Cobalt Deficiency in Ruminants
Robert Bascom Sager • John Maas
Definition and Etiology
A number of syndromes occur in ruminants as a result of a primary cobalt (Co) deficiency in their diet. These include ill thrift or enzootic marasmus and anemia.
These conditions are characterized by decreased growth, weight loss, diarrhea, decreased feed efficiency, unthrifty appearance, anorexia, and anemia. A Co deficiency syndrome referred to as ovine white liver disease has been described in sheep.1-3 This syndrome is also characterized by ill thrift, weight loss, serous ocular discharge, and occasionally photosensitization.1-3 Histopathologic lesions of this syndrome included accumulation of lipid droplets and lipofuchsin particles, dissociation and necrosis of hepatocytes, and sparse infiltration by neutrophils, macrophages, and lymphocytes.4 Co-deficient animals are more prone to parasitic infestation, particularly Ostertagia ostertagi in cattle.1 Also, Co fed at levels above National Research Council (NRC) minimal recommendations has resulted in increased antibody production to a single antigen in weaned beef calves.5Clinical Signs and Differential Diagnosis
Co deficiency in ruminants is associated with the nonspecific signs of decreased growth, weight loss, diarrhea, ill thrift, pica, emaciation, pale mucous membranes (anemia), and lacrimation. Clinical disease is more common in young, growing animals. Sheep are apparently more susceptible to Co deficiency than cattle. Primary differential diagnoses include helminthic parasitism; protein-calorie malnutrition; coccidiosis; Johne’s disease; nutritional deficiencies of selenium, copper, or vitamin D; and other chronic diseases that may be associated with weight loss. Co-deficient ruminants are commonly anorexic and fail to thrive on lush pasture or high-quality feeds.
Anemia with Co deficiency is characterized as normocytic normochromic and must be differentiated from other causes of anemia. Co-deficient cattle are more susceptible to infestation with Ostertagia ostertagi 4and to the effects of parasitism.4 1 he primary differential diagnosis when considering Co deficiency is invariably internal parasitism.
Clinical Pathology and Diagnosis
Because the role of Co in ruminant nutrition is tied to the formation, absorption, and use of vitamin B12, the most significant biochemical role of Co is correlated with tissue vitamin B12 concentrations. However, the effects of starvation tend to increase vitamin B12 concentrations in the liver and kidneys.6 If Co deficiency occurs with other conditions that cause anorexia, the tissue vitamin B12 concentrations may appear falsely elevated (normal). The appropriate analytic methods for serum B12 vary from humans to ruminants, so extrapolation of ruminant serum B12 concentrations analyzed in a human laboratory may not be possible. Serum or plasma vitamin B12 levels exhibit a marked diurnal variation.7 In addition, serum vitamin B12 concentration more closely reflects short-term Co intake and can be decreased when adequate liver reserves of vitamin B12 remain. In normal, Co-sufficient ruminants’ serum vitamin B12 values are usually 0.1 to 0.3 ng/mL (parts per billion [ppb]). When serum vitamin B12 values decrease, clinical signs of Co deficiency can become evident.8,9 Because serum B12 values can give spurious results, the concentration of Co in hepatic tissue is probably the best current standard for determining Co status and making clinical decisions. The liver concentration of B12 for cattle and sheep considered to be adequate is 0.30 to 2.24 μg∕mL (ppm) on a wet weight basis.10,11 Table 32.25 contains reference ranges for cattle and sheep.
■ TABLE 32.25
Reference Values for Cobalt and Vitamin B12
| Analyte | Cattle | Sheep |
| Serum cobalt | 0.1-0.3 ng/mL (ppb)11,12 | 0.1-0.3 ng/mL (ppb)11,12 |
| 1-3 ng/mL | 1-3.5 ng/mL | |
| vitamin B12 | (ppb)10,11 | (ppb)11 |
| Liver cobalt | 80-160 ng/g (ppb) wet weight10-12 | 80-160 ng/g (ppb) wet weight10-12 |
| Liver vitamin | 0.3-2.24 μg∕g | 0.3-2.24 μg^ |
| B12 | (ppm) wet weight10,11 | (ppm) wet weight10,11 |
Pathophysiology
Co deficiency in ruminants induces a deficiency of vitamin B12 (cyanocobalamin). It is the lack of vitamin B12 that is thought to cause the majority of clinical signs and clinicopathologic abnormalities observed. Monogastric species need to ingest vitamin B12 preformed, whereas ruminants can manufacture adequate vitamin B12 if the rumen microorganisms are supplied with adequate Co in the diet. The rumen microorganisms incorporate Co into vitamin B12 and a number of physiologically inactive vitamin B12-like compounds. The production of vitamin B12 from dietary Co was estimated to be approximately 15% in Co-deficient sheep and only approximately 3% in Cosufficient sheep.13 Approximately 50% of the vitamin B12 produced is absorbed in normal animals, but only 3% to 5% of vitamin B12 is estimated to be absorbed by Co-deficient sheep.14 Although the absorption of vitamin B12 formed in the rumen is not particularly efficient, with normal dietary Co there are usually no clinical problems, and interference by other dietary components does not appear to be clinically important.
Ruminants use the VFAs acetate, propionate, and butyrate as their primary energy sources. Propionate produced in the rumen is the precursor of glucose for ruminant metabolism. The general metabolic steps for conversion of propionate to glucose are shown15 in Fig. 32.144 use 32-134 from the 5th edition.
A primary defect in Co-deficient ruminants is the inefficient metabolism of propionate at the point in the pathway at which methylmalonyl-CoA mutase, a vitamin B12-requiring enzyme, catalyzes the conversion of methylmalonyl-CoA to succinyl- CoA.16 As Co deficiency becomes severe, the rate of propionate clearance from the blood decreases, and the intermediate metabolite methylmalonyl-CoA accumulates. 17 With severe Co deficiency, the amount of methylmalonic acid excreted in the urine increases. As the half-time for propionate clearance increases, the voluntary feed intake of Co-deficient sheep decreases.17 These changes correlate with the degree of anorexia and weight loss observed in severely Co-deficient sheep.
The decreased growth, weight loss, unthrifty appearance, and anorexia are closely correlated to the observed abnormalities of carbohydrate metabolism. The diarrhea commonly observed with Co deficiency is not well explained; however, an increase in susceptibility to parasitism4 might explain a portion of this clinical observation.
The anemia that is associated with Co deficiency occurs late in the development of the syndrome and is characterized as normocytic normochromic.18 Co deficiency results in the depression of the vitamin B12-containing enzyme 5-methyltetrahydrofolate homocysteine methyltransferase.19 This interference with the recycling of methionine has a marked influence on folate metabolism. In addition to potentially
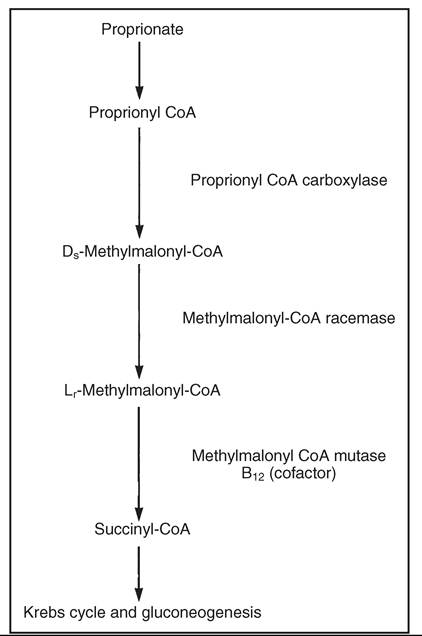
FIG. 32.144 Pathway for conversion of proprionyl coenzyme A (CoA) from proprionate to succinyl CoA.
resulting in anemia through inefficient folate metabolism, the decreased activity of this methyltransferase could lead to a deficiency of methionine; this is a possible reason for nitrogen retention and the decreased body growth and wool growth observed.
■ Epidemiology and Cobalt Requirements Co deficiency in ruminants occurs in selected regions throughout the world and in association with a variety of soil types. Clinically recognizable Co deficiency is reported in New Zealand, Australia, Brazil, United Kingdom, Ireland, Scandinavia, and North America. In the United States, Co deficiency is most commonly seen in Florida, in the Northeast, along the eastern seaboard, in the upper Midwest, and around the Great Lakes.20 Although various soil types are associated with Co deficiency, heavy fertilization with limestone reduces the Co available to plants and animals.21 The dietary requirement of Co by ruminants is generally recommended to be 0.1 mg/kg of dry matter (DM) of the complete ration.22-24 The Co requirement of young, rapidly growing lambs is thought to be 0.2 mg/kg (ppm) of DM of the diet.25 When pasture Co concentrations are less than 0.07 mg/kg of DM or 0.04 mg/kg of DM for sheep and cattle, respectively, signs of deficiency can be expected to develop. On a practical basis, diets with 0.1 mg/kg of DM are considered to be adequate. Legumes have relatively high Co concentrations. Rapidly growing grasses have much lower Co concentrations, and cereal grains are poor sources of Co.22 Oilseed meals are generally good sources of Co. Co supplemented at levels above NRC recommendations (0.2 mg/kg versus 0.1 mg/kg) has been associated with increases in the immune response to one antigen in cattle.5
■ Treatment and Control Treatment is best accomplished in the short term with vitamin B12 injections. Ruminants poorly absorb oral vitamin B12; thus injections are the most efficient.
Lambs receiving 100 μg of vitamin B12 per week or 150 μg B12 every other week show remission of clinical signs.26 Sheep receiving injections of 300 μg of vitamin B12 weekly or cattle receiving 2000 to 3000 μg of vitamin B12 weekly would also be expected to regain normal status.Rations with 0.1 to 0.2 mg/kg (ppm) of DM Co would be expected to prevent Co deficiency in ruminants. Salt-mineral mixes containing 0.1% Co also provide adequate supplementation. 0.1% Co in salt can be made by mixing Co carbonate (which is 46% Co) at the rate of 4.35 pounds/ton of salt, or 1 g of Co carbonate per pound of salt. A pound equals 453.59 grams.
Co sulfate as a top dressing for pastures (1.5 kg/hectare every 3 to 4 years or 0.3 kg/hectare every 1 to 2 years) has been used to increase Co concentration of pasture forage. Heavily limed pastures21 and soils high in manganese oxide27 decrease Co availability, and Co top dressing of the pastures or Co (B12) supplementation to the animals should be considered.
A variety of rumen pellets containing Co are used to supplement grazing ruminants. These pellets have been successful in maintaining normal Co status in animals.25-29 The pellets are not commercially available in the United States at this time.
The perennial grass, Phalaris tuberosa, can cause a syndrome in ruminants that is referred to as “phalaris staggers.” Co supplementation can aid in prevention of this syndrome because it inactivates or decreases absorption of the neurotoxin contained in P. tuberosa, Phalaris minor (canary grass), or Phalaris hybrids (ronpha).29 The increased level of Co in the rumen is the important factor in preventing this condition; administration of oral or parenteral vitamin B12 is not effective.26 Treatment of clinical phalaris staggers with Co is not effective, however.
Because Co is poorly absorbed, toxicity is an uncommon problem, and diets in excess of 30 mg/kg of DM are necessary for toxicosis to occur in most cases.22-24
A recommendation by the National Research Council of increased levels for Co (mg/kg DM) for beef cattle has been made since 2016. This increase has recommended increased Co levels of 20 mg / kg DM from the previous 10 mg/ kg DM. Research has reflected increased NRC Co levels improved performance (ADG) in Simmental bulls (Stangl, et al.). Increased NRC Co levels in feedlot steers showed increased antibody titers of M. haemolytica leukotoxin (P postsurgical complications.