be common in horses, progression to CRF appears to be an infrequent occurrence. In this necropsy survey, the predominant IF staining pattern was granular (patchy deposits of immune complexes and complement along GBM), but linear deposits were found in two horses.3 The latter finding was supportive of true autoimmune disease with more diffuse deposition of anti-GBM antibodies (type II hypersensitivity response) along the basement membrane.3 Streptococcal antigens and purpura haemorrhagica have been suggested as an important trigger for development of proliferative GN.4,5 In one report, a 12-year-old gelding developed CRF due to GN 3 months after a lower respiratory tract infection with Streptococcus Zooepidemicus.5 In this instance, group-C streptococcal antigens and IgG were confirmed to be present in diseased glomeruli at necropsy.5 Equine infectious anemia (EIA) virus is the only other antigen that has been detected in glomeruli of horses with proliferative immune- mediated GN.6 However, diffuse subclinical GN likely accompanies many other chronic infections in horses. It has also been suggested that equine GN may also be associated with either mixed or monoclonal cryoglobulins forming antibody-antibody and/or complement glomerular deposits resembling human cryoglobinemia.7 In one horse, with no evidence of viral or bacterial infection, deposits consisting solely of IgM were identified within the GBM.8Chronic Interstitial Nephritis
Chronic interstitial nephritis (CIN) and fibrosis are probably the most common causes of CRF in older horses.
In one retrospective study of 99 horses with CRF, CIN accounted for 39% of acquired cases of CRF.2 Interstitial nephritis (tubulointerstitial disease) usually develops as a long-term sequela to ATN caused by nephrotoxins or vasomotor nephropathy. Other causes of CIN include drug-induced interstitial nephritis, urinary obstruction, pyelonephritis, renal hypoplasia/ dysplasia, and papillary necrosis. Although the majority of horses that develop ARF attributable to these causes recover with apparently normal renal function (they remain nonazo- temic), a few may survive with significant loss of renal functional mass and subsequently (often years later) develop signs of CRF due to CIN.9 In horses younger than 5 years of age that develop CRF unattributable to other causes, anomalies of development (e.g., renal hypoplasia, dysplasia, polycystic kidney disease [PCKD]) should be strongly suspected.2,10-13Pyelonephritis
Bilateral septic pyelonephritis is a rare cause of CRF in horses.14-16 Pyelonephritis is usually due to an ascending infection and is often accompanied by nephrolithiasis or uretero- lithiasis. However, in septic neonatal foals, it may occur due to hematogenous bacterial seeding of the kidneys. Multiparous mares (especially those with a history of dystocia) and horses with bladder paralysis are at greater risk for lower urinary tract infection (UTI) and subsequent development of ascending upper UTI. Bladder paralysis with chronic distention compromises the integrity of the ureteral orifices and leads to vesiculoureteral reflux and pyelonephritis. If paralysis is longstanding, ureteral orifice(s) may appear wide open on cystoscopy and, occasionally, the scope can be advanced into the ureter with little resistance. With unilateral pyelonephritis, adequate renal function is usually maintained by the contralateral kidney. Gram-negative organisms appear to be the most common causative agents, although Staphylococcus, Streptococcus, or Corynebacterium spp.
may be isolated and mixed bacterial infections are not uncommon (see the Urinary Tract Infections section later).Miscellaneous Causes
Other reported causes of CRF in horses include amyloidosis, neoplasia, focal glomerulosclerosis-like disease, and chronic oxalate nephrosis.17-20 One study described CRF secondary to PCKD in an aged pony with hematuria; the pony also had hepatic cysts.21 Renal amyloidosis has only been reported in horses used for production of antiserum.17 So-called oxalate nephropathy in horses is likely a misnomer; the presence of oxalate crystals in renal tissue of horses with CRF is typically a consequence rather than the cause of CRF.20
Clinical Signs and Laboratory Findings
The most common presenting complaint in horses with CRF is weight loss.2 A small plaque of ventral edema, usually between the forelimbs, is another frequent finding.1,2,22 Moderate polyuria and polydipsia (PU/PD) are often present but may not be noticed except by the astute owner or trainer.1,2 Rough hair coat, partial anorexia, and poor performance are also reported.1,2 Dysuria is generally not reported unless CRF is due to pyelonephritis, which may be associated with bladder paralysis, urolithiasis, and lower UTI. Hematuria ± pyuria (gross or microscopic) may be present in some (but not all) horses with pyelonephritis, urinary calculi, renal hypertension, or neoplasia. Urine produced by horses with CRF is often light yellow and transparent because it is relatively devoid of crystals and mucus.

FIG. 34.2 Dental tartar caused by chronic azotemia in a 5-year-old Standardbred with chronic renal failure.
Accumulation of dental tartar (especially on the incisors and canine teeth [Fig. 34.2]), melena, and oral ulcers may also be found in horses with CRF. Growth may be stunted in horses with renal hypoplasia, dysplasia, or PCKD.
Colic signs are variable in horses with nephrolithiasis or urolithiasis producing obstruction of the upper urinary tract and may or may not be (intermittently) present.9,23 Rarely, signs of uremic encephalopathy such as obtundation, anxiety, head pressing, and seizure may be present, but this is more common with severe, fulminant ARF.24,25Clinicopathologic findings in horses with CRF vary depending on appetite, diet, cause, and severity of renal damage. Most horses with clinical signs of CRF have moderate to severe azotemia (serum or plasma creatinine usually ≥5 mg/dL). The serum or plasma BUN-to-creatinine ratio may vary depending on protein intake, muscle mass, hydration, and degree of azotemia but is usually greater than 10 : 1.2 Mild hyperkalemia, hyponatremia, and hypochloremia are typically found in horses with CRF. Hypercalcemia, with serum concentrations sometimes greater than 20 mg/dL, appears to be a laboratory finding with CRF that is unique to the equid. One study of horses evaluated at referral hospitals for renal failure reported 56% of 39 horses with CRF to be hypercalcemic, and a larger study of 99 horses with CRF found 67% to be hypercalcemic.2,26 Hypercalcemia in horses with CRF is not due to hyperparathyroidism; its presence or absence appears to be more closely related to dietary intake than to the magnitude of azotemia.27 For example, 4/4 bilaterally nephrectomized ponies fed alfalfa hay developed marked hypercalcemia, whereas serum calcium concentration remained within the normal range in 4/4 bilaterally nephrectomized ponies fed grass hay.28,29 Similarly, hypercalcemia in horses with spontaneously occurring CRF can resolve within a few days of changing diet from alfalfa to grass hay. Serum phosphorus concentration in horses with CRF is usually normal to low, and hypophosphatemia is more often detected with concurrent hypercalcemia. Hypermagnesemia may also be detected in some horses with CRF.
Acid-base balance usually remains normal until CRF becomes advanced, but metabolic acidosis is a common finding in horses with eskd.Many horses with CRF are moderately anemic secondary to decreased erythropoietin production by the diseased kidneys. Those with CRF resulting from GN frequently have hypoal- buminemia and hypoproteinemia. Horses with advanced CRF due to any cause may also have mild hypoproteinemia associated with GI ulceration. Hyperglobulinemia may be detected in horses with immune-mediated diseases or chronic pyelonephritis. Horses with CRF can also develop hypercholesterolemia and hypertriglyceridemia (hyperlipidemia), and with advanced CRF may occasionally have grossly lipemic plasma.30
Urinalysis varies depending on the cause of CRF but is usually relatively devoid of normal mucus and crystals and thus may appear more transparent than normal equine urine. Isosthenuria is typical (USG = 1.008 to 1.014), although heavy proteinuria in GN cases may produce USG values up to 1.020. Laboratory quantification of urine protein concentration (rather than a dipstick) is required to accurately assess proteinuria. Urine protein concentration in normal horses is usually less than 100 mg/dL, and the urine protein (UPro)-to-creatinine (UCr) ratio is less than 1: 1.31,32 With significant proteinuria, the UPro:UCr ratio is usually greater than 2: 1.5 In the earlier stages of GN, excessive urine protein is primarily albumin, but with progression of glomerular pathology an increasing amount of globulin is also lost in the urine. Horses with CIN usually do not have significant proteinuria. Hematuria (gross or microscopic) can produce trace proteinuria, but the UPro:UCr ratio usually remains less than 2 : 1. Horses with septic pyelonephritis would be expected to have pyuria (>5 leukocytes/ high-power field) and significant bacteriuria on sediment examination, but these findings are not consistently detected; a urine sample should be submitted for quantitative bacterial culture in all horses with CRF.
Diagnosis
A diagnosis of CRF is most often made in horses with azotemia and isosthenuria that present with a complaint of weight loss and/or decreased performance. Determining the inciting cause of CRF can be difficult because the disease has often advanced to ESKD when horses are initially presented for evaluation, although a detailed long-term history can help. Trends in serum creatinine and body condition score over weeks to months probably provide the most useful prognostic information in the horse with CRF. Urinalysis does not often reveal the cause of CRF except in some horses with pyelonephritis. Assessment of urine protein concentration and UPro:UCr ratio should be helpful in separating glomerular disease from tubulointerstitial disease, but in practice these laboratory measures have not consistently been elevated in horses with histopathologic evidence of GN. However, detection of moderate to heavy proteinuria (UPro:UCr ratio >2 : 1), without hematuria, provides support for glomerular disease.29
Rectal examination may be helpful as horses with pyelonephritis and/or ureteral calculi often have enlarged ureters that can be palpated dorsolaterally in the retroperitoneal space. Although kidneys of horses with CRF are often small with an irregular surface, these changes are not always apparent on palpation of the caudal pole of the left kidney per rectum. The right kidney cannot usually be palpated in the horse unless it is greatly enlarged or displaced caudally by the liver or a mass. US is useful for evaluating kidney size and echogenicity, and it may reveal fluid distention (indicating hydronephrosis, pyelonephritis, or PCKD) or presence of nephroliths.33-35 Horses with significant renal parenchymal damage and fibrosis often have loss of detail of the corticomedullary junction, and echogenicity of renal tissue may be similar or even greater than that of the spleen (Fig. 34.3, A). The contralateral kidney may be normal or hypertrophic in cases with unilateral kidney disease (Fig. 34.3, B). Intravenous pyelography (IVP) provides little information in adult horses and is generally limited to foals less than 50 kg. When hematuria or dysuria accompanies CRF, cystoscopic examination can be helpful in determining from which kidney(s) hematuria is originating and allows assessment of ureteral orifice size and urine flow. A single case report of a stallion with hematuria due to unilateral nephritis described severe renal hypertension secondary to fibrotic constriction of the renal vein.36 Nephrectomy of the affected kidney was curative in that stallion.
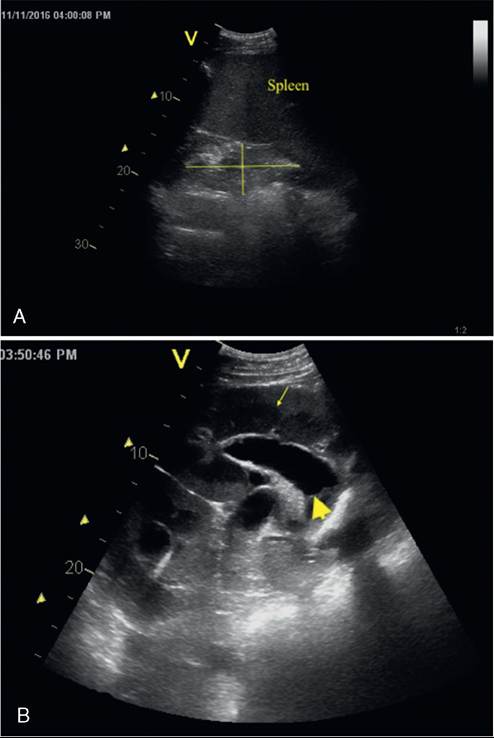
FIG. 34.3 A, Ultrasonographic image of the left kidney in a 4-year-old Quarter Horse gelding with chronic renal failure secondary to unilateral renal hypoplasia and exposure to nephrotoxic agents in the 6 months before onset of clinical signs (weight loss, polyuria, and polydipsia). The left kidney is measured in the 17th intercostal space (ICS) and is small (10.5 cm length ? 5.8 cm width; reference range: 12.6 ± 2.2 cm length ? 7.9 ± 1.1 cm width), hyperechoic relative to the spleen, and has a loss of corticomedullary distinction. B, Ultrasonographic image of the right kidney in the same horse measured in the 16th ICS is enlarged (23 cm length ? 9 cm width; reference range: 16.0 ± 0.7 cm ? 7.9 ± 1.0 cm width), with a distended renal pelvis (wide arrow) and distinct hyperechoic and widened renal cortex (arrow) (2.0 cm; reference range 1.3 to 1.6 cm). This kidney was suspected to be hyperplastic.
Measurement of GFR provides the most accurate assessment of renal function, and repeated measurements at monthly (or longer initially) intervals can be useful to monitor rate of progression of CRF and thus prognosis and remaining lifespan. It is also a useful measure to document a reduction in renal function in horses that are thought to have early CRF, before significant azotemia has developed. Measurement of GFR can be by several methods, including urinary clearance of endogenous or exogenous creatinine, inulin, or technetium-99m diethylenetriamine pentaacetic acid (99mTc-DTPA) (all require timed urine collections), and plasma disappearance of sodium sulfanilate, phenolsulfonphthalein, or radiolabeled compounds (e.g., 99mTc-DTPA).13,37-40 Assessment of renal function by nuclear scintigraphic imaging of the kidneys has also been described, but in horses this technique appears to be better for documenting decreased individual kidney function (i.e., with unilateral disease) than for quantitative assessment of GFR.40,41 In most clinical settings, performing a 24-hour endogenous creatinine clearance is the most practical and economical method for measuring GFR. The major challenge is application of a urine collection device for collection of all urine produced, via a method that does not pose a risk of introducing ascending infection into the urinary tract. Once urine has been collected, a well-mixed sample is submitted to the laboratory, along with a sample of serum obtained during the collection period, and GFR is estimated by the following standard clearance formula:
GFR(mL ∙ kg 1 ∙ min 1) = {([Crurine]∕[Crsenm])} ? UF/bwt where UF is urine flow (mL min-1) and bwt is body weight in kilograms.38,39 In horses with normal renal function, GFR ranges from 1.5 to 3.0 mL/kg/min, and values 116 mm Hg).45
The inciting cause of CRF can sometimes be confirmed by renal biopsy. Renal biopsy should be approached somewhat cautiously and pursued only if findings are likely to change treatment or prognosis. However, a recent multicenter study on equine renal biopsies found that histopathologic diagnosis by biopsy had a 72% agreement with histopathology at necropsy.46 This same study found a complication rate of 11.3%, generally associated with hemorrhage or signs of colic, and there was only one fatality.46 Risk factors for complications included biopsy of the left kidney, a diagnosis of neoplasia, and low USG.46
Treatment
Treatment of horses with CRF is most likely to produce improved renal function if there is an acute reversible component exacerbating CRF (i.e., acute-on-chronic disease). Similar to ARF, sudden exacerbation can be caused by exposure to nephrotoxins or vasomotor nephropathy secondary to diseases producing hypovolemia (e.g., diarrhea). Ascending UTI or obstruction can also exacerbate CRF. If an acute component is detected, it should be corrected rapidly (as described for ARF) with the goal of minimizing further loss of functional nephrons. In addition, surgical removal or fragmentation of stones may be indicated in horses with calculi thought to be disrupting urine flow.
In horses with relatively stable CRF, management changes should be kept to a minimum and, when necessary, made gradually. Treatment of horses with stable CRF consists of supportive care: fluids, electrolytes, and nutritional support. Water should be available at all times, and salt can be provided freely so long as edema and/or hypertension are absent. If edema develops, salt should be restricted, even in the face of hyponatremia. In addition to serum creatinine, electrolyte concentrations and acid-base balance should be measured regularly (e.g., monthly or initially longer intervals). If serum sodium and chloride concentrations are decreased, 60 to 120 g (≈2 to 4 oz) of salt may be added to the feed, provided edema is not present. If metabolic acidosis is detected (e.g., blood pH be remembered that if the horse with CRF becomes anorectic or will eat very little, quality of life is an important factor to consider.
Additional treatments for CRF in human patients include antihypertensive agents, including diuretics, β-adrenergic blockers, and ACE inhibitors.54 The ACE inhibitors may have an additional benefit of limiting proteinuria.55 In dogs and cats, ACE inhibitors and/or angiotensin receptor blockers are considered standard of care for managing chronic kidney disease with proteinuria.56 Little is known about the roles of systemic or intrarenal hypertension in progression of renal disease in horses. There are no research reports of potential benefits of use of antihypertensive medications in horses with CRF. Oral administration of the ACE inhibitor benazepril was evaluated in healthy horses following exogenous administration of angiotensin 1 and modestly attenuated a rise in systemic blood pressure at a dose of 1 mg/kg.57 Future studies are needed to determine the optimal dose, frequency, safety, and efficacy for horses with CRF.57
Horses with end-stage CRF often develop oliguria and uncontrollable metabolic acidosis. At this stage, CRF can only be managed by hemodialysis or peritoneal/pleural dialysis. However, pursuit of either hemodialysis or peritoneal dialysis in horses with CRF is of questionable logic because even when successful, dialysis is likely to prolong the life of the horse for only a short time.
Prognosis
As soon as the diagnosis of CRF is made, the owner should be made aware that it is a terminal condition, so as to prepare him or her well in advance for making the decision to euthanize on humane grounds at the appropriate juncture, most likely within 2 years after the diagnosis of (stable) CRF. With patient- tailored management and monitoring, many horses with early CRF may be able to continue in performance or live as a “pasture pet” for months to a few years. In general, as long as creatinine remains less than 5.0 mg/dL and the BUN-to- creatinine ratio is less than 15 : 1, affected horses seem to maintain a reasonably good attitude, appetite, and body condition. Once creatinine is greater than 5.0 mg/dL, the rate of progression of CRF appears to accelerate and signs of uremia (e.g., anorexia, poor hair coat, loss of body condition) often become more apparent. Although this threshold for creatinine concentration is a useful figure for informing an initial prognosis for most horses, it is important to remember that progression of CRF is highly variable. Thus, each case must be handled on an individual basis, with the emphasis on maintenance of body condition until humane euthanasia becomes necessary.