Cerebrospinal Fluid
Mary O. Smith • Lisle W. George • John R. Middleton
Cerebrospinal fluid (CSF) is partly derived from and in equilibrium with the extracellular fluid that bathes the brain and spinal cord parenchyma.1-4 The composition is an indicator of the state of the intrathecal contents.
CSF is produced by a combination of ultrafiltration of plasma and active secretion.5 The sites of CSF production are the choroid plexuses of the lateral, third, and fourth ventricles; the ependymal lining of the ventricular system; the pia arachnoid; and the meningeal blood vessels. The CSF in the ventricular system flows caudally and diffuses out of the lateral apertures in the fourth ventricle. It then circulates around the brain and spinal cord. Circulation of CSF is achieved through regional pressure changes caused by spinal motion and pulsations of blood vessels. CSF is resorbed from both the cranial cavity (75%) and the spinal canal (2 5%).6 Some resorption of brain CSF occurs at the arachnoid villi that are near large veins and sinuses, but most resorption occurs at the cribriform plate, into nasal lymphatics.7,8 Spinal CSF is resorbed into the lymphatic vessels near spinal nerves.The predominant direction of CSF flow in the spinal canal is cranial to caudal. CSF specimens can be collected from the cisterna magna when the site of interest is the brain, whereas it should be collected from the lumbar subarachnoid space when the lesion is in the spinal cord. In large animals, however, the risks associated with the general anesthesia required for cisterna magna tap are considerable, and so lumbar puncture is usually the most suitable technique for CSF collection in these species, regardless of the site of the lesion.9,10
Collection of Cerebrospinal Fluid
Lumbosacral Spinal Tap
For collection of CSF by lumbosacral puncture, the animal is lightly sedated, and the skin of the dorsal midline over the junction of the sixth lumbar (L6) and first sacral (S1) vertebrae is surgically prepared (Fig.
35.1). A variety of standard sedative protocols are suitable; xylazine has been shown to reduce CSF pressure.11 Correct placement of the spinal needle is more easily achieved when the animal is standing. The proper anatomic site for insertion of the spinal needle is between the dorsal spinous process of L6 cranially and S1 caudally and the two tuber sacrales laterally. The overlying skin forms a depression that can be revealed by palpation, although this may be difficult in well-muscled animals. The correct site for needle placement can also be determined by locating (1) the dorsal midline at the highest point of the quarters or (2) the point where an imaginary line drawn between the caudal aspects of the two tuber coxae intersects the midline.The skin is anesthetized with 2% lidocaine, and a 1-cm incision is made with a No. 15 scalpel blade. Alternatively, the skin can be punctured with a 14-gauge needle and the needle removed or left in place as a guide through which the spinal needle is passed. In adult horses and cattle, a 6- to 9-inch, 18- to 20-gauge spinal needle is inserted perpendicularly through the incision (or 14-gauge needle) and advanced, usually with the stylet seated, until the tip punctures the lumbosacral cistern. For small ruminants, foals, and calves, a 3.5-inch needle can be used. Use of hypodermic needles for CSF collection is discouraged because they have a cutting surface on the end; such a surface is absent on spinal needles. A “snapping” sensation is sometimes felt as the needle passes through the interarcuate ligament. The patient may reflexively contract the tail, anus, and gluteal muscles. Some patients, particularly horses, may respond with violent motor activity. Therefore a lumbosacral spinal tap performed on a conscious horse should be done only when the animal is restrained in stocks. The average depth of insertion is 17.64 cm (7 inches) in adult horses, 8.26 cm (3.3 inches) in ponies,10 and approximately 7.5 to 10 cm (3 to 4 inches) in adult cattle.
The spinal needle is advanced gently to the floor of the spinal canal. Passage of the needle through the terminal spinal cord or the cauda equina does not cause subsequent neurologic abnormalities. When the needle is seated in the spinal canal, the stylet is removed, and fluid is allowed to drip from the hub into a sterile tube, or gentle negative pressure can be applied to withdraw spinal fluid into a series of 3-mL syringes. If frank blood is obtained, the tip of the needle is probably in one of the ventral vertebral sinuses. The needle should be withdrawn a few millimeters, and a clean syringe should be attached to the hub. Compression of the jugular vein causes engorgement of the ventral vertebral plexus, which increases CSF pressure in the lumbosacral cistern.
Cisterna Magna Tap
General anesthesia is required for a cisterna magna tap. After the patient has been anesthetized, the dorsal area of the neck overlying the atlanto-occipital joint is surgically prepared. The patient's head is held flexed at a right angle to the neck, with the sagittal plane of the head parallel to the floor or table on which the patient is lying. The head must not be allowed to
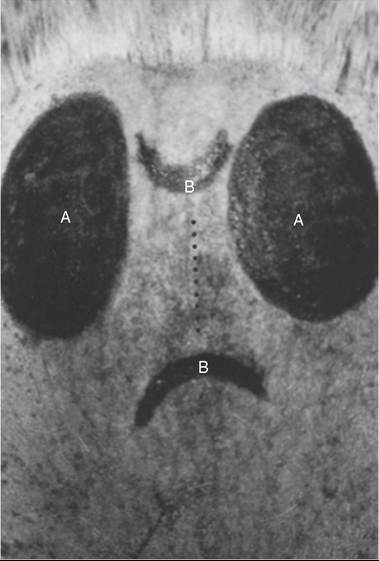
FIG. 35.1 Close-up view of landmarks for a lumbar cistern puncture in a horse. The large dark ovals (A) represent the position of the two tubers sacrale. The smaller curved lines (B) represent the respective caudal and cranial aspects of the L6 and S1 dorsal spinal processes. The dotted line represents the optimum area for placement of a skin stab.

FIG. 35.2 View of the ideal area for a cisterna magna cerebrospinal fluid tap in a cow. The two lines (a) represent the wings of the atlas. The large spot in the center (b) is the optimum area for needle insertion. Use of anesthesia and restraint is essential to prevent head movement.
move while the needle is inserted. The needle is inserted 1 to 2 cm caudal to a point, usually 6 to 9 cm (2.5 to 3.5 inches) from the poll (Fig. 35.2), that corresponds to the intersection of the dorsal midline, and a line is drawn between the cranial aspects of the wings of the atlas. A 3.5-inch, 18-gauge spinal needle is inserted perpendicular to the skin and aimed toward the nose. The needle is advanced slowly with the stylet seated. After the needle has been advanced a few millimeters, the stylet is removed, and the hub of the needle is examined for CSF flow. The stylet is replaced if it is dry and CSF is not spontaneously dripping from the hub, and the needle is advanced another few millimeters and checked again for CSF flow. Entry of the tip of the needle into the cisterna magna may be accompanied by the sensation of “popping” through a tissue plane or by a sudden decrease in resistance to the advancement of the needle. In other cases, no such sensation is perceived; thus CSF flow must be checked every time the needle is advanced a few millimeters.
In most adult large animals, the needle is seated at approximately 5 to 8.75 cm (2 to 3.5 inches). While the needle is advanced, the heel of the hand should be held firmly against the patient's neck to minimize the possibility of spinal cord injury. The mean depth of insertion is 6.5 cm (2.5 inches) in adult horses10 and 5 cm (2.25 inches) in adult cattle. In a cisterna magna tap, the needle entry site is close to the cervical spinal cord and brainstem. To minimize the danger of central nervous system (CNS) damage during a cisterna magna tap, the patient should be adequately anesthetized and ventilated because an increase in the partial pressure of carbon dioxide (PCO2) results in an elevation in intracranial pressure.12 Removal of fluid from the cisterna magna is contraindicated in a patient with increased intracranial pressure because the brain may herniate through the foramen magnum, which could be fatal. Signs of increased CSF pressure include a moderate to marked decrease in mentation, mydriatic pupils, opisthotonos, extensor rigidity, ventrolateral strabismus, and papilledema.
Ultrasonography can be used as an aid to needle placement for collection of CSF from both the atlanto-occipital cistern and the lumbosacral subarachnoid space.13,14
Myelography
Contrast material for myelography is injected into the cisterna magna in large animal patients. Withdrawal of CSF before injecting the contrast medium is unnecessary, as is reinjection of CSF after it has been withdrawn. The turnover of CSF is rapid and under strict homeostatic control; therefore withdrawal of CSF through a spinal tap does not have deleterious effects that necessitate its replacement.15-17
Analysis of Cerebrospinal Fluid
The color of the CSF should be noted as it flows from the hub of the spinal needle. Blood can originate from the tapping procedure (iatrogenic hemorrhage) or from a traumatic CNS lesion. Iatrogenic hemorrhage is usually unevenly mixed in the CSF and disappears as the fluid drips from the needle. Fluid collected immediately after placement of the spinal needle tends to be mildly contaminated with blood even when this is not apparent grossly. Subsequent aliquots are usually less contaminated, and so the later aliquots are most suitable for cellular and protein analysis.18 Blood from CNS hemorrhage is evenly mixed with CSF even after a large amount has been removed. Hemorrhage that occurred days earlier may have a brownish rather than red discoloration. Prior hemorrhage also results in xanthochromia, a yellow discoloration of the CSF. Xanthochromia can be observed in the CSF for at least 10 days after the introduction of blood. Xanthochromic samples do not contain bilirubin.
The normal values for CSF are presented in Table 35.1. Cell counts should be determined in a noncentrifuged specimen as soon as the sample is collected, with the use of a hemocytometer. Automated methods for counting cells are not suitable for CSF because the low numbers of cells in CSF in comparison with blood result in erroneous counts. Morphologic examination of cells from CSF is most suitable on cytospin preparations in an appropriately equipped laboratory.
Normal CSF from large animals contains fewer than six white blood cells (WBCs) per deciliter; however, WBC counts greater than 40 cells/dL have occasionally been documented in the CSF of normal■ TABLE 35.1
Normal Range of Values in Cerebrospinal Fluid for Large Animals1,4,5
| Component | Unit | Equine | Bovine | Ovine | Caprine |
| Specific gravity | 1.004-1.008 | 1.004-1.008 | NA | NA | NA |
| Refractive index | 1.3343-1.3349 | 1.3343-1.3349 | NA | NA | NA |
| Protein | mg/dL | 5-100 | 20-40 | 8-70 | 24-40 |
| White blood cells (WBCs) | WBCs/dL | 0-6 | 0-3 | 0-5 | 0-7 |
| Glucose | mg/dL | 30-70 | 35-70 | 48-109 | 45-87 |
| Sodium | mEq/L | 140-150a | 132-144a | 145-157a | NA |
| Potassium | mEq/L | 2.5-3.5 | 2.7-3.2 | 3-3.3 | 3 |
| Creatine kinase | IU/L | 0-8 | 2-48 | NA | NA |
| Magnesium | mEq/L | NA | 1.7-2.7 | NA | NA |
aCerebrospinal fluid (CSF) sodium level is the same as serum or plasma sodium level when measured with ion-specific electrodes. When other measurements are used, the level of sodium in CSF is usually higher than that in plasma.
NA, Result not available.
horses.19 Although various “correction factors” have been suggested to correct for the effects of iatrogenic blood contamination, they are inaccurate and should not be used.18,20
The refractive index of normal CSF is less than 1.335. The protein concentration of CSF is less than 50 mg/dL in normal adult ruminants and less than 100 mg/dL in normal horses, although reference values vary with the techniques used for protein measurement. Reference values should be established for each laboratory.21
Studies of the specific and relative quantities of albumin and immunoglobulins, particularly immunoglobulins G and M (IgG and IgM), have been stimulated by the increasing importance of immunologic testing of CSF for diseases such as equine protozoal encephalomyelitis. Reference values for a number of parameters have been established.22 The most important of these parameters are albumin quotient, a measure of blood-brain barrier permeability,23 and IgG index, a measure of intrathecal production of IgG.24 The formulae for these parameters are as follows:
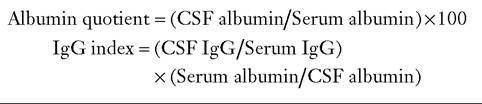
Reference values must be established for each species. An elevated albumin quotient indicates blood-brain barrier leakage or contamination of CSF with blood, with possible introduction of immunoglobulins from serum. An elevated IgG index indicates intrathecal production of IgG and may support a diagnosis of infectious disease of the CNS. The usefulness of these parameters is influenced by a number of other variables, including the immunoreactivity of blood.24 Therefore clinical interpretations must be made with great caution. The composition of protein from the CSF of horses and cattle has been established.3-5,10
The concentrations of glucose and protein in the CSF of newborn foals are almost twice those found in the CSF of adults, but they approximate adult normal values by the age of 2 weeks.25 In contrast, calves between 1 and 2 months have lower protein concentration and higher leukocyte numbers in CSF than do adult cattle.26
Neural tissue contains the BB isoenzyme of creatine kinase (CK-BB), which increases after damage to the nerve cells.27-29 The molecule does not cross the blood-brain barrier, and so CK in the CSF originates from neural tissue. Contamination of CSF with dura or fat, however, falsely elevates the CK concentration. Some have suggested that CK is an accurate marker and a prognostic indicator of CNS disease, but other studies have not supported this conclusion, and measurement of CK, although interesting, has limited clinical utility.27,29,30
The normal concentration of glucose in CSF is approximately 80% of that in blood. A decline in the ratio of CSF to serum glucose occurs in animals with bacterial meningitis because of increased use of glucose by inflammatory cells.
Measuring sodium concentration of the CSF may be helpful for diagnosing salt poisoning in cattle. In animals that do not have salt poisoning, the sodium concentration is less than 160 mmol/L; in animals with salt poisoning, the concentration is usually greater than 160 mmol/L.