Disorders of the Esophagus
Samuel L. Jones • Anthony T. Blikslager
■ Anatomic and Physiologic Considerations The most cranial aspect of the esophagus is located on the median plane immediately dorsal to the trachea.
However, at approximately the midcervical region (C4 to C5), the esophagus typically shifts to the left of the trachea and lies just deep to the external jugular vein.1,2 It is here that intraluminal obstructions or the tip of a stomach tube may be visualized, and this is the region where trauma can readily result in esophageal perforation. When a stomach tube is passed, it must be palpated to ensure that it is in the esophagus because jugular pulses can be confused with the appearance of the tip of the tube. In addition to its proximity to the external jugular vein, the esophagus is also adjacent to the vagosympathetic trunk and the common carotid artery.1 The esophagus is innervated by branches of the vagosympathetic trunk, and blood is supplied to the cervical portion of the esophagus by branches of the carotid arteries. The thoracic portion of the esophagus—which lies ventral to the trachea until it reaches the tracheal bifurcation, where it resumes a dorsal position—receives its blood supply from the bronchoesophageal artery. Venous drainage is via the external jugular veins in the cervical portion of the esophagus, and the esophageal vein in the thoracic portion of the esophagus.The muscular wall of the esophagus increases in thickness as the esophagus courses distally, whereas the lumen shrinks.1 The esophagus is not covered by a serosa except for a very short segment that traverses the abdominal cavity between the diaphragm and the stomach.2 Instead, the outer wall of the esophagus is composed of adventitia that is loosely attached to surrounding tissues. This loose connection allows movement of the esophagus during swallowing and during movement of the neck.
The cranial two thirds of the esophageal wall consists of skeletal muscle, whereas the distal third of the esophageal wall is composed of smooth muscle. Although the muscular layers, like those in the remainder of the gastrointestinal tract, are composed of an outer and an inner layer, the skeletal muscle layers are oriented obliquely to one another.1 This, and an abundant submucosa, enables extensive dilation of the esophagus as a bolus of food moves toward the stomach. In addition, the velocity of esophageal contraction is faster in the skeletal muscle segment of the esophagus than in the distal smooth muscle segment.3 The muscle layers become oriented in more of an outer longitudinal and inner circular configuration in the caudal portion of the esophagus.1 In the resting collapsed state, redundant esophageal mucosa and submucosa become oriented in longitudinal folds. The mucosa is composed of stratified squamous epithelium that is continuous with the stratified epithelium of the cardiac portion of the stomach.1The cranial portion of the esophageal sphincter is formed by the cricopharyngeus muscle and maintains a resting intra- esophageal pressure of approximately 85 mm Hg and a postdeglutition pressure as high as 200 mm Hg. Although the caudal portion of the esophageal sphincter is anatomically indistinct, resting intraesophageal pressure in this region is maintained at approximately 13 mm Hg, and postdeglutition pressure in the caudal portion of the esophagus may be as high as 100 mm Hg. The pressure in the caudal portion of the esophagus is maintained at approximately 10 mm Hg higher than the intraluminal pressure of the stomach.3,4 Although the higher pressure in the distal esophagus has been implicated as the cause of the inability of most horses to vomit and for gastric rupture, other factors such as a poorly developed vomiting reflex may be more important.5
■ Diagnostic Considerations Esophageal disease should be part of the differential diagnosis in any horse that demonstrates excessive salivation.
Such signs also indicate the need to assess hydration, electrolyte levels, and acid-base status. In a study in which horses had continual loss of saliva via an experimentally placed esophagotomy, abnormalities included hypochloremia, hyponatremia, and hypokalemia.6 This results from the relatively high levels of these electrolytes in saliva. Furthermore, because horses depend on dietary intake of potassium, hypokalemia would be exacerbated in a horse that was also unable to eat because of esophageal obstruction. Loss of salivary fluid and bicarbonate also results in dehydration and metabolic acidosis. However, metabolic alkalosis subsequently occurs, presumably as a result of renal compensation for loss of electrolytes, particularly chloride.6Further examination of horses with esophageal disease may reveal evidence of swelling or emphysema in the region of the cranial or cervical portion of the esophagus that should prompt a thorough oral examination and further diagnostic studies such as radiography and endoscopy to define the nature of any esophageal abnormalities. If the esophagus has been perforated or ruptured, subcutaneous emphysema is usually evident. The lungs should be carefully auscultated for evidence of aspiration pneumonia. Radiographs of the chest are required for a full pulmonary assessment.
Radiographs of the esophagus should initially include plain films that may reveal evidence of an obstruction or areas of gas opacity within facial planes indicative of esophageal perforation.7 However, facial and subcutaneous emphysema must be differentiated from other causes, including tracheal perforation.5 The esophagus is often distended with gas cranial to an obstruction up to the cranial portion of the esophageal sphincter. Plain radiographs may be diagnostic, but contrast radiographs are frequently necessary to fully define the nature of esophageal abnormalities.7 Administration of barium paste or liquid helps reveal linear opacifications as a result of the linear mucosal folds and may help outline intraluminal obstructions or strictures (Fig.
32.43).7 A double-contrast study is a useful radiographic technique for defining esophageal wall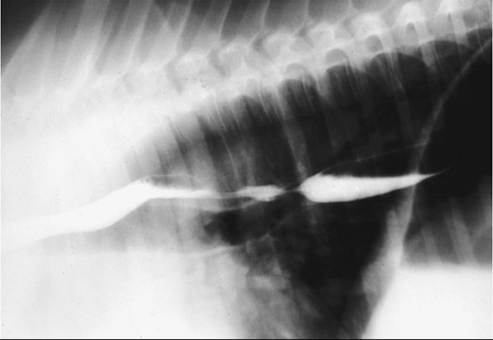
FIG. 32.43 Barium contrast medium-enhanced esophagogram outlining esophageal luminal structure. (Courtesy Dr. K.E. Sullins.)
abnormalities, particularly postobstruction mucosal ulceration. For this study, a cuffed nasogastric tube is placed in the cranial portion of the esophagus, and 300 to 500 mL of liquid barium is injected, followed by a similar volume of air. Care should be taken in evaluation of such radiographs because swallowing can create the false impression that there is a stricture.8 The incidence of swallowing can be decreased by administration of xylazine or detomidine. Liquid barium is preferable if swallowing function is compromised because it is less harmful to pulmonary tissues than is paste, and water-soluble iodinated contrast material is particularly damaging to the lung because of its hypertonicity.5 However, if an esophageal perforation is suspected, water-soluble contrast material is preferable.5
Ultrasonographic examination of the cervical portion of the esophagus is often helpful to identify the exact location of obstructions and to determine whether abnormalities of the esophagus are present. Perforations can be identified by periesophageal gas patterns. Whereas intraluminal contents often cannot be examined with ultrasonography because of the presence of air, abnormalities of the mucosal or muscularis layers can be identified. Intramural or extramural causes of esophageal problems (particularly obstructions) may be discovered through ultrasonography. The location and characteristics of masses (e.g., neoplasia, granulomas, abscesses) may be evaluated more readily with ultrasonography than with radiography or endoscopy. The thoracic portion of the esophagus, however, cannot be evaluated with ultrasonography.
The esophagus should be evaluated endoscopically as part of a complete evaluation of esophageal injuries and abnormalities. After the patient is sedated, the endoscope should be passed all the way into the stomach before the esophagus is examined; the esophagus is viewed more easily as the endoscope is withdrawn.7 Inflation of the esophagus must also be performed intermittently because the wall of the esophagus periodically collapses around the end of the endoscope. The longitudinal folds of the esophageal mucosa are readily appreciated and can be flattened out as the esophagus is distended to view the entire circumference of the esophagus more clearly. Swallowing may create artifacts such as the appearance of strictures, so the esophagus should be carefully reinflated after each swallow to carefully evaluate such findings.8
The mediastinum, including the thoracic component of the esophagus, may be evaluated via thoracoscopy. Although this procedure caused pneumothorax in one case, a 15-minute period of evaluation allowed observation of numerous structures, including the esophagus.9 Portals placed at the eighth, tenth, and twelfth intercostal spaces were useful for completion of this procedure and could provide additional information aside from radiographic and endoscopic evaluation of the thoracic portion of the esophagus.
■ Esophageal Obstruction Esophageal obstruction, either primary (simple choke) or secondary to other disease processes, is the most common esophageal disorder in horses. Although primary obstructions may be caused by foreign bodies (including corncobs, potatoes, apples, carrots, medicinal boluses, stones, riding crops, or wood fragments), primary obstructions are most often caused by roughage, particularly leafy alfalfa hay, coarse grass hay, bedding, and even grass.10-20 Prior esophageal trauma or poor mastication caused by dental abnormalities may predispose horses to esophageal impaction.
Obstructions from roughage may be precipitated by wolfing or gulping food, particularly if an affected horse is exhausted or mildly dehydrated (such as after a long ride) or weakened from chronic debilitation. Secondary impactions are caused by intramural or extramural abnormalities that mechanically impede food passage. Examples of intramural obstructions include tumors (squamous cell carcinomas), strictures, diverticula, cysts, and vascular ring anomalies.21-27 Mediastinal or cervical masses (tumors or abscesses) may cause extramural obstructions.Regardless of whether obstructions are classified as primary or secondary, the associated clinical signs are similar and are rarely specific. Many horses with esophageal obstruction are anxious and stand with the neck extended. Gagging or retching may be noted, particularly with acute proximal obstructions. Bilateral frothy nasal discharge containing saliva and food material, coughing, odynophagia, ptyalism, and dysphagia are usually the primary clinical signs, the severity of which varies with the degree and location of the obstruction. Distention of the cervical portion of the esophagus may be evident at the site of obstruction. Other clinical signs may be observed related to complications stemming from the obstruction, such as dehydration, weight loss, aspiration pneumonia, or esophageal rupture.
Thorough physical examination, including a complete oral examination, must be performed to rule out other causes of hypersalivation, dysphagia, and nasal discharge. Palpation of the jugular furrow may reveal a mass associated with the impaction. In most horses the esophagus is in the left jugular furrow, but it is in the right furrow in some animals. Crepitus or cellulitis may be evident, which suggests rupture of the esophagus. Auscultation of the lungs can determine whether pneumonia or pleural fluid is present because of aspiration or intrathoracic esophageal rupture. Passage of a nasogastric tube is a good way to determine whether and where an obstruction is present, but it provides little information about the nature of the obstruction or the condition of the esophagus.
Ultrasonography of the cervical region is extremely useful not only to confirm the presence of an impaction in the cervical portion of the esophagus but also to provide critical information about the location and extent of the impaction and esophageal wall thickness and integrity. Ultrasonography may also provide information about the cause of the obstruction. Radiography, particularly air or barium contrast studies, are useful for assessing an esophageal impaction but may be more useful for evaluating the esophagus after, rather than before, relief of the impaction to demonstrate stricture, dilation, diverticula, esophageal rupture, or masses.28,29 Care should be taken in interpretion of radiographic studies in sedated horses, particularly after passage of a nasogastric tube or other esophageal manipulations that may contribute to esophageal dilation.30 Impacted food material can be detected in the esophagus as a typical granular pattern, and gas is often observed to accumulate proximal to the obstruction. Foreign bodies may be identified by contrast radiographic studies.
Definitive evaluation of esophageal obstructions often necessitates endoscopic examination. Most cases of esophageal obstruction occur at sites of natural narrowing of the esophageal lumen, such as the cervical portion of the esophagus, the thoracic inlet, the base of the heart, or the terminal esophagus; therefore an endoscope longer than 1 m may be required. The endoscope can be used to localize and investigate the nature of the impaction if a foreign body is suspected. Foreign bodies may be retrievable via transendoscopic tethering.18 Critical diagnostic and prognostic information is obtained after resolution of the impaction to determine whether mucosal ulceration, esophageal rupture, masses, or strictures are present.
The primary goal of treatment for esophageal impaction is to relieve the obstruction. Parenteral administration of acepromazine (0.05 mg/kg IV), xylazine (0.25 to 0.5 mg/kg IV) or detomidine (0.01 to 0.02 mg/kg IV), oxytocin (0.11 to 0.22 IU/kg IM), esophageal instillation of lidocaine (30 to 60 mL of 1% lidocaine), or a combination of these may help reduce esophageal spasms resulting from pain or increased esophageal tone.15,30-32 However, conclusive studies have revealed that detomidine, acepromazine, or a combination of xylazine and butorphanol had the greatest effect on esophageal motility when evaluated by a monomer in conscious horses.33 In vitro studies revealed a relaxant effect of oxytocin on esophageal muscle, which suggests it may be useful for relief of esophageal obstruction.34
Resolution of an impaction may necessitate physical dispersal of the material. A nasogastric tube can be used to displace the impacted material in conjunction with external massage if the obstruction is in the cervical region. Often it is necessary to carefully flush the esophagus with water via an uncuffed or a cuffed nasogastric tube while the horse's head is lowered to aid in breaking up the impaction. Some clinicians advocate a dual-tube method whereby a tube is placed through each nasal passage into the esophagus for ingress and egress of the lavage fluid. Because of the risk of aspiration of water, food, or both, esophageal lavage is sometimes done with a cuffed nasotracheal tube while the horse is under general anesthesia.
In refractory cases, intravenous administration of isotonic fluid containing 0.9% NaCl and KCl (10 to 20 mEq/L) for 24 hours at a rate of 50 to 100 mL/kg/day, in conjunction with an esophageal relaxant such as oxytocin, may promote hydration and softening of the impaction. Moreover, this helps prevent or alleviate any electrolyte or acid-base imbalances resulting from salivary losses of chloride, sodium, and potassium. Refractory cases may necessitate esophagotomy to relieve the impaction. Restriction of access to food, water, and bedding material must be enforced until the obstruction is resolved and the esophagus has regained function.
Dilation proximal to the site of obstruction, mucosal injury from trauma, and esophagitis are sequelae to esophageal impaction that predispose patients to reobstruction (Color Plates 32.1 and 32.2). The rate of reobstruction may be as high as 37%. Depending on the duration of the obstruction and the degree of trauma or dilation, the risk of reobstruction is high for 24 to 48 hours or longer; therefore food should be withheld for at least 24 to 48 hours after resolution of the obstruction. After 48 to 72 hours or when the esophageal mucosa has recovered as assessed by endoscopy, soft food (moistened pellets and bran mashes) can be fed to the horse. The patient can be returned to a high-quality roughage diet over a period of 7 to 21 days, depending on the degree of esophageal damage induced by the impaction and the nature of any underlying disease. The prognosis for survival is good (78%), but some horses may require permanent dietary modification if persistent chronic obstruction is a problem.17
Complications of esophageal impaction include esophageal ulceration, stricture, perforation, aspiration pneumonia, megaesophagus, and metabolic alkalosis from prolonged loss of salivary chloride and sodium. Esophageal endoscopy, ultrasonography, or both should be performed immediately after the impaction is relieved to determine whether any complications of the impaction have developed or whether an inciting cause of the obstruction is present. Endoscopic evaluation is critical to determine the postobstruction treatment and follow-up. Reevaluation should be performed intermittently every 2 to 4 weeks after resolution of the impaction if esophageal dilation or mucosal injury is noted. Additional evaluation with radiography may be warranted to assess motility and transit times.
If the obstruction was present for 48 hours or longer, dehydration, hyponatremia, hypochloremia, and hypokalemia may occur and should be corrected with oral electrolyte solutions or intravenous administration of 0.9% NaCl and KCl (10 to 20 mEq/L). If aspiration is suspected, broad-spectrum antibiotics that are effective against Gram-positive and Gramnegative organisms, including metronidazole for anaerobes, should be administered. Sucralfate (20 mg/kg orally [PO] q6h) may hasten healing if esophageal ulceration is evident, but this is controversial. Some clinicians suggest that administration of an NSAID such as flunixin meglumine (1 mg/kg PO or IV q12h) or phenylbutazone (1.1 mg/kg PO or IV q12h) for 2 to

FIG. 32.44 Severe ulceration of the esophagus in a weanling foal that had severe duodenitis and gastric outflow obstruction. (Courtesy Dr. MJ. Murray.)
4 weeks after resolution of the impaction may limit the development of strictures.
■ Esophagitis Inflammation occurs during many conditions of the esophagus. Esophagitis refers to a clinical syndrome of esophageal inflammation, which may or may not be ulcerative. Causes of esophagitis in horses include trauma (foreign bodies, nasogastric tube), infection (mural abscesses), and chemical injury (acidic medicines, cantharidin).35,36 An important category of esophagitis is reflux esophagitis, caused by reflux or delayed clearing of gastric contents into the distal esophagus and subsequent chemical injury to the mucosa (Fig. 32.44). As with ulceration of the squamous portion of the stomach in horses, a major cause of ulcerative esophagitis is epithelial damage resulting from exposure to acid, which is synergistically exacerbated by bile salts.11,37 The major protective mechanisms of the esophageal mucosa include salivary and food material buffers, normal peristaltic motility, and the barrier formed by the gastroesophageal sphincter. Thus esophagitis may accompany gastric ulcer disease, motility disorders, increased gastric volume from gastric outflow obstructions, gastric paresis, intestinal ileus, or impaired function of the lower portion of the esophageal sphincter.
The clinical signs of esophagitis are nonspecific and similar to those of esophageal obstruction and gastric ulcer disease. In fact, esophagitis may occur concurrently with esophageal obstruction or gastric ulcer disease, so clinical signs may overlap extensively with those of these diseases. Gagging or discomfort when swallowing may be evident, and hypersalivation and bruxism are signs of esophageal pain. Horses with chronic esophagitis may have partial or complete anorexia to such a degree that they exhibit significant weight loss. Motility dysfunction secondary to esophagitis may cause recurrent esophageal impaction. Clinical signs of underlying disease that predisposes horses to esophagitis may predominate or mask the signs of esophagitis. Horses with gastrointestinal motility disorders such as anterior enteritis are at high risk for developing reflux esophagitis because of the presence of both gastric acid and bile salts in the fluid reflux. However, signs attributable to esophagitis secondary to ileus may not be noted because of the profound signs caused by the intestinal disorder. Foals with gastric outflow obstructions commonly have reflux esophagitis.
Diagnosis requires endoscopic examination of the esophagus. Diffuse, patchy, linear, or coalescing erosion or ulcerations may be noted. Significant edema or hyperemia may also be observed. It is important to determine whether underlying disease, such as infection, neoplasia, diverticula, or esophageal stricture is present. In addition, the stomach must be examined because reflux esophagitis is commonly accompanied by gastritis or gastric ulcer disease. If endoscopy is not available to detect esophageal ulceration, contrast radiography may be helpful for assessing esophageal motility and transit time.
The principles of therapy for reflux esophagitis include control of gastric acidity and correction of any underlying disorder that is contributing to gastroesophageal reflux. Thus treatment with histamine-2 (H2) receptor antagonists such as ranitidine or proton pump antagonists such as omeprazole is important for resolution of the disease. Some clinicians advocate sucralfate administration to aid healing of esophageal ulcers. However, the efficiency with which sucralfate binds to ulcerated mucosa in the squamous epithelium of the gastrointestinal tract has been questioned because low pH is optimal for the sucralfate polymers to bind ulcerated tissues. It is not clear whether reflux esophagitis provides the right pH environment for binding.
Foals with reflux esophagitis secondary to delayed gastric outflow caused by gastroduodenal ulcer disease or gastric paresis may benefit from prokinetic drugs that act on the proximal gastrointestinal tract. Metoclopramide (0.02 to 0.1 mg/kg SC q4-12h) reduces gastroesophageal reflux by increasing tone in the lower portion of the esophageal sphincter and increasing gastric emptying and gastroduodenal coordination. Metoclopramide should be administered to horses with caution because they are prone to extrapyramidal neurologic side effects. Continuous-rate infusion of metoclopramide (0.04 mg/kg/h) is one way to reduce the risk or severity of neurologic side effects. The rate can be reduced if side effects appear. Cholinergic drugs such as bethanechol (0.025 to 0.035 mg/kg SC q4-24h or 0.035 to 0.045 mg/kg PO q6-8h) may improve gastric emptying and are effective for treating reflux esophagitis. For esophagitis from trauma or pressure injury after esophageal impaction, judicious use of NSAIDs may be warranted to reduce esophageal inflammation and pain.
Dietary modification may be necessary in patients with esophagitis, depending on the degree of ulceration or if motility is impaired. Horses with less severe esophagitis should be fed frequent small meals of moistened pellets and fresh grass. Severe esophagitis may necessitate withholding food and complete esophageal rest for several days. Although the prognosis for esophagitis is good in the absence of underlying disease, the risk of stricture formation is high if severe circumferential or coalescing ulcerations are present. Animals with esophagitis caused by severe trauma or infection also may be prone to stricture formation.
■ Motility Disorders of the Esophagus Esophageal hypomotility is the most common motility dysfunction of the equine esophagus and results in esophageal dilation or megaesophagus. Although megaesophagus in horses is most commonly acquired, there are reports of idiopathic megaesophagus in young horses that is probably congenital (Fig. 32.45 and Color Plate 32. 3).38-43 Congenital megaesophagus appears to be more common in Friesian horses than in other breeds and is associated in some cases with smooth muscle hyertrophuy in the distal esophagus.39,40
Acquired megaesophagus in adult horses is usually caused by either primary or secondary esophageal obstruction. Esophageal impactions of relatively short duration cause proximal dilation of the esophagus that is generally reversible. However, if the duration of the obstruction is long, the motility of the esophagus may be permanently impaired. Acquired megaesophagus in foals is often secondary esophagitis resulting from gastric outlet or duodenal obstruction. Other causes of acquired megaesophagus include extraesophageal obstruction by tumors or abscesses, pleuropneumonia, and vascular ring anomalies. In addition, acquired megaesophagus may result from neurologic,
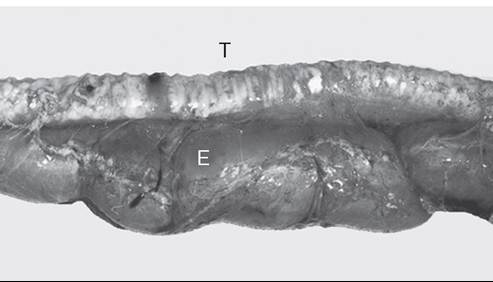
FIG. 32.45 Megaesophagus in a 10-month-old Paint Horse foal that had two duodenal strictures that appeared to have been present for several months. The trachea (T) lies dorsal to the dilated esophagus (E). (Courtesy Dr. MJ. Murray.)
neuromuscular, or muscular disorders. Neurologic diseases that cause vagal neuropathy, such as equine protozoal myeloen- cephalitis, equine herpesvirus myeloencephalitis, and idiopathic vagal neuropathy, have been associated with megaesophagus in horses. Pleuropneumonia may accompany vagal neuropathy and thus result in megaesophagus. Megaesophagus is also an early sign of equine dysautonomia44 and may be noted in patients with botulism. Myasthenia gravis is a well-known cause of megaesophagus in other species but has not been reported in horses. Also in other species, electrolyte disorders, cachexia, primary myopathies, myositis, and Addison disease may affect esophageal motility, but these have not been associated with megaesophagus in horses.
Esophageal inflammation, particularly reflux esophagitis, may affect motility and cause megaesophagus. However, because esophageal hypomotility may predispose to reflux esophagitis, it may be difficult to determine whether the esophagitis or the megaesophagus is the causative disorder (see Color Plate 32.3). Iatrogenic megaesophagus can be induced by the α2- adrenergic agonist detomidine, but this is transient and reversible.45 However, the use of this drug may complicate clinical evaluation of esophageal motility. Because esophageal hypomotility represents a functional obstruction, the clinical signs of esophageal hypomotility or megaesophagus are similar to those of esophageal obstruction. These clinical signs include ptyalism, dysphagia, and nasal discharge of saliva and food material. Dilation of the cervical portion of the esophagus may be evident externally. Weight loss is a common sign, and clinical signs attributable to an underlying disease may be evident.
Diagnosis of esophageal hypomotility requires transit studies. Transit time of a bolus from the cervical portion of the esophagus to the stomach can be measured by fluoroscopy or contrast radiography.7,44 Other signs of esophageal hypomotility and megaesophagus include pooling of contrast material and an absence of peristaltic constrictions. Endoscopy may reveal a dilated esophagus and an absence of peristaltic waves. Evidence of underlying disease causing obstruction or esophageal dilation may be observed. The esophagus should be evaluated for evidence of esophagitis that is either causing esophageal motility dysfunction or is a result of impaired esophageal clearance of gastric fluid. Esophageal manometry may be useful for documenting abnormal postdeglutition contraction pressures, contraction time, and propagation times.4,38 Other diagnostic tests such as a CBC and chemistry studies help identify an underlying cause. A careful neurologic evaluation should be performed. Signs of neurologic disease and abnormal cerebrospinal fluid analysis suggest an underlying neurologic disorder. Myopathy may be detected by electromyography.
Treatment of esophageal hypomotility or megaesophagus should be aimed at the underlying cause. Dietary modification should be aimed at improving esophageal transit of food. Slurries of pellets should be fed. In addition, it may be beneficial to feed from an elevated position to promote transit. In patients with reflux esophagitis associated with megaesophagus, metoclopramide or bethanechol may be beneficial to increase lower esophageal tone, promote gastric emptying, and reduce gastroesophageal reflux. The prognosis depends on the underlying cause and the degree of dilation. Although many cases of megaesophagus associated with reflux esophagitis respond well to treatment, many other forms of megaesophagus, including congenital megaesophagus, have a poor prognosis.
■ Congenital Disorders Congenital disorders of the esophagus are rare. Reported congenital abnormalities include congenital stenosis,46 persistent right aortic arch, congenital strictures, esophageal duplication cysts,47,48 and megaesopha- gus.39,40,49 In the one report on congenital stenosis, doublecontrast radiography revealed concentric narrowing of the thoracic portion of the esophagus in the absence of any vascular abnormalities at the base of the heart. Successful treatment included having the foal stand with the forelimbs elevated off the ground after each feeding.
Persistent right aortic arch is a congenital anomaly in which the right fourth of the aortic arch becomes the definitive aorta instead of the left aortic arch, which results in constriction of the esophagus by the ligamentum arteriosum as it extends between the anomalous right aorta and the left pulmonary artery.24 Clinical signs may include dysphagia, drooling of saliva, and distention of the cervical portion of the esophagus as a result of partial obstruction of the thoracic portion.50 Endoscopic examination typically reveals dilation of the esophagus cranial to the obstruction with evidence of diffuse esophagitis. In addition, evaluation of the thorax usually reveals the presence of aspiration pneumonia. Successful surgical treatment of persistent right aortic arch has been reported in one foal.
Esophageal duplication cysts cause typical signs of esophageal obstruction, including salivation, dysphagia, and swelling of the cervical portion of the esophagus as they enlarge. Such signs can make them difficult to differentiate from simple obstruction (choke). However, an aspirate of the mass may aid in the diagnosis by revealing the presence of keratinized squamous cells.51 Cysts may communicate with the lumen of the esophagus. Surgical treatments have included complete surgical resection and surgical marsupialization. The latter appears to be more successful and to result in fewer complications. Complications of surgical resection have included (1) laryngeal hemiplegia secondary to surgical trauma to the recurrent laryngeal nerve in the region of the esophagus and (2) esophageal fistula formation.
■ Esophageal Perforation Perforation typically occurs in the cervical region in response to external trauma or rupture of an esophageal lesion such as an impacted diverticulum. The esophagus is particularly vulnerable to external trauma in the distal third of the neck because it is covered by only a thin layer of muscle at this location.52 Iatrogenic perforation may occur in response to excessive force with a stomach tube against an obstruction or a compromised region of the esophagus. Esophageal perforations may be open or closed and tend to cause extensive necrosis of tissues surrounding the wound because of drainage of saliva and feed material within fascial planes (Fig. 32.46). This may lead to extensive cellulitis and endotoxemia. Closed perforations of the esophagus are particularly troublesome because wound discharge may migrate all the way to the mediastinum and pleural space via fascial planes and may cause abscessation (Fig. 32.47). In addition, extensive subcutaneous and fascial emphysema frequently develops and is usually evident on cervical radiographs.
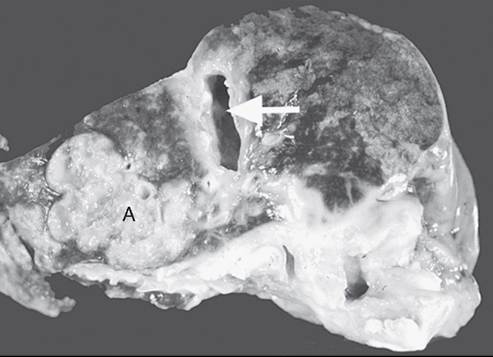
FIG. 32.47 Esophageal abscess (A) and cellulitis that developed secondary to an esophageal obstruction. The esophageal lumen is indicated by the white arrow. (Courtesy Dr. MJ. Murray.)
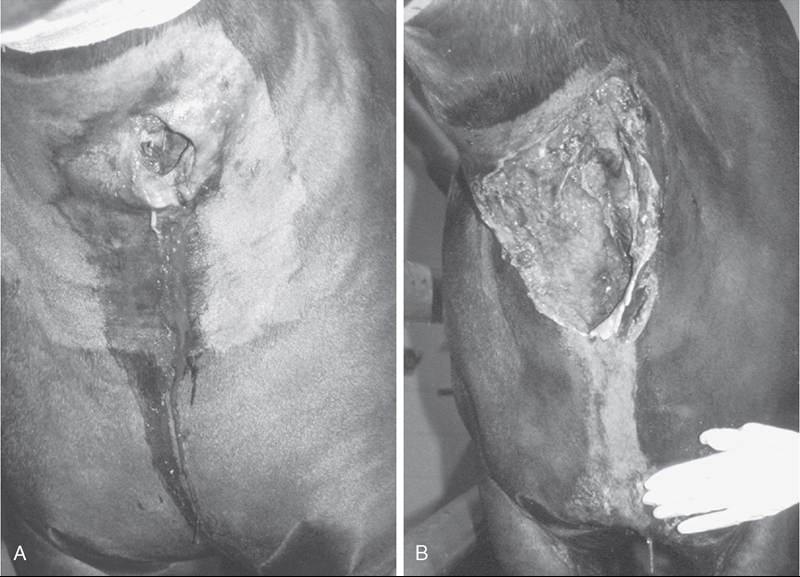
FIG. 32.46 Esophageal perforation in a horse. A, An open esophageal laceration was detected on presentation in the midcervical region. The wound was treated by lavage and debridement, and the horse was fed via a tube inserted into the esophagus through the wound. B, Approximately 14 days later, dissection of esophageal contents within surrounding fascial planes resulted in extensive sloughing of tissue.
Treatment should include conversion of closed perforations to open perforations if possible,53 extensive debridement and lavage of affected tissues, broad-spectrum antibiotics, tetanus prophylaxis, and esophageal rest. The latter may be achieved by placing a feeding tube into the esophagus via the wound. Alternatively, a small (12-French) nasogastric tube should be placed. For open perforations, once the wound has granulated and contracted to a small size, oral feeding may be attempted. Extensive loss of saliva via esophageal wounds may lead to hyponatremia and hypochloremia. In addition, transient metabolic acidosis occurs because of salivary bicarbonate loss, followed by progressive metabolic alkalosis. Although there are reports of esophageal wounds that healed well by second intention, it takes a prolonged period of time.54 In addition, some perforations never completely heal and form permanent esophagocutaneous fistulas that may necessitate surgical correction. The development of esophageal strictures is not common because wounds are usually linear and not circumferential. However, traction diverticula may develop. Other complications of esophageal wounds include Horner syndrome and left laryngeal hemiplegia.
In a retrospective study on esophageal disorders, only 2 of 11 horses with esophageal perforations survived long term,17 and in a report on esophageal trauma secondary to nasogastric intubation, 4 of 5 affected horses were euthanized.35 The prognosis is therefore poor in horses with esophageal perforations, largely because of the extent of cellulitis, tissue necrosis, shock, and local wound complications.
■ Esophageal Stricture Strictures most commonly occur as sequelae to esophageal obstructions that result in circumferential erosion or ulceration of the esophageal mucosa; however, they may result from oral administration of corrosive medicinal agents and trauma to the neck.55 Congenital strictures have also been reported. Strictures that result from mucosal and submucosal trauma are termed esophageal webs or rings. Strictures may also originate in the muscular layers and adventitia of the esophagus (mural strictures) or in all of the layers of the esophagus (annular stenosis).56 Horses with these lesions have a presentation similar to that of horses with simple obstructions because strictures result in partial obstruction and accumulation of feed material in the lumen. Esophageal webs or rings can be observed endoscopically, whereas confirming the presence of mural strictures or annular stenosis may require double-contrast esophagography.

FIG. 32.48 Attempted dilation of esophageal stricture with bougienage. In this case, a cuffed Silastic tube (Dow Corning, Midland, Mich.) was passed to the site of stricture under endoscopic guidance, and the cuff was then inflated to distend the site of stricture. (Courtesy Dr. MJ. Murray.)
In one study on esophageal stricture after simple obstruction, maximal reduction in esophageal lumen occurred within 30 days of esophageal obstruction. Although surgery has been employed to reduce such strictures, initial medical management is warranted because strictures may resolve with conservative therapy, and the esophagus continues to remodel for up to 60 days after ulceration. In one report, seven horses with esophageal obstruction-induced stricture were treated conservatively by being fed a slurry diet and with antiinflammatory and antimicrobial medications; five of seven were clinically normal within 60 days. One of the five successfully treated horses had a 10-cm area of circumferential ulceration, which suggests extensive mucosal injury may resolve without permanent stricture formation.
If strictures do not resolve within 60 days, other methods to increase esophageal diameter should be investigated. Bougienage has been used successfully in small animal patients and human beings and is increasingly used to dilate strictures in horses. The technique involves passage of a tubular dilatable instrument down the esophagus and stretching of the stricture. Some authors have suggested that this may be accomplished by passing a nasogastric tube with an inflatable cuff (Fig. 32.48).57 However, the procedure has to be performed frequently to achieve any success and is often not well tolerated by horses. Alternatively, several surgical techniques have been used to resolve strictures, including resection and anastomosis,58,59 temporary esophagostomy with fenestration of the stricture, esophagomyotomy for strictures of the muscularis layers and adventitia,60,61 and patch grafting with local musculature.62 However, such surgeries are fraught with complications, largely because of the propensity for stricture to recur in the traumatized esophagus. The esophagus lacks a serosal layer and does not rapidly form a fibrin seal, as does the remainder of the intestinal tract, and so anastomoses tend to leak. In addition, tension on the esophagus during swallowing and movement of the neck impairs healing of anastomoses.
■ Esophageal Diverticula There are two types of diverticula: traction (true) diverticula and pulsion (false) diverticula.
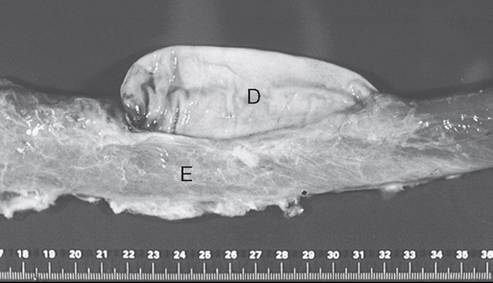
FIG. 32.49 Pulsion diverticulum (D) of the esophagus (E) in a horse that had intermittent episodes of esophageal obstruction. (Courtesy Dr. MJ. Murray.)
Traction diverticula result from wounding and subsequent contraction of periesophageal tissues, with resultant tenting of the wall of the esophagus. Pulsion diverticula arise from protrusion of esophageal mucosa through defects in the muscular wall of the esophagus and usually result from trauma or acute changes in intraluminal pressure (Fig. 32.49). A traction diverticulum appears as a dilation with a broad neck on contrast esophagography, whereas a pulsion diverticulum typically appears as a flask shape with a small neck on an esophagogram.63 Whereas traction diverticula are usually asymptomatic and of little clinical significance, pulsion diverticula may fill with feed material, ultimately leading to esophageal obstruction.64 However, a movable mass in the midcervical region may be noticed before onset of complete obstruction.5 Pulsion diverticula may be surgically corrected by inversion or resection of prolapsed mucosa and closure of the defect in the wall of the esophagus.26,63,64 Inversion of excessive mucosa may predispose horses to esophageal obstruction and should therefore be reserved for small diverticula.
■ Neoplasia Neoplasia of the esophagus is rare, but squamous cell carcinoma65,66 and leiomyosarcoma67 have reportedly affected the esophagus either as the primary site or in association with a lesion in the squamous portion of the stomach. The predominant clinical signs are weight loss, colic, and recurrent esophageal obstruction. The tumor is typically detected on esophagoscopy and radiography during an affected horse's life, but a definitive diagnosis may necessitate a biopsy during laparotomy.21,67 When neoplasia affects the lower portion of the esophageal sphincter, gastroesophageal reflux may contribute to ulceration of esophageal mucosa. The prognosis for malignant neoplasia of the esophagus is grave.