Dentistry and Oral Disease
Jack Easley
The equine species has evolved as a continuously grazing animal, developing its own dental form and function over millions of years. The oral and dental structures provide horses with the ability to detect, prehend, masticate, and begin the digestion of mixed grass forage.
As humans have domesticated and confined horses, their diet has been altered to consist of grazing improved pastures with more interval feedings of dry hay, grain, processed forages, and concentrates. Selective breeding and domestication practices have increased the incidence of equine dental and oral disease in modern equine populations.■ Anatomy and Function The structures that horses use in eating include tactile and prehensile lips, hypsodont incisors, premolars and molars, facial bones, muscles of mastication, tongue, hard palate, buccal mucosa, cheeks, olfactory organs, taste buds, salivary glands and ducts, blood vessels, lymphatic vessels, and nerves that support them. The equid oral cavity is long and cylindrical and is the entrance to the alimentary canal. The muscular lips form the entrance to the mouth, which is bound laterally by the cheeks, dorsally by the palate, and ventrally by the body of the mandible and the mylohyoid muscles. The caudal aspect of the mouth is composed of the soft palate, root of the tongue, and epiglottis and is continuous with the oropharynx.1,2
The blood supply to the mouth is derived from the maxillary, mandibular, labial, and sphenopalatine arteries. The venous drainage is chiefly through the linguofacial veins. Nerve sensation in the mouth, cheeks, and lateral aspect of the tongue is derived from the mandibular and maxillary branches of the trigeminal nerve (cranial nerve V). Motor function of the sublingual and mandibular salivary glands, lacrimal glands, and facial and labial muscles is activated by the facial nerve (cranial nerve VII).
The hard palate has a central raphe, dividing the surfaces into right and left halves. The portion of the palatal mucosa just caudal to the upper incisors may appear swollen in 2- to 5-year-old horses when permanent incisor teeth erupt. Such mucosal enlargement is normal and has historically been referred to as lampas. Farther caudal, the hard palate becomes more concave and contains paired transverse ridges that traverse the cavity. These ridges are instrumental in moving a food bolus caudally in a spiral manner as horses masticate forage.The highly mobile, muscular tongue sits in the bottom of the mouth between the paired hemimandibular rami. It is covered by a tough, specialized squamous epithelium modified to form papillae. The tongue is supported in a sling formed by the mylohyoideus muscles. The root of the tongue is attached to the lateral aspect of the soft palate, pharynx, and hyoid bone. The lingual muscles receive their motor innervation from the hypoglossal nerve (cranial nerve XII) and sensory innervation from the lingual and glossopharyngeal nerves (cranial nerve IX). The rostral portion of the tongue is susceptible to injury from bits and other tack placed in the oral cavity. Injury from penetrating foreign body (usually wire) and neurogenic injury are possible.
The mandible is the largest bone of the face and is formed by the paired hemimandibles, which fuse rostrally at the mandibular symphysis when horses are approximately 2 to 3 months of age. Each hemimandible is composed of a horizontal and a vertical ramus. The horizontal ramus contains the alveoli of the teeth in the lower jaw. The vertical ramus terminates with the coronoid process rostrally and the mandibular condyle caudally. The temporalis muscle inserts on the coronoid process.
Between the incisors and the rostral aspect of the mandibular cheek teeth in the horizontal rami of the mandible is a large diastema: the interdental space or “bars” of the mouth. Canine teeth, if present, are located in this area.
In young horses, the ventral border of the mandible is wide and round. Eruption swellings or “bumps” are often seen on the ventral border of the mandible of 2- to 4-year-old horses as the permanent mandibular cheek teeth erupt. With age and as eruption of the mandibular cheek teeth continues, the ventral border of the mandible takes on a sharper, angled appearance.The paired incisive (premaxillary) bones form the rostral part of the upper jaw and contain the alveoli of the upper incisors. Caudally, the incisive bone becomes thinner and forms the rostral part of the hard palate. The suture line between the incisive bones and the maxillary bones is an anatomically weak area and a common site of facial fractures. The upper canines (if present) are situated just caudal to this suture line.
The paired, large maxillary bones extend from the incisive bone rostrally to the nasal bones dorsally and lacrimal bones caudally. The facial crest is a prominent ridge of bone on the lateral aspects of the maxillae. This crest continues caudally as the zygomatic process and joins the molar and temporal bones to form the zygomatic arch. The ventromedial aspects of the maxillary bones join to form a horizontal shelf that provides rigid support to the majority of the hard palate. The alveoli of the upper canines, premolars, and molars are embedded in the maxillae. The positions of the alveoli of the upper cheek teeth are somewhat variable, but usually the alveoli of the first two cheek teeth lie rostral to the maxillary sinuses. The third and fourth cheek teeth lie within the rostral maxillary sinus in young and middle-aged horses. The caudal two cheek teeth lie within the caudal maxillary sinus. As the teeth continue to erupt with age, the maxillary sinus volume increases. More detailed anatomic relationships of the maxillary cheek teeth and the paranasal sinuses have been explored in horses of various ages with the use of CT.3 Each alveolus is separated by transverse interalveolar bony septa.
Horses have seven paired paranasal sinuses: ventral conchal, dorsal conchal, frontal, sphenopalatine, caudal maxillary, rostral maxillary, and ethmoidal sinuses. The rostral and caudal maxillary sinuses are contained within the maxillae and are usually separated by a thin bony septum, although this septum often breaks down with sinus disease. The long infraorbital canals (one on each side of the head) traverse longitudinally through the maxillary sinuses, encasing the large paired infraorbital nerves.
Sinusitis can result from disease of the third, fourth, fifth, and sixth upper cheek teeth and classically results in a unilateral, malodorous nasal discharge. In a young horse, virtually the entire maxillary sinuses are occupied by dental alveoli. Therefore as the facial bones grow and reserve crowns of the upper cheek teeth erupt, the cheek teeth move forward and ventral in the sinus compartments. The maxillary sinuses drain into the back of the nasal cavity via a slitlike aperture, the nasomaxillary opening. The medial compartment of the rostral maxillary sinus is called the ventral conchal sinus. This compartment has poor drainage and is a common site in which inspissated pus accumulates. Its secretions must drain dorsally over the infraorbital canal into the lateral compartment of the rostral maxillary sinus. Drainage from these two sinuses courses into the caudal middle meatus adjacent to the drainage angle of the caudal maxillary sinus. The areas rostral to the paranasal sinuses are scrolled sections of the nasal cavities, referred to as the dorsal and ventral nasal conchal bullae. These structures have been shown to be an area in which inspissated pus accumulates in cases of chronic sinusitis.4
The temporomandibular joint is a synovial joint formed by the articulation of the squamous temporal bone and the condylar process of the mandible. The joint lies approximately 15 cm above the level of the occlusal surface of the cheek teeth. The joint cavity is large and divided in two by a cartilaginous intraarticular disk.
The joint is bound by a tight capsule and lateral and caudal ligaments. The unique functional anatomy and age-related changes in the normal equine temporomandibular joint were described only as recently as the mid-2010s.5,6 This joint can make a wide range of lateromedial movements (allowing the medially directed power stroke of mastication) but limited vertical and rostrocaudal movements.7As a result of the wide lateromedial range of motion of the temporomandibular joint associated with the power stroke of chewing, the masseter and pterygoid muscles are the most highly developed muscles of mastication in horses. The powerful masseter muscle originates along the full length of the facial crest and zygomatic arch and has wide insertions along the caudolateral aspect of the mandible. The superficial masseter muscle fibers run almost vertically, whereas the deep fibers course in a ventrocaudal direction. The masseter pulls the jaw to the ipsilateral side and also contributes to closure of the jaw. The medial and lateral pterygoid muscles have origins and insertions similar to those of the masseter, and these lie on the medial aspect of the mandible. The digastricus muscle originates on the occipital bone and attaches to the caudal aspect of the mandible and is small in horses as a result of the minimal effort required to open the jaw with gravity assistance. The temporalis muscle, whose function is jaw closure, is also small and poorly developed in horses because vertical opening of the temporomandibular joint is limited. The muscles of mastication are innervated by the motor branch of the mandibular nerve, which originates from the trigeminal nerve (cranial nerve V).
■ Teeth At approximately 6 months of age, 24 deciduous teeth have erupted in a foal. Development of the cranial and facial bones during the first 2 to 3 years of life allows room for the expansion of the dental formula from 24 deciduous to between 36 and 44 permanent teeth in a mature horse.
The mature mouth of a horse contains six incisors each in both the upper and lower jaws, six permanent upper cheek teeth on each side of the mouth, and six lower cheek teeth on each side of the mouth (Fig. 32.40). The rostral three cheek teeth are premolars, and the caudal three cheek teeth are molars. Incisors and premolars have deciduous and permanent sets. Molars erupt at an older age and do not have deciduous counterparts. The cheek teeth of the upper jaw are broad and square, whereas the lower cheek teeth are narrower and rectangular.The cheek teeth in each quadrant of a horse's mouth are commonly referred to by number, from rostral to caudal (1 to 6). The inconsistent and vestigial first premolar, often referred to as a “wolf tooth,” is not included in the 1-to-6 nomenclature. To help avoid confusion, the American Veterinary Dental College has endorsed use of the Modified Triadan System of tooth numbering for horses.8 This three-digit tooth numbering system is based on a full phenotypic dentition composed of 44 teeth in total. The first digit designates the quadrant and arcade location and whether the dentition is deciduous or
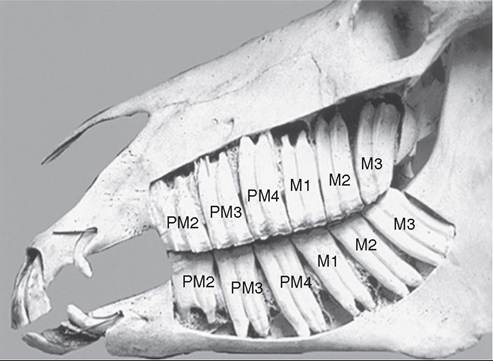
FIG. 32.40 Lateral view of equine cadaver skull. M, Molar; PM, premolar.
permanent. The numbering sequence for permanent teeth starts with 1 for the upper right, 2 for the upper left, 3 for the lower left, and 4 for the lower right. The corresponding deciduous teeth quadrants are numbered 5 to 8, respectively. In each dental quadrant, the first or central incisor is always 01; the other incisors are numbered 02 and 03. The canines, whether present or not, are designated 04 in this formula. The premolars are numbered 05 to 08 and the molars 09 to 11.
The equine incisor and molarized cheek teeth are hypsodont and have long anatomic crowns, which erupt throughout the life of the animal in a dynamic process of periodontal ligament and alveolar bond remodeling. The tooth crown is the enamelcontaining portion of the tooth. When these hypsodont teeth first erupt, the occlusal surface is covered with cementum overlying the enamel. As the teeth are subjected to masticatory forces and abrasive forage, the thin layers of occlusal cementum and enamel wear away, exposing the true or functional occlusal surface of the tooth. This process is termed coming into wear. The functional occlusal surface of hypsodont teeth is composed of thin, brittle sheets of hard enamel, sandwiched between softer but more stress-resistant layers of cementum and dentin. This three-textured occlusal surface is self-sharpening and very wear- and fracture-resistant. At the time of eruption, there are no true roots, and teeth are divided into apical and coronal regions, but most of the crown (reserve crown) lies within the alveolus. True roots are formed gradually over a period of 2 to 3 years after eruption.
The incisors and upper cheek teeth have enamel crown invaginations termed infundibulae. These invaginations partially fill with cementum that receives its blood supply from the occlusal soft tissues covering the tooth before eruption. A shallow infundibulum is present on each incisor tooth and has a wide opening at the occlusal surface referred to as a cup. As a tooth wears down over time, the small bottom portion of the infundibulum is exposed at the occlusal surface and is called the spot. Each upper cheek tooth has two deeper infundibulae: one rostral (mesial) and one caudal (distal). These extra enamel cones give the central area of these teeth a hard, serrated, but wear-resistant chewing surface. As these teeth develop but before the occlusal surface comes into wear, the infundibulae are supplied by infundibular arteries entering from the occlusal direction. Cementogenesis of the infundibulum starts first at distinct enamel infoldings in the occlusal part of the infundibula and advances in an apical direction.9 The center of the cement lake that fills the infundibulum contains a hole of variable diameter. This channel is a remnant (“ghost”) of the central blood vessel that supplied nutrition to the now dead infundibular cementum. If the blood supply becomes compromised before cementogenesis is complete, infundibular cemental hypoplasia can develop, which predisposes affected teeth to infundibular caries and midsagittal fractures.
The interior of a tooth is composed primarily of dentine; primary dentine lines the walls of the common pulp chamber of a newly erupted tooth. The pulp chambers of hypsodont teeth are active throughout a horse's life, with primary and secondary dentine continually produced within the pulp cavity. This process of continuous secondary dentine production prevents pulp exposure at the occlusal surface as the tooth wears. The depth of secondary dentine at the occlusal surface of the pulp horns (seen as a brownish area on the occlusal surface of the tooth) varies in horses but is usually 5 to 7 mm thick. No age-related increased thickness of occlusal secondary dentine has been found research, which supports the theory that secondary dentine deposition is at least partially regulated by occlusal stimulation.10,11 The pulp cavity in the young equine permanent cheek tooth is very large. With increasing age, it divides into smaller pulp chambers (or horns) as dentine deposition increases. From 2 to 4 years after eruption, mandibular cheek teeth have a distinct, apically located, common pulp chamber that communicates with the pulp horns. The number of pulp horns has been well described: Five pulp horns are present in the 07 to 10 teeth, six pulp horns in the 06 teeth, and six or seven pulp horns typically present in the 11 teeth (Fig. 32.41).12 Two to four years after tooth eruption, the dentine divides the endodontic system of most of the mandibular cheek teeth into two distinct compartments or roots. Each compartment consists of a root canal, a pulp chamber, and two or three pulp horns. The anatomic changes in pulps with age are quite complicated and slightly different between horses; thus endodontic treatments in this species are challenging.13 The maxillary cheek teeth, as well as the 311 and 411, have three roots: one palatal and two buccal. Because of the continuous production of cementum around the apical or root portion of the tooth and continuous crown wear, old equine teeth wear apically past the infundibular enamel and peripheral enamel infolding that normally prevents crown
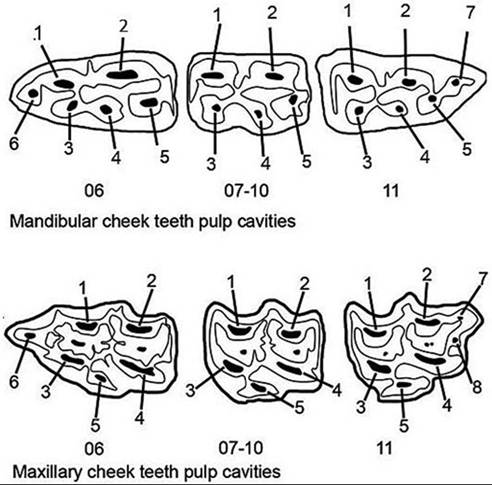
FIG. 32.41 Diagram of the premolar and molar pulp horns, seen as dark areas of secondary dentine on the occlusal surface.
attrition (senile excavation). When most of the crown enamel has worn away, the softer dentine and cementum are quickly worn away, which leads to a condition known as “senile excavation.” As the crown undergoes further wear, the peripheral enamel is lost, and the smooth dentine and cementum become the functional occlusal surface. When this condition involves multiple teeth in an arcade, it is referred to as smooth mouth.
Innervation of the dental structures is supplied by the trigeminal nerve (cranial nerve V), which exits the skull just below the ear. This nerve traverses rostrally and divides into the ophthalmic, maxillary, and mandibular branches. The maxillary nerve lies in the pterygopalatine fossa deep to the subperiorbital fat pad and enters the caudal maxilla ventral to the orbit via the maxillary foramen. It runs through the maxilla in the infraorbital canal, at which point it becomes the intraorbital nerve, and gives off branches to supply the maxillary cheek teeth and incisors. A branch of the infraorbital nerve exits the maxilla at the infraorbital foramen, just rostral and dorsal to the facial crest. The mandibular nerve runs medially along the mandible, becoming the lingual and inferior alveolar nerves, which arise as a common trunk and pass rostrally between the pterygoideus medialis and the ramus of the mandible. The inferior alveolar nerve enters the mandibular canal on the caudomedial aspect of the mandible, innervating the mandibular teeth. The mental nerve exits the mandibular canal via the mental foramen at the rostrolateral aspect of the mandible just rostral to the mandibular cheek teeth and supplies the ipsilateral soft tissues over the incisive portion of the mandible. These nerves and their branches are clinically significant in diagnostic procedures or procedures involving regional anesthesia in horses.14
Rudimentary first premolars (wolf teeth) are constant in fetal life in both upper and lower jaws. Many never develop to the point of eruption but instead degenerate and become incorporated in the maxilla or mandible. The upper wolf teeth erupt in 20 to 80% of horses; the lower wolf teeth rarely erupt (in 1% to 5%).
Equine males normally have two upper and two lower canine (bridle) teeth. This type of anatomic discrepancy is referred to as sexual dimorphism, inasmuch as as canine teeth are absent or rudimentary in most mares. The upper canine teeth erupt just caudal to the suture between the incisive and maxillary bones. The lower canine teeth lean forward, producing a long lower diastema or interdental space.
The horse is anisognathic: that is, the bottom jaw is narrower (by ≈25%) than the upper jaw. The lateral excursion of the jaw during mastication is conducive to occlusal wear of the buccal aspect of the lower and the lingual aspects of the upper molar arcades. The horse's jaw anatomy and jaw motion have an effect on the angle of the molar tables.15 Cheek teeth occlusal angles have been found to range from 15 to 20 degrees in normal horses, according to three-dimensional models from CT images.16 As horses chew, the jaw moves in rotational motion from side to side with some rostral-caudal excursion.17 The construction of the molars with interdigitations of enamel, cementum, and dentine allows for uneven, continuous wear with a sharp, serrated surface when horses are grazing. The extent of lateral excursion of the mandible during normal mastication is affected by the length of the stem or roughage in a horse's ration. A horse on pasture or hay has a full or wide area of mandibular excursion. However, horses eating pellets or concentrates have a limited range of lateral jaw excursion. Horses with limited lateral jaw excursion have incomplete wear of the molar surfaces, which predisposes the arcades to sharp enamel edges, a vaulted ceiling of occlusion, or the serious problem of shear mouth. Malocclusion of the incisor or molar arcades perpetuates abnormal wear patterns that eventually predispose affected horses to diastema and secondary periodontal disease.18
Rostral or caudal molar malocclusions or eruption problems (displaced, deformed, delayed-eruption, missing, or supernumerary teeth) lead to uneven dental wear. Many horses with asymmetry between the upper and lower molar arcades (as a result of mandibular fracture, facial injury, congenital deformities such as brachygnathism [parrot mouth] and prognathism [sow mouth] or a mandible that is abnormally narrow in relation to the maxilla) have abnormal tooth wear in the form of sharp enamel points, dental overgrowths (hooks or ramps), shear mouth, step mouth, or wave mouth.
The dynamic change that takes place in the mature horse's head continues at a slower rate throughout life, with continual eruption and crown wear of the hypsodont premolar, molar, and incisor teeth, which retain their long reserve crowns and slowly-forming, short root structures. With continuous eruption and wear of the equine hypsodont teeth, all horses eventually experience senile attrition and wearing of their teeth “smooth” to the root.
■ Equine Dental Developmental Abnormalities Equine dental developmental abnormalities can involve tooth number, structure, or position in the dental arcades. Abnormalities of dental development and eruption are quite common in horses and result in a wide range of clinical conditions. A congenital/developmental problem that manifests at the time of tooth eruption often leads to acquired dental problems as the teeth continue to erupt and wear. Some developmental abnormalities of the teeth of very young horses may not cause it to exhibit clinical signs until middle age. Consequently, several different dental abnormalities with interrelated pathogenesis are often present concomitantly at the time of clinical 19 21
presentation.19 21
SUPERNUMERARY TEETH. Supernumerary teeth are teeth in excess of the normal expected number in any of the dental arcades. This disorder has been referred to as polydontia or hyperdentition. Supernumerary teeth can be loosely categorized morphologically into two categories: (1) supplemental teeth that resemble teeth of the normal series in crown and root structure but not always in size, and (2) rudimentary or dysmorphic teeth that are abnormally shaped and smaller in size than normal teeth.
In general, these extra teeth are encountered at the caudal aspects of the molar arcades, but supernumerary teeth can also be lingual, buccal, or rostral to the normal arcades. Clinical signs most commonly associated with supernumerary cheek teeth are dental overgrowths and diastemata, which often lead to secondary periodontal disease.
Supernumerary incisors are reported more often in horses than are supernumerary cheek teeth. The main condition included in the differential diagnosis for supernumerary incisors or cheek teeth is retained deciduous teeth. In some cases, it may be clinically difficult to determine whether an extra tooth is a retained deciduous tooth or a supernumerary tooth. Examination with a radiograph that encompasses the entire affected dental arcade is often necessary to diagnose this condition. Radiographic examination of the affected jaw is often indicated to determine the identity of an extra tooth. A retained deciduous tooth has a more mature root and a shorter reserve crown than does the adjacent permanent teeth. Such distinguishing characteristics are visualized with radiographs.
Horses with supernumerary teeth should be managed on a case-by-case basis, but management in general is limited to regular assessment of the dentition, coupled with aggressive dental floating to minimize the opportunity for soft tissue damage by unopposed elongations. Dental elongations place abnormal orthodontic forces on the involved tooth. This can lead to shifting of teeth and diastema formation. In severe long-standing cases, deep periodontal pockets and oroantral fistulas predisposing to forage accumulation in the paranasal sinuses may develop. If complications such as severe periodontal disease or maxillary sinusitis occur, the supernumerary tooth or displaced adjacent tooth should be extracted or appropriate therapy undertaken to manage associated pathology, or both.18-22
OLIGODONTIA. Oligodontia is the congenital absence of a tooth germ or retention and inclusion of a tooth within the jaw. It is difficult to differentiate developmental oligodontia from tooth loss caused by damage to, or displacement of, a dental bud from injury. It is possible for permanent tooth germs of a young horse to be damaged, displaced, or removed when deciduous teeth or jaw bones are injured. Absence of a tooth in the dental arcade leads to dental drift or tipping of adjacent teeth. Lack of wear in the antagonist to the missing tooth can lead to dental elongations and abnormal mastication. Radiographic examination is often necessary to confirm a diagnosis of true oligodontia. Oligodontia may be associated with other epidermal defects such as poor development of hair and hooves.23
DENTAL DYSPLASIA OR HYPOPLASIA. Dental dysplasia (i.e., abnormal growth or development of a tooth or teeth) may result in an irregularly shaped tooth that does not fit well into a dental row. The poor fit may lead to diastemata, food entrapment and periodontal disease. Enamel hypoplasia has been associated with certain drugs or chemicals administered to the dam during gestation, or it may be idiopathic in origin. Dental dysplasia can involve the abnormal formation of the entire tooth structure or only a single tissue type. Abnormal enamel structure, such as branched pulp horns or abnormally shaped teeth, has been observed. Enamel acts as the scaffolding and template for the deposition of dentine and cementum. These tissues follow the abnormal enamel pattern, and consequently all three calcified tissues are dysplastic. Cemental hypoplasia usually involves the infundibular portion of the tooth, but it can also be a defect of the peripheral, coronal, or reserve crown or root cement.
ABNORMAL DENTAL ERUPTION. Abnormal dental eruption, or maleruption, often results from trauma to developing teeth or surrounding bones, but it has also been reported to be congenital or idiopathic in origin. Cheek teeth can become vertically impacted when dental buds are developing in abnormal or crowded areas in the dental arcades. Teeth may become rotated or otherwise displaced as a result of developmental malpositioning of tooth buds or overcrowding before, during, or after eruption.
Most tooth displacements are developmental in origin as a result of overcrowding of the cheek tooth row at the time of eruption. These malocclusions are seen most often in miniature breeds and ponies and are often bilateral. Tooth displacements are also believed to be caused by abnormal positioning of a dental bud, which may result in impaction and delayed eruption or noneruption of the displaced teeth if they are sufficiently horizontal to the adjacent teeth. Developmental diastemata or abnormal spaces or gaps between cheek teeth are often caused by insufficient angulation of teeth to achieve interdental compression between adjacent teeth. Another cause for diastemata is the development of embryonic teeth too far apart.21
Malocclusions of incisors are congenital, developmental, or acquired in origin. Mandibular brachygnathism (parrot mouth) is a congenital incisor malocclusion, the origin of which is unknown but probably genetic. Many horses have some degree of overjet of the premaxillary incisors, but the overjet rarely causes a problem with prehension, unless the premaxillary and mandibular incisors totally lack occlusion. If brachygnathism is discovered when the foal is young, treatment may correct, or at least improve, the functional outcome for the animal.24
A main consideration with an incisor overjet in adult horses is the cheek teeth malocclusions that accompany this condition. The maxillary cheek teeth arcades are usually positioned rostral to the mandibular cheek teeth, causing a rostral overgrowth of teeth 106 and 206 and a caudal overgrowth of 311 and 411. Check teeth elongations should be reduced to allow for proper rostrocaudal jaw excursion and mastication. The unopposed incisors can become elongated and limit lateral jaw motion, which can lead to abnormal dental wear and shear mouth.
Prognathism or undershot jaw occurs with less frequency in horses and is most common in miniature or dwarf breeds. Early detection and correction of the malocclusion in the foal may prevent the condition from worsening with age. The cheek teeth should be evaluated for malocclusion caused by overgrowths of teeth 111, 211, 306, and 406 and these should be corrected on a regular basis.
Bony malformations of the head can result in malocclusion of the incisors and cheek teeth. These bony skull curvatures or asymmetries usually result in an offset or diagonal incisor bite. Some bony malformations, such as campylorrhinus lateralis (wry nose) are obvious, and surgical correction may be necessary for a horse to be functional.25 More subtle changes to the large bony plates in the head can be difficult to recognize and can be managed by correcting dental overgrowths and abnormal wear patterns.26 Fractures secondary to trauma to the mandible or facial bones can also cause malocclusions and facial asymmetry. Care must be taken with correcting dental overgrowths associated with malocclusions, and they should be corrected gradually to prevent damage to pulp horns (which can lead to apical infection), dysphagia, and pain. Often, incisor malocclusion remains throughout a horse's lifetime, but regular maintenance may prevent it from worsening.
■ Acquired Dental Disease Dental disease can be grouped into six basic categories:
1. Dental malocclusions and abnormal occlusal wear
2. Periodontal disease
3. Caries of the infundibulum or peripheral cementum
4. Endodontic disease
5. Tooth resorption and hypercementosis
6. Traumatic dental injuries
These dental disease types are interrelated, and in most clinical cases, affected horses suffer from a combination of varying degrees of different dental disease types.
Alignment of the dental arcades is critical for the normal wear of continually erupting equine dentition, and any malocclusion can lead to abnormal occlusal wear. Historically, abnormal dental wear patterns have been described as dental crown elongations, descriptive terms for which include hooks, ramps, waves, steps, and transverse ridges. These elongations usually involve a normal tooth that is out of occlusion with an abnormality in the opposite arcade. The opposite diseased, damaged, misplaced, or missing tooth or jaw should be evaluated when elongations are found. Most dental elongations are addressed by reducing the crown height of the long tooth or portion of a tooth with a rasp or grinding instrument. In dental reductions, iatrogenic damage to the tooth, such as pulp horn exposure, thermal injury, or crown fracture, must be avoided. The viable pulp is usually covered by 7 to 10 mm of secondary dentine, but only 2 to 4 mm occlusal secondary dentine covers some pulp horns. Therefore crown reductions should be carried out in stages; no more than 3 to 4 mm of occlusal crown should be reduced in a session. Power grinding dental instruments generate heat that can cause damage to the pulp tissue. Shorter durations of grinding and water cooling have been found to mitigate this heating effect.27,28 It is important to diagnose and treat the underlying malocclusion or dental disorder in horses with a diagnosis of abnormal dental elongations; otherwise, the elongation of the tooth will recur over time as the tooth erupts.
Periodontal disease is an altered state of the periodontium. The periodontium is the attachment apparatus of the tooth consisting of the gingiva, alveolar bone, periodontal ligament, and cementum. The periodontium is responsible for hypsodontic tooth eruption and for the distribution of masticatory forces from the teeth into the supporting bone. Periodontal disease is often a painful dental condition and is described as the leading cause of “quidding” in horses. Gingivitis is the mildest form of periodontal disease and is often associated with local irritants such as plant awns or bristles, botfly larvae, traumatic injury, or chemical exposure. Oral ulceration can be a reflection of systemic disease, such as vesicular stomatitis, which is a contagious reportable disease. Another mild form of periodontal disease affects primarily young horses 2.5 to 5 years of age when deciduous teeth (caps) are shed and permanent incisors and premolar teeth are erupting. A more progressive form of periodontal disease affects older horses as a result of the chronic effects of diastema or spaces that develop between teeth that are not aligned properly in the arcade. Diastema can form during tooth development when dental buds are spaced too far apart or abnormally angulated so that the teeth in a dental row are not properly compressed, which allows forage to become trapped between teeth. This is usually a progressive condition; left untreated, it becomes worse over time. As food becomes compressed deep between teeth, gingivitis and gingival recession develop. Deeper penetration of food causes periodontal disease to progress to affect all four periodontal tissues, along with proliferation of secondary bacterial infection with multiple species of bacteria that are also found in the normal equine oral cavity. Current molecular bacteriologic techniques help practitioners and scientists better understand this large pool of organisms that cannot be conventionally cultured.29 Periodontal disease is the primary cause of tooth loss in mammals and is the most common reason for extraction of equine cheek teeth.
Management of periodontal disease involves treating both the cause and the effect of the problem. Diastema with feed trapped in the gingival margin often responds to thorough cleaning with dental picks, irrigation, or both. Reduction of any associated abnormal wear patterns is also indicated. In more refractory cases, it may be necessary to open or widen the diastema with a special burr or a right-angle grinder. This procedure may allow horses' masticatory actions to more easily channel food in and out of the gap, thus preventing or reducing entrapment of feed or stagnations and decay. This procedure is not without risk of pulp exposure and should be performed only by a professional with proper equipment and training.30
Some practitioners have had positive results using high- pressure irrigation to clean out periodontal pockets, followed by packing the area with a perioceutic agent such as doxycycline gel or a powdered antibiotic. This technique packs a high concentration of antibiotic in contact with the infected and inflamed tissues and acts as a temporary barrier to recontamination. This form of therapy may need to be repeated on a regular basis (every 4 to 6 months) in order to achieve long-term positive results. Severe periodontal disease that has resulted in bone loss and tooth mobility responds positively only to extraction of the involved teeth.
Dental caries is the macroscopic destruction of calcified dental tissues as a result of pH changes. These changes usually result when microorganisms within the oral cavity metabolize dietary carbohydrates to produce acids, which dissolve the mineral components of teeth. Because the mineral content of cementum (65% inorganic material) is lower than that of enamel (96 to 98% inorganic material), the critical pH required for the demineralization process is higher (less acidic) than that for enamel; a pH of 5.5 is required for enamel, 6.2 for dentine, and 6.7 for cementum. Caries in horses can affect the exposed crown or infundibulum of the hypsodont teeth, the softer cementum being more commonly involved. Peripheral caries involving the cementum around the erupted tooth crown is poorly understood. This condition usually involves the distal cheek teeth and can progress to involve all three dental tissues. The prevalence is higher in particular regions of the world, and feeding on hay high in water-soluble carbohydrates, feeding on silage with a low pH, and drinking water with a low pH were found to be contributing factors. Equine peripheral caries does appear to be a reversible condition if the etiological agent is removed.31
Caries can also involve the infundibular portion of the incisor and maxillary cheek teeth. All infundibulae of incisor and cheek teeth show some evidence of cemental decay in the cup or open portion.9,32 As the tooth wears, the portion of the infundibulum that is more apical fills with cementum (except for the small central vascular channel) and becomes exposed at the occlusal surface (referred to as the spot in the incisor teeth). Feed and other products of mastication can be compressed into a ghost of a vascular canal, and some degree of decay is always present. The infundibulum contains dead cementum and is lined with a layer of enamel. Therefore this decay does not usually lead to an inflammatory response or dental infection, and such superficial decay is innocuous in most cases. True dental disease secondary to infundibular decay can occur only if the protective enamel layer is penetrated. Developmental malformations of the infundibulum may weaken this enamel and predispose affected horses to dentine exposure and pulp disease. In upper cheek teeth with very large vascular channels or deformed infundibula, decay may weaken the tooth and predispose the tooth to excessive crown attrition or midsagittal crown fracture. A shallow infundibulum or senile attrition of the infundibulum can allow central occlusal excavation, which can lead to dental elongations on the opposite occlusal arcades (wave mouth). These abnormal wear patterns need to be reduced on a regular basis. To help strengthen the tooth and delay the progression of infundibular decay, some practitioners advocate cleaning out abnormally enlarged infundibular vascular channels and packing and sealing them with a dental composite material.33 As advanced diagnostic methods such as CT become more readily available to equine practitioners, these abnormal-appearing infundibula can be better evaluated and treated.
Disease of the dental pulp is referred to as endodontic disease and occurs primarily in horses between the ages of 4 and 10 years. This type of dental disease usually manifests as an infection and associated inflammatory changes at the apical region of the tooth. The clinical presentation depends on the structures adjacent to the apex of the affected tooth. Infections of the lower first four cheek teeth can manifest as ventral mandibular swellings with a draining tract. The last two lower cheek teeth are embedded in the portion of the mandible surrounded by the large muscles of mastication. These muscles are often enlarged or swollen, and ultrasound evaluation may reveal exudate accumulating between the mandible and muscle. The upper rostral two or three cheek teeth apices are closely associated with the facial bones and nasal passages. The caudal three or four upper cheek teeth are in the maxillary sinuses and can be associated with secondary sinusitis. Unilateral nasal discharge often occurs when the upper cheek teeth are affected. Because pulp disease compromises the tissue responsible for production of secondary dentine, the pulp horns and root canals on the affected teeth do not fill with secondary dentine as they should. In the later stages of pulp disease, the affected tooth usually shows some degree of pulp horn decay on the occlusal surface. This weakening and decay may predispose the affected tooth to crown fracture.34,35 Medical therapy has been successful in the management of apical disease in the early stages. Chronic apical infections are usually treated by removal of the tooth and treatment of any associated bone or sinus disease.
Equine cheek teeth have classically been removed by several surgical and nonsurgical methods:
• Extraction via oral approach (with or without tooth sectioning)
• Repulsion via apical or retrograde approach
• Elevation via lateral buccotomy/alveolectomy approach
More recently, minimally invasive procedures involving the use of small radiographically guided pins for repulsion or an oral trocar approach to teeth through the cheek have been developed.36,37
A progressive dental condition involving the incisor, canines, and premolars of aged horses has been described as equine odon- toclastic tooth resorption and hypercementosis (EOTRH).38 This disease is characterized by internal and external resorption of dental structures and is sometimes associated with excessive production of irregular cementum on the exterior and interior of the apical or root portion of the tooth. EOTRH is a progressive condition, but the pathophysiologic processes are still under investigation.39 Clinical signs include sensitivity in the mouth to any manipulation, head shyness, periodic inappetence and weight loss, and decreased use of incisors for grasping or grazing. Oral examination reveals varying degrees of gingival secession, calculus deposition, and firm bulbous enlargement of the incisive bone over incisor reserve crowns. Radiographs are needed to confirm a diagnosis and evaluate the severity of disease. Radiographic changes can include various forms and depths of tooth resorption, cemental thickening, osteosclerosis, osteitis and tooth fracture. This condition can be a painful, progressively debilitating disease of aged horses. No medical or husbandry changes have been identified to slow or change the course of disease. Extraction of painful or fractured unstable teeth appears to be the best method of managing these cases.40
Traumatic injuries to facial and dental structures are more common in young horses. Bones that support to teeth are often involved in these injuries, and a good dental alignment in the repair of these fractures is often more important than good bone apposition. Jaw and facial fractures can also involve the deciduous teeth, the developing buds of the permanent teeth, or both. Damage to a deciduous tooth can lead to dental drift and crowding of the eruption pathway for the permanent tooth. Permanent tooth bud damage can result from direct trauma or oral contamination by the damaged deciduous tooth. Facial fractures often lead to bone growth disruption, which predisposes horses to dental malocclusions. Tooth avulsion, subluxation, and total luxation are also observed. Diseased teeth in the fracture line can lead to dental or bone sequestum, delayed union, malunion or nonunion, oronasal or orosinus fistula, and osteomyelitis. Teeth in the fracture site should be preserved in most cases to add to stability of the fracture repair. Problems associated with periodontal or endodontal disease may be observed soon after the fracture has stabilized or may not show up clinically until many years later.
Fractures of the mandible and maxilla involving the teeth can be repaired successfully, but the health of the dental structures must be maintained for good long-term results. Most of the jaw and facial fractures involving the dental bearing bones are best managed by the least invasive approach. Intraoral wiring, alone or combined with a U-bar or acrylic splint, work wells and supports the compression side of the fracture. External fixation with a pinless external fixator provides less stability but is noninvasive and can be combined with oral wiring. Open reduction and internal fixation should be reserved for cases with few other options in stabilizing the fracture. Pins and screws should not be placed in the teeth because this often results in severe pulp damage.37
■ Salivary Glands and Ducts Saliva hydrates and lubricates the oral cavity, facilitates swallowing, prevents tooth demineralization, and regulates the oral flora.41 Diseases of the salivary glands and ducts, including sialoadenitis, salivary calculi, salivary mucocele, trauma, and neoplasia, are uncommon in horses. During oral examination, the openings of the salivary ducts should be noted. The parotid salivary duct communicates with the oral cavity via a flaplike, dorsally directed papilla, opposite the upper third or fourth check tooth. The mandibular salivary duct opens into the mouth on the lateral aspect of the sublingual caruncle. The sublingual salivary ducts (approximately 30 in number) are small pores in the sublingual recess.
Slobbering or drooling may indicate excessive accumulation of saliva in the mouth (sialism, ptyalism, or dysphagia). Heavy metal toxicity, parasympathomimetic poisoning, cholinesterase- inhibiting insecticides (organophosphates or carbamates), neurologic disease, and stomatitis may cause ptyalism. Slaframine is a cholinergic agonist that can cause “slobbers” in horses consuming forages, mostly commonly clover, contaminated with the fungus Rhizoctonia Ieguminicola. Tests for the presence of slaframine (1-acetoxy-6-amino-octahydroindolizine) are not readily available. Dysphagia can be caused by esophageal obstruction (choke), oral foreign body, rabies, or other neurologic disease.
Sialoadenitis may be the result of salivary duct obstruction caused by accumulation of exudate or mucus, by an ingested foreign body, or by a sialolith. Sialoliths develop in the parotid duct and can cause duct obstruction and salivary retention, which can lead to glandular atrophy or acute sialoadenitis, swelling, and rupture. On palpation, sialoliths are usually hard, smooth, and painless enlargements over the course of the parotid duct on the lateral aspect of the jaw. The diagnosis of sialolith is straightforward and differs from that of trauma, tooth abscess, and facial tumor. Surgical removal, usually orally, and primary closure often yield good results.
Salivary mucocele is an accumulation of salivary secretions in a single or multiloculated cavity adjacent to a ruptured salivary duct. A ranula is a type of mucocele that is secondary to obstruction of the sublingual salivary duct. Treatment consists of creating a salivary fistula into the oral cavity or excising the mucocele and associated salivary gland.
Laceration or iatrogenic injury to the salivary ducts can lead to salivary cutaneous fistula. These injuries can be surgically repaired by reapposition of the severed duct and creation of an oral opening for the duct or by resection of the salivary gland. Oblation and sclerosis of the gland has been achieved by flushing of the duct with 1% formalin solution. Wounds involving the salivary glands can usually be handled by cleansing, debridement, and primary skin closure.
Benign mixed tumors, adenocarcinomas, and acinar cell tumors of the salivary glands have been reported in horses. Local invasion of a salivary gland by tumor originating in adjacent tissues and metastasis of melanomas to the parotid salivary gland in older gray horses are more common.
■ Equine Oral Tumors Equine oral tumors are rare, making up a very small percentage of the facial or mandibular swellings. These tumors can be divided into three basic types: odontogenic, osteogenic, and secondary.42,43
Odontogenic tumors are derived from remnants of dental epithelium. Five types have been recorded in the maxillas and mandibles of horses: ameloblastomas, ameloblastic odontomas, complex odontomas, compound odontomas, and cementomas. Because of their rarity, ill-defined biological behavior, and poorly defined radiographic features, diagnosis can be difficult. Histopathologic findings can be confusing because their appearance varies at different sampling sites and because of age-related changes in tumor appearance.
Primary bone tumors are rare in horses and if present, they are usually benign. More than 80% of equine osteosarcomas occur in the head region. As is the case with odontogenic tumors, disagreement remains with regard to histologic classification, terminology, and nature of tumor. In addition to gross and histologic examination, clinicians and pathologists often must find a correlation between the history and clinical, radiologic, and some biochemical findings to establish a diagnosis. Ossifying fibroma can occur in young horses and usually involves the rostral mandible.
Secondary tumors of the head include extensions of oropharyngeal squamous cell carcinoma, lymphosarcoma, papilloma, and melanoma. Squamous cell carcinoma is the most frequently reported oral tumor in horses. In general, these tumors are seen in older horses and have no gender or breed predilection. There are many treatment options and methods of controlling the progression of oral tumors. Radiotherapy, hyperthermia, chemotherapy, cryosurgery, immunotherapy, autogenous vaccines, photodynamic therapy, laser therapy, and surgical resection have been used with variable success.
■ Dental Examination Biannual dental examination of horses should be part of a routine health maintenance program. Improved eating efficiency and oral hygiene are the most important considerations from a medical standpoint. However, often owners are more enthusiastic about dental care because of its positive effects on a horse's sensitivity to the bit and athletic performance. Written documentation of dental examination findings is necessary to formulate a problem-oriented treatment plan and monitor age-related dental changes and progress after maintenance, treatment, or both (Fig. 32.42). A consistent routine followed by the examiner increases the efficacy and quality of the examination (Box 32.1).44,45
Several signs may be noted in the history or observed in a horse suffering from dental problems. A history of abnormal head carriage or head tossing when the horse is being ridden or eating, longer time taken to eat, halitosis, dysphagia, drooling or hypersalivation, dribbling feed (quidding), and eating hay before grain suggest that a dental problem exists. Indicators
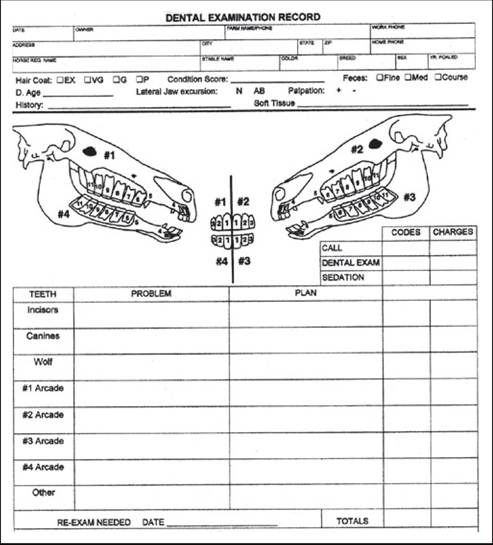
FIG. 32.42 Dental record form used to document dental examination findings and treatments performed.
■ BOX 32.1
Recommended Timetable for Routine Dental Examinations and Common Corrective Procedures
Birth
1. Examine for congenital defects of lips or palate.
2. Assess tongue motion and strength.
3. Identify dental malocclusions.
4. Evaluate all body systems.
Recommended Procedures
1. Provide genetic and orthodontic consultation, and perform corrective surgery if necessary.
2. Look for other problem signs such as underdeveloped carpal or tarsal bones, ruptured extensor tendons, and hernias.
6 to 8 Months of Age
1. Check incisor and premolar occlusions.
2. Check to see that all incisors have erupted.
3. Check for sharp enamel points or hooks.
4. Check tongue and buccal mucosa for ulcers.
Recommended Procedures
1. Provide orthodontic consultation, and float teeth if necessary.
16 to 24 Months of Age
1. Check for expanded eruption of lower wolf teeth.
2. Check points and hooks on premolars.
3. Look for bit lesions.
Recommended Procedures
1. Float teeth and round off rostral corner of premolar 2.
2. Extract wolf teeth.
2 to 3 Years of Age
1. Look for upper and lower wolf teeth.
2. Check corners of mouth and interdental space for bite injuries.
3. Evaluate incisors and molars for eruption and premolars for points and loose or retained deciduous teeth.
Recommended Procedures
1. Float outside of upper and inside of lower cheek teeth.
2. Remove caps if present and ready.
3. Extract wolf teeth.
3 to 4 Years of Age
1. Check corners of mouth and interdental space for bit injuries.
2. Evaluate incisors for retained deciduous teeth or supernumerary teeth.
3. Evaluate molars for eruption and premolars for points and retained or loose deciduous teeth.
4. Evaluate size and shape of lower jaw and percuss sinuses.
5. Check for blind wolf teeth.
Recommended Procedures
1. Remove caps if present and loose.
2. Float teeth.
3. Remove wolf teeth.
4 to 5 Years of Age
1. Check all incisors for eruption and wear occlusion.
2. Check canine teeth for sharp edges or eruption delays.
3. Evaluate entire molar arcade for proper eruption and alignment (third cheek tooth).
4. Visually check upper rostral and lower caudal cheek teeth for hooks from malocclusion.
5. Digitally check for points on sharp edges of cheek teeth.
6. Percuss sinuses.
Recommended Procedures
1. Remove deciduous teeth if loose and ready.
2. Reduce hooks if present.
3. Float teeth.
4. Remove mucosa over canines if gingival cysts are present.
5 Years and Older
1. Examine mouth visually and digitally, especially noting hooks and uneven wear.
2. Evaluate canines for sharp edges and tartar.
3. Percuss sinuses.
4. Use olfactory senses to detect evidence of oral decay or gingivitis.
5. Observe incisors for even wear.
6. Evaluate lateral jaw excursion.
Recommended Procedures
1. Float teeth.
2. Remove hooks.
3. Level or shorten incisors if indicated.
of dental problems in performance horses include tail wringing, headshaking, lunging in or out on the track, and fighting the bit (refusing to collect the head). Chronic colic or choke can result from improper mastication of feed. Reluctance to drink cold water may be a result of dental pain.19,20,46
Good dental health is extremely important to the equine digestive system. Proper mechanical digestion of feed allows better carbohydrate absorption in the small intestine and improved fiber fermentation in the cecum and large colon. Improperly masticated roughage and concentrate leads to poor digestibility in the small and large intestine because of large feed particles with decreased surface area per mass. This decreased surface area does not allow proper enzyme degradation or bacterial fermentation. Findings of whole grain or stem particles longer than 5 mm during manure examination indicate improper mastication.
As a routine aspect of the dental examination, a horse's overall condition should be evaluated in view of its use and dietary intake. A body score should be assigned, as this is a more accurate way to subjectively record body condition47 (Table 32.1). Objective assessment of body condition with the use of a scale, weight tape, or photographs is also beneficial and provides good data to assist in proper documentation and management.
The age of a horse should be considered during evaluation.48 Different conditions need to be addressed for each stage of the horse's growth, development, and maturity. The use of the horse should be considered during evaluation because dental care for horses that wear a bit might differ from dental care for horses that do not wear a bit. Stable surroundings should be carefully observed for evidence of vices (such as cribbing) or poor eating habits (such as quidding or dribbling grain).
The physical examination begins with observation of the horse's body condition, attitude, and temperament. The horse should be approached from the left side of the shoulder. Body and head conformation should be considered during evaluation of the masticatory system. Horses with small heads have more of an angle in the curve of the mandibular ramus (i.e., curvature
■ TABLE 32.1
Principles to Guide Health Care Transformation in Canada
| Condition | Neck | Withers | Shoulder | Ribs | Loin | Tailhead |
| 1. Poor | Bone | Bone | Bone | Ribs | Spinous processes | Tailhead, pinbones, |
| structure | structure | structure | protruding | projecting | and hook bones | |
| easily noticeable | easily noticeable | easily noticeable | prominently | prominently | projecting prominently | |
| 2. Very thin | Bone structure faintly discernible | Bone structure faintly discernible | Bone structure faintly discernible | Ribs prominent | Slight fat covering over base of spinous processes Transverse processes of lumbar vertebrae feel rounded Spinous processes are prominent | Tailhead prominent |
| 3. Thin | Bone | Bone | Bone | Slight fat | Fat buildup | Tailhead prominent, |
| structure | structure | structure | cover over | halfway on | but individual | |
| accentuated | accentuated | accentuated | ribs Ribs easily discernible | spinous processes, but easily discernible Traverse processes cannot be palpated | vertebrae cannot be identified visually Hook bones appear rounded but are still easily discernible Pin bones not distinguishable | |
| 4. Moderately | Neck not | Withers not | Shoulder not | Outline of ribs | Negative crease | Prominence depends |
| thin | obviously | obviously | obviously | faintly | (peaked | on conformation |
| thin | thin | thin | discernible | appearance) along back | Fat can be felt; hook bones not discernible | |
| 5. Moderate | Neck blends | Withers | Shoulder | Ribs cannot | Back is level | Fat around tailhead |
| (ideal | smoothly | rounded | blends | be visually | beginning to feel | |
| weight) | into body | over spinous processes | smoothly into body | distinguished but can be easily palpated | soft | |
| 6. Moderately | Fat | Fat | Fat | Fat over ribs | May have a slight | Fat around tailhead |
| fleshy | beginning to be deposited | beginning to be deposited | beginning to be deposited | feels spongy | positive crease ?(a groove) down back | feels soft |
| 7. Fleshy | Fat deposited | Fat deposited | Fat deposited | Individual ribs | Positive crease | Fat around tailhead is |
| along neck | along withers | behind shoulder | can be felt with pressure, but noticeable fat filling between ribs | may be present down the back | soft | |
| 8. Fat | Noticeable | Area along | Area behind | Difficult to | Positive crease | Fat around tailhead |
| thickening of neck | withers filled with fat | shoulder filled in flush with body | feel ribs | down the back | very soft | |
| 9. Extremely fat | Bulging fat | Bulging fat | Bulging fat | Patchy fat appearing over ribs | Obvious crease down the back | Bulging fat around tailhead |
of Spee) and are predisposed to dental crowding and ramps on the lower dental arcades. The head is observed from both sides and the front, and any asymmetries, protuberances, or swellings should be noted. The tongue is checked for proper movement, abnormal swellings, or signs of trauma or injury; the horse's ability to swallow is checked as well. Lacrimation should be noted, as well as any nasal discharge. Neurologic evaluation should be considered if any cranial nerve deficits are detected. Finally, the examiner assesses the head by palpating the mandibular rami, masticatory muscles, temporomandibular joints, and submandibular lymph nodes to detect enlargements or asymmetry.
The frontal and maxillary sinuses should be percussed with the horse's mouth open. The width between the mandibular ramus should be noted because this is correlated with the room in the mouth for the bit. The sides of the head lateral to the upper dental arcade should be compressed from the orbit, moving forward to the first cheek tooth at the level of the nasal notch; any protuberances, depressions, asymmetry, or evidence of pain should be noted.
The commissures of the lip should be observed and palpated for signs of trauma from sharp teeth or improperly fitting bits. A loose-fitting halter is necessary to properly evaluate the mouth and oral cavity. If the horse is fractious or resists examination, a sedative should be administered before the oral portion of the examination. Sedation should be induced after a medical assessment of the animal (i.e., consideration of temperament, breed, age, body condition, mucous membranes appearance, central reaction time, heart rate and rhythm, and rectal temperature).
The mouth should be rinsed thoroughly with clean water. Impacted or trapped feed in the mouth should be removed manually or with the use of a dental pick and irrigation. Many horses with sharp buccal points on the upper dental arcade resist the full-mouth speculum. Floating the upper arcades before applying the speculum may decrease a horse's resistance. With a full-mouth speculum in place and the head properly restrained, a detailed visual and tactile oral examination can be carried out. A bright light source is necessary to illuminate the entire oral cavity for complete visual inspection. An examiner should manually inspect all hard and soft tissue in the oral cavity. Use of dental mirror, occlusal hook pick, and calibrated periodontal probe is often necessary to see and probe the occlusal surfaces and pockets between the cheek teeth. An oral endoscopic camera can aid in the completeness of the oral
49
examination.4
■ Dental Imaging Diagnostic radiology is a valuable aid in the diagnosis and management of equine dental disease. Because of the excellent contrast among air, bone, soft tissue, and tooth substance, the head is an excellent area for radiologic evaluation. Good-quality films can be obtained with portable x-ray machines and rare-earth intensifying screens without a grid. Digital and computed radiology have improved radiographic image quality and allow for high-quality images to be shared electronically for consultation with colleagues.
Indications for radiographic examination of the head include a suspicion of dental infection, maleruption, diastema, or oral pain of unknown origin. Radiographs should be obtained before, during, and after dental extraction. Any abnormal dental finding, facial swelling, deformity, neoplasm, trauma, or fracture may warrant radiography to aid in diagnosis and management.
Radiographs can be taken in a standing, sedated horse. The technique for acquiring excellent images in the field has been reviewed.50 The website of the American Veterinary Dental College also has a good example set of dental radiographs that can be viewed for reference (AVDC.com). The head and radiographic cassette can be placed on a stand to decrease motion distortion. A lateral view centered over the rostral edge of the facial crest demonstrates fluid lines, if present, in the sinuses. The lateral view superimposes the dental arcades and should not be relied on to diagnose diseases involving the dental reserve crown and roots. Lesion-oriented oblique films demonstrating the root or apical portion of the upper or lower cheek teeth are helpful in diagnosis of periapical disease. Open-mouth oblique films are beneficial in evaluating the exposed crown of the dental arcades. Special 4-inch ? 8-inch (10 cm ? 30 cm) flexible dental cassettes can be used to obtain intraoral radiographs of the maxillary dental arcades. Dorso- ventral views centered over the tooth in question or area of concern can demonstrate periodontal disease on the buccal aspect of the upper cheek teeth, fractured teeth, or large area of infundibular decay. Intraoral occlusal films are useful in demonstrating incisor lesions or fractures rostral to the bars of the mouth. Other imaging techniques, such as ultrasonography, nuclear scintigraphy, CT, and MRI are useful in the diagnosis of many oral and dental diseases.51,52
■ Treatment A plan for treatment should be based on the results of history, clinical findings, oral examination, and imaging before any dental work is begun. This problem-oriented approach ensures that the owner, the trainer, or both are informed of any abnormalities and are given a plan for treatment, as well as an estimate of the cost, before any corrective procedure is taken.
Therapy must be planned to ensure that all equipment is present to complete the prescribed task. The horse should be properly restrained and adequate help should be present to assist in performing and completing the corrective or surgical procedures. A dental record form should be used to document examination findings, treatment plan, and procedures performed (see Fig. 32.42).
Routine Dental Maintenance
floating (Odontoplastyof enamel points and dental CROWN ELONGATIONS). Dental floating is an age-old and routine method of correcting the abnormal wear patterns associated with equine dental eruption and occlusal wear. Floating is also a procedure that allows the sculpting of the teeth to accommodate the bit. The main purpose of molar floating (leveling) is to remove points or sharp edges from the buccal aspect of the upper and lingual aspect of the lower molar arcades. Floating may also entail removing minor hooks or ramps from the rostral or caudal aspect of the arcades or leveling minor elevations on the occlusal surface of the arcades.
Proper equipment is necessary to reach all aspects of the cheek teeth molar surfaces completely, regardless of horse size. Smaller instruments are often needed to access the oral cavity of a miniature horse or pony. Longer, heavier instruments are often used to work in the mouths of large, Warmblood, or draft horse breeds. Sharp float blades made of carbide chips or tungsten carbide planning blades make the work of floating more efficient and less strenuous than in the past. The outward curve of the upper arcade makes the central buccal area involving premolar 3 (PM3) through molar 2 (M2) the easiest to reach with the float. For the area around PM2 and M3, an offset or angled head on the rasps is needed to reach all extremities. In most cases the lower arcade can be floated to remove the lingual enamel points with a flat, long-handled rasp. To correct rostral and caudal hooks, specialized tools such as carbide planing blades or power burrs may be required. The use of all dental equipment requires special training and skill to prevent iatrogenic injury to the horse's mouth.
Use of a full-mouth speculum aids in the oral examination and floating procedures, ensuring that the horse's mouth is kept in an open, safe (for the examiner as well as the animal) position for floating. In horses whose back teeth are slightly ramped back because of a greater curvature of Spee, a mouth speculum and a slightly curved or swivel-head float may be necessary to reach the table of the last molar.
In horses wearing bits, the rounding of the first upper and lower cheek teeth and lowering of the buccal cusps from upper PM2 and PM3 is referred to as a “bit seat” and usually requires an offset float or an S-shaped rasp. In theory, a bit seat is fashioned to prevent the soft tissue of the mouth from pressing against sharp points on the first premolars. To prevent pulp cavity exposure, care should be taken not to “overfloat” the occlusal surface of a tooth when bit seats are formed or overgrowths are corrected because this could lead to a direct pulp horn exposure.5 Routine floating and other corrective measures in the mouth may require the added physical restraint of a dental halter and mild chemical sedation.
WOLF TEETH. Wolf teeth are the first premolars to erupt and are present in 20 to 80% of horses. They are most often located in the upper arcade and seldom in the lower arcade. Horses that are worked with a bit in their mouth benefit from having the wolf teeth extracted. Some wolf teeth are naturally exfoliated at approximately 3 years of age when the first cheek teeth (or 06 caps) are shed and the permanent tooth erupts. Although not all wolf teeth cause problems, a loose or sharp wolf tooth can be a distraction or even cause pain of such severity as to lead to bad bitting habits. In some instances, diagnosis of wolf tooth problems is difficult and confusing. Sometimes they do not erupt in a normal downward path, penetrating the gum; rather, they may migrate rostrally under the gum and causing a subgingival enlargement, which in turn, is irritating to affected horses. Such unerupted first premolars have been referred to as “blind” wolf teeth and should be removed. Most wolf teeth are easily elevated with the horse sedated or after a small volume of local anesthetic is instilled around the tooth.
CANINE TEETH. Canine teeth are present in most male horses older than 4 years of age. Because of their unopposed position in the bars of the mouth, they are unlikely to cause problems. Some mares have small or rudimentary canines that do not seem to cause a problem but can become loose or accumulate tartar and must be removed. Long or sharp canines in a stallion or gelding can interfere with bitting, be a nuisance or a danger to the groomer/handler, or become an area of tartar accumulation. Erupting canine teeth in 4- to 6-year-old horses may cause an operculum to form and lead to subgingival pain and bit irritation, which may manifest as headshaking or other bad habits. The thin layer of tender mucosa should be removed over the canine if the gingival operculum is present. Severe calculus accumulation can be present on the lower canines, which predisposes horses to periodontal disease. Scaling calculus and frequent brushing of lower canines can control this problem in most horses.
The canine roots are long and curved, and thus this tooth is extremely difficult to extract in the male. If the canine becomes injured, infected, or involved in painful odontoclastic tooth resorption, surgical removal through a bone flap is indicated.53
DENTAL CAPS. As the developing permanent tooth (incisor or premolar) pushes toward the surface, it presses on the roots of the worn-down deciduous tooth, gradually cutting off that tooth's nutrition. The deciduous tooth becomes loose, its blood supply diminishes, the tooth dies, and it is displaced occlusally. The osseous alveolar wall adjusts to these changes by bone production and resorption, thereby providing a new socket for the embedded portion of the newly formed permanent tooth. The remaining cap portion of the deciduous tooth has up to four “legs” (root slivers) that cover the crown of the permanent tooth. If these slivers are broken off and remain subgingivally after the cap has been shed, gingivitis and periodontal disease often result.
The eruption pattern of permanent molarized dentition follows a sequence that predisposes to entrapment of deciduous PM3 and PM4.54 Delayed shedding of deciduous premolars can predispose horses to gingivitis, periodontal irritation, or apical infection. Retained, split, or displaced deciduous premolars can be distracting in the training process of a young horse and may be a factor in dorsal displacement of the soft palate.
Retained caps can cause displacement or delayed eruption of permanent teeth. Clinically, they manifest as bony enlargements on the ventral mandibular ramus or on the maxilla, rostral to the facial crest. Often, such swellings are benign. However, they can become diseased if eruption is severely inhibited or bloodborne bacteria inhabit the inflamed dental pulp, which leads to anachoretic pulpitis and bony swelling with a draining tract. Caps should be evaluated visually as well as by manual palpation. A crease or indentation can be felt just above the gum line at the juncture of the separating deciduous and permanent tooth. Radiographs may be necessary to diagnose retained deciduous premolars.