Urinary Tract Infections
Thomas J. Divers • Dominic R. Dawson-Soto • Alexandra J. Burton
UTI can be anatomically divided into two categories: those affecting the upper urinary tract (kidneys and ureters) and those involving the lower urinary tract (bladder and urethra).
Lower UTI usually results from anatomic or functional causes of abnormal urine flow, especially bladder paralysis (see Urinary Incontinence section later). Although recognized less frequently, upper UTI is often a more serious, potentially life-threatening problem. In horses, UTI is also frequently accompanied by urolithiasis and partial obstruction.1Risk Factors and Causes
The most common risk factors for development of UTI are bladder paralysis, urolithiasis, and urethral damage (e.g., foaling trauma in mares, neoplasia or habronemiasis in males). However, in the case of urolithiasis, with the exception of single large cystoliths (which predispose horses to lower UTI), it is often difficult to determine whether concurrent nephroliths, ureteroliths, multiple small cystoliths, and/or urethroliths are a cause or consequence of UTI. The shorter urethra and its location near the anus can increase the risk of lower UTI in mares and fillies. One study in healthy horses showed that mares had significantly more colony-forming units (CFUs) of bacteria in their urine than males.2 In humans, silent lower UTIs and pyelonephritis resulting from infection with bacteria shed from the GI tract can develop in prepubertal girls and during pregnancy or after menopause in adult women.3 In certain instances, this increased risk has been further attributed to a lack of estrogen, which appears to be important for production of glycosaminoglycans that cover uroepithelial surfaces and inhibit attachment of bacteria.4 Whether fillies or pregnant mares are at increased risk for UTI has not been studied.
Horses with bladder paralysis or decreased urethral sphincter tone are at greater risk of UTI. Immunosuppression should also be considered an important risk factor, especially in today's aging equine population (i.e., if uncontrolled pituitary pars intermedia dysfunction [PPID] is present). Finally, as bladder catheterization cannot be performed in a completely sterile manner due to normal bacterial flora in the vestibule and distal urethra, iatrogenic lower UTI is a risk of this procedure. However, UTI is an unlikely complication of bladder catheterization in otherwise healthy animals because host defense mechanisms, including urine flow, are highly effective in eliminating contaminating bacteria. When urethral or bladder mucosa has been damaged or urine stasis (e.g., bladder paralysis) is present, bladder catheterization has a greater risk of producing UTI.Bacterial UTI is most common. In one study on urine from healthy male and female horses, multiple bacterial species were cultured, regardless of whether urine was obtained via midstream free catch or catheterization, with the predominant isolates being Streptococcus spp., E. coli, Enterobacter sp., Bacillus sp., Staphylococcus spp., Diptheriods sp., Proteus spp., and Enterococcus sp.2 In one author's experience (TJD), E. coli, Proteus mirabilis, Klebsiella spp., and Enterobacter spp. are the most common pathogens isolated from individual horses with UTI. Historically in the literature, E. coli, Staphylococcus spp., Corynebacterium spp., Streptococcus spp., and Pseudomonas aeruginosa were the microbes isolated most frequently from horses with UTI.5,6 A more recent study found E. coli (36%), Streptococcus spp. (20%), and Enterococcus spp. (20%) in urine cultures from equine clinical cases.7 In a group of seven horses with pyelonephritis, Pseudomonas aeruginosa, E. coli, and Streptococcus zooepidemicus were cultured.8 Individual case reports of cystitis in horses due to Corynebacterium matruchotii infection and a combined E.coli and Enterococcus spp.
infection have also been described.9,10 In horses with instrumentation of the urinary tract (e.g., indwelling bladder catheters, ureteral stents), UTI with nosocomial, antimicrobial-resistant pathogens should always be considered a risk. In septicemic foals, hematogenous infection of the kidney(s) with Actinobacillus spp., Rhodococcus equi, and Salmonella spp. has occurred.11-13 Lower UTI with yeast (Candida spp.) occurs in neonatal foals receiving broad-spectrum antibacterial therapy, especially if they are recumbent and/or have indwelling urinary catheters. The spirochete Leptospira interrogans caninfect the equine kidney, occasionally causing acute interstitial nephritis, but it is more commonly implicated in uveitis and abortion.14
Equine parasitic UTIs do not commonly cause clinical disease. The coccidian parasite Klossiella equi infects the renal parenchyma of equids but has only been reported to cause disease (interstitial nephritis and tubular necrosis) in instances of heavy infection or host immunosupression.14-18 The nematode Halicepbalobus gingivalis is primarily a cause of equine neurologic disease (meningoencephalitis) but may also result in granulomatous nephritis via hematogenous spread.14,19-21 Both K equi sporozoites and H. gingivalis parasites can sometimes be found in the urine sediment of infected animals.’’’ !here is one report of two horses developing tubularinterstitial nephritis in association with productive, lytic equine polyomavirus infection.22 The etiopathogenesis in these two horses was hypothesized to be similar to BK polyomavirus nephropathy of immunocompromised humans.22,23 In horses without any obvious predisposing factor for UTI, primary immune dysfunction or other immunocompromise (e.g., uncontrolled PPID) should be considered, especially in cases where uncommon pathogens are identified as causative agents. ,, Sterile ulcerative cystitis due to phenylbutazone administration has been reported.24 In addition, a newly described entity of equine sterile idiopathic hemorrhagic cystitis was recently documented in a cases series of 11 horses (see the Urinary Tract Neoplasia section later).25
Clinical Findings
Clinical signs of UTI usually reflect the location, severity, and duration of infection.
Lower UTI seldom causes signs of systemic illness and infection and is typically characterized by disturbances in urine flow (dysuria, dysuria, stranguria, pol- lakiuria, and incontinence). An exception to this is in mares with subclinical cystitis/urethritis, where outward signs may not be present or recognized. Urine scalding of the perineum may develop with chronic UTI in mares but should not be confused with estrus or fecal crusting/scalding due to diarrhea or a sunken anus (poor conformation or as a result of low body condition score). The sheath opening and dorsal aspects of the hindlimbs may be coated with urine crystals or blood in males with UTI. In an occasional horse, gross pyuria may also be observed as passage of mucopurulent debris in otherwise clear urine but should not be confused with the normal turbid appearance of equine urine (see Chapter 10, Fig. 10.2). Gross hematuria can be seen with urinary calculi, neoplasia, or if the bladder and/or urethral mucosa is eroded or very inflamed. Hematuria of bladder origin typically produces hematuria throughout urination, with gross discoloration of urine most obvious at the end of urination. Hematuria can also be caused by upper urinary tract hemorrhage. Renal hemorrhage was a major component of bacterial pyelonephritis reported in seven horses and has also been seen with clinical K. equi infection.7,15 Horses with upper UTI are much more likely to have signs characteristic of a systemic infection, including fever, inappetence, lethargy, colic, and weight loss. However, because upper UTI is often accompanied by concurrent lower UTI, dysuria may also be present.Diagnosis
A diagnosis of UTI is based on clinical signs, analysis of blood and urine samples, US, and cystoscopy. With lower UTI, the complete blood cell count (CBC) and serum biochemical profile are usually normal, whereas the CBC with upper UTI often supports a systemic inflammatory response. Detection of azotemia, low USG, and white blood cell (WBC) casts in urine sediment are indicative of upper UTI, especially when accompanied by signs of systemic illness.
With chronic upper UTI, increased total protein and globulin concentrations are also often detected. In human medicine, pyuria (increased number of WBCs in the urine) is defined as the presence of greater than 10 WBCs per mm3 urine or greater than or equal to three WBCs per microscopic high-power field (HPF).26 In horses, to the author's (AJB) knowledge, there has been no peer-reviewed study specifically assessing the cellular content of urine in a large number of healthy adult horses. However, in horses, pyuria is generally considered to be the presence of greater than 10 WBCs per HPF of a midstream-voided or catheterized sample, with the urine of healthy horses generally said to have fewer than five WBCs per HPF.27 That said, one study in healthy males and females found that no horse had a WBC count greater than one per HPF in midstream free catch sample.2 This suggests that the generally accepted number of greater than 10 WBCs per HPF to diagnose pyuria may be too high for horses, and it should be diagnosed if greater than five WBCs per HPF are seen, providing collection is aseptic or midstream and there is clinical suspicion of urinary tract disease. When bacterial infection is the cause of pyuria, there are typically more than 20 organisms visible per HPF. Urine samples should be examined and processed for bacterial culture within 30 minutes after collection or be refrigerated because bacteria can continue to proliferate when urine is stored at room temperature. Culture results should be interpreted in light of the clinical picture, as not all organisms cultured may be causative and some may be innocuous contaminants.Rectal examination and transrectal US may help confirm a predisposing cause of lower UTI (e.g., enlarged and atonic bladder, cystic calculi, bladder mass). Chronic cystitis also usually leads to bladder wall thickening, visible via US.25 The ureters are not usually palpable during rectal examination of the normal horse, but in horses with upper UTI, careful palpation of the dorsolateral aspects of the caudal abdomen (retroperitoneal space) usually reveals enlarged ureters, and transrectal US can help confirm this finding.
With pyelonephritis, rectal palpation may further reveal an enlarged, painful, or shrunken and misshapen left kidney, while the right kidney is usually not palpable. Transabdominal US of the kidneys is useful for detecting abnormal renal size, shape, or consistency in horses with upper UTI.8,27-32 Horses with pyelonephritis may have a focus of septic infection with adjacent dilation of the renal pelvis (Fig. 34.4), which may be detected by US if it distorts renal architecture and echogenicity sufficiently.Cystoscopic examination of the lower urinary tract is useful for evaluating the integrity of urethral and bladder mucosa, detecting small uroliths, and assessing urine flow from each ureteral orifice.1,8,27,32 With long-standing cystitis, especially when bladder paralysis is the underlying cause, ureteral orifices may become dilated (and appear wide open), allowing for vesiculo-ureteral reflux and development of ascending pyelonephritis. When unilateral pyelonephritis is suspected on the basis of US findings, cystoscopy with catheterization and collection of urine samples individually from each ureter can be helpful to document unilateral disease. Ureters may be catheterized by passing sterile polyethylene tubing through the biopsy channel of the endoscope during cystoscopy or can be accomplished in mares by directing blunt-ended catheters (e.g., 8-Fr polypropylene) through the urethra into each ureteral orifice.33
Treatment
Treatment of UTI consists of proper antimicrobial therapy and correction, if possible, of predisposing anatomic or functional causes. Selection of the appropriate antimicrobial agent is best determined by prior knowledge of susceptibility patterns of the causative pathogen(s), concentration of the antimicrobial in renal tissue and urine, activity of the antibiotic at different pH values, toxicity, compatibility with other antimicrobial drugs, ease of administration, and expense. In addition, with
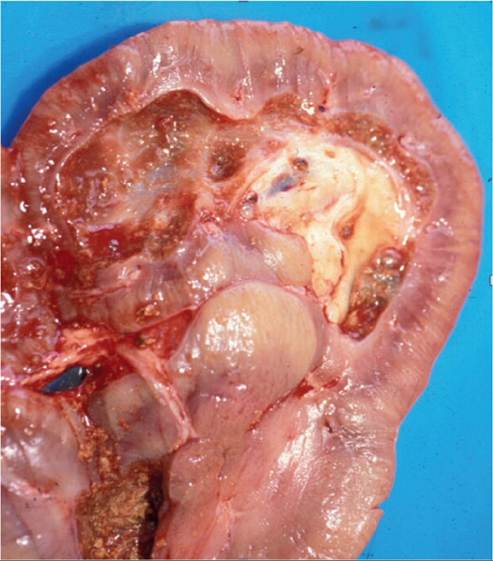
FIG. 34.4 A transected kidney from a horse with pyelonephritis. Note the severely dilated renal pelvis adjacent to a septic purulent focus. (Courtesy The University of Pretoria, Faculty of Veterinary Science.)
the increasing emergence of antimicrobial-resistant pathogens, especially within hospital settings, antimicrobial stewardship through rational antimicrobial therapy is vital (see Chapter 45). Resistance in vitro to a particular antibiotic may not preclude successful treatment with the drug, providing high enough concentrations are achieved in urine. Similarly, in vitro susceptibility does not always guarantee a successful response to treatment. Penicillin, ampicillin, cephalosporins, trimethoprim-sulphonamide (TMS), and gentamicin are all concentrated in urine. The antimicrobials of choice for horses with lower UTI are TMS or ceftiofur, or a broad-spectrum combination (i.e., penicillin or ampicillin or ceftiofur, plus gentamicin or amikacin).34 Gentamicin and amikacin should be avoided in patients with severe azotemia or suspected renal failure, as these are potentially nephrotoxic. Fluconazole is the antifungal drug of choice for UTI involving Candida spp.34 Treatment should be continued for 7 to 14 days and then urine recultured. For upper UTI (pyelonephritis), TMS, ceftiofur (or other third-generation cephalosporins), penicillin or ampicillin, or enrofloxacin are the antimicrobials of choice.34 Therapy for upper UTI is usually required for 2 to 3 weeks and often longer.34 Although less of a risk with newer preparations, horses with acidic urine, dehydration, or poor renal perfusion may develop hematuria and crystalluria with sulfonamides.35 With presumed lower UTI, if the UTI recurs and the same organism is isolated, a focus of upper UTI should be suspected. In contrast, recurrence of UTI with a different pathogen suggests an anatomic or functional cause of abnormal urine flow as a predisposing cause of UTI.
Although unstudied in horses, the use of lactobacillus suppositories in women predisposed to UTI enhanced cure rates in some studies but showed no efficacy in others.32,36,37 Preliminary research on vaccines against bacterial virulence factors to reduce the incidence of UTIs in predisposed populations of humans and mice appears promising.38 There is no research into these alternative therapies in horses to date.