Diseases of Lymph Nodes, Vasculature, and Pharynx
Retropharyngeal Lymph Node Abscessation
John R. Pascoe
■ Definition and Etiology In horses, the retropharyngeal lymph nodes consist of medial and lateral lymphoid chains.
The lateral chain (8 to 15 nodes) is located ventral to the atlas and along the lateral sides of the guttural pouches. These lymph nodes are covered by the parotid gland and are not clearly distinguishable from the medial retropharyngeal lymph nodes (20 to 30 nodes). The medial retropharyngeal lymph nodes are located ventral to the lateral chain on the dorsolateral aspect of the pharynx and the caudoventral aspect of the guttural pouches.1Retropharyngeal lymph node abscesses in horses are generally caused by Streptococcus equi subsp. equi infection (see the Streptococcus equi subsp. equi Infection [Strangles] section earlier) or are secondary to trauma.2,3 Other bacterial isolates have included S. equi subsp. zooepidemicus, Corynebacterium pseudotuberculosis, Actinomyces denticolens, and Actinobacillus spp., including Actinomyces denticolens.4,5 An unusual case of granulomatous infection of the guttural pouch caused by Mycobacterium avium complex was believed to have originated from the retropharyngeal lymph nodes.6 Extension of guttural pouch infections into the retropharyngeal space has been suggested as another source of infection.7 Lymphadenopathy of the retropharyngeal nodes may also occur during viral respiratory infections, including equine herpesvirus (EHV), influenza, and equine viral arteritis.8 Retropharyngeal abscesses not associated with regional lymph nodes can result from perforation of the oropharynx or nasopharynx by ingested foreign bodies,9 passage of a nasogastric tube,10 or use of a balling gun.
In ruminants, the medial retropharyngeal lymph nodes are located on the dorsolateral aspect of the pharynx, one on each side of the midline.
One to three lymph nodes may be present in cattle. The lateral retropharyngeal lymph nodes are located caudal to the medial retropharyngeal lymph nodes in the cranial neck region and are caudal to the retropharyngeal space.11Abscessation of the medial retropharyngeal lymph nodes in cattle may result from pharyngeal actinobacillosis, foreign body penetration, or traumatic perforations by balling guns or dose syringes.12-14 Trueperella pyogenes or Actinobacillus spp. are frequently isolated.8 Cattle with abscessed pharyngeal lymph nodes often have a small ulcer in the mouth, most frequently at the junction of the base and shaft of the tongue. This is more likely to occur when cattle are eating dry scabrous roughage. In addition to traumatic perforations and foreign bodies, caseous lymphadenitis (CLA) caused by C. pseudotuberculosis frequently results in abscessation of the retropharyngeal lymph nodes in sheep and goats.
■ Clinical Signs and Differential Diagnosis Clinical signs associated with retropharyngeal lymph node infection or abscessation in horses include dysphagia, odynophagia (painful swallowing), nasal or oral regurgitation, excess salivation, difficult and often noisy breathing, painful throatlatch swelling, mucoid to mucopurulent nasal discharge, extension of the head and neck, and weight loss. In 46 horses with retropharyngeal lymph node abscessation, common clinical signs were fever and increased heart and respiratory rates (80%), unilateral or bilateral throatlatch swelling (65%), respiratory stertor or distress (35%), purulent nasal discharge (20%), inappetence and signs of depression (15%), and dysphagia (9%).3 Other signs observed endoscopically include decreased cross-sectional area or collapse of the pharyngeal lumen, asymmetry of the dorsal pharyngeal wall, and deviation of the laryngeal aperture away from the retropharyngeal mass.2,3 Differential diagnosis for a retropharyngeal mass should include abscess, cellulitis, guttural pouch empyema or tympany, parotiditis, lymphadenopathy, neoplasia, and hematoma.
Clinical signs observed in cattle with infection or abscessation of the medial retropharyngeal lymph nodes include difficult breathing, excessive salivation, extension of the head and neck, anorexia, enlarged submandibular lymph nodes, nasal discharge, and swelling in the retropharyngeal space.12 Other disease conditions that affect the oropharynx and surrounding lymph nodes should be considered in the differential diagnosis. These include actinobacillosis, lymphosarcoma, sialolithiasis, and necrotic laryngitis, laryngeal edema, or severe tracheitis caused by infectious bovine rhinotracheitis (IBR) virus.8,12
Affected sheep and goats may exhibit excessive salivation, increased respiratory rate, stertorous breathing, mucopurulent nasal discharge, regurgitation, gagging, depression, subcutaneous crepitation, weakness, and fetid breath. A false carotid aneurysm in the retropharyngeal space has been reported; on external examination it may be confused with abscessation of the medial retropharyngeal lymph nodes.15 Enlarged retropharyngeal lymph nodes are usually easily palpated and identified in sheep and goats. CLA (see Chapter 37) is the most frequent cause of enlarged retropharyngeal lymph nodes in these species.
■ Clinical Pathology Collection of purulent material from abscessed lymph nodes may assist in identification of the causal agent. Neutrophilic leukocytosis may be evident on the hemogram.
■ Laboratory Aids and Definitive Diagnostic Tests Lateral radiographs of the pharynx, ultrasonography, and endoscopy facilitate the diagnosis of retropharyngeal infections or abscesses. In horses, radiography may reveal a large soft-tissue mass impinging on the guttural pouch from a caudoventral direction (Fig. 31.40, A), as well as thickening of the pharyngeal roof. The soft-tissue swelling may contain gas (Fig. 31.40, B). Compression of the larynx and trachea with ventral displacement may be evident (Fig. 31.40, C).2 A gas-fluid interface on radiographs of the pharynx generally indicates abscessation, but care should be taken to distinguish a retropharyngeal abscess from guttural pouch empyema.6 Foreign bodies associated with pharyngeal trauma are not typically radiopaque and thus not visible unless outlined by contrast medium.
Exceptions include small wire foreign bodies likely ingested from baled hay that can perforate the tongue or oropharynx and cause cellulitis and dysphagia9 and, in cattle, magnets that have been inadvertently placed retropharyngeally.On endoscopy, asymmetry or collapse of the pharyngeal lumen, or both signs, suggests a retropharyngeal space-occupying mass. Recognition of drainage from the guttural pouch openings or examination of the guttural pouches may be necessary to differentiate between guttural pouch empyema and retropharyngeal lymphadenopathy or pharyngeal neoplasia. Occasionally the pharyngeal wall ruptures, allowing endoscopic observation of retropharyngeal drainage into the pharynx, usually near the esophageal entrance. Percutaneous needle aspiration of the mass may yield purulent material. Ultrasonography improves diagnostic precision by permitting more accurate identification of the abscess and highlighting its anatomic relationships to facilitate surgical drainage.16
Clinical examination, radiography, ultrasonography, endoscopy, and percutaneous centesis may all prove helpful in making a diagnosis of medial retropharyngeal lymph node infection or abscessation in ruminants. In cattle, localized swelling cranial to the larynx may be detected by digital palpation of the oropharynx.12 Oropharyngeal examination must be performed carefully in animals with respiratory distress to prevent further airway compromise.
■ Pathophysiology Upper respiratory tract disease, trauma, and foreign body penetration with resulting infection and drainage to local lymph nodes result in clinically apparent infection and abscessation of the retropharyngeal lymph nodes. In horses, the retropharyngeal space is occupied primarily by the guttural pouches. Because the vagus, glossopharyngeal, hypoglossal, spinal accessory, and sympathetic nerves traverse this area, their function can be affected by infectious or inflammatory processes involving the retropharyngeal space.2 If such
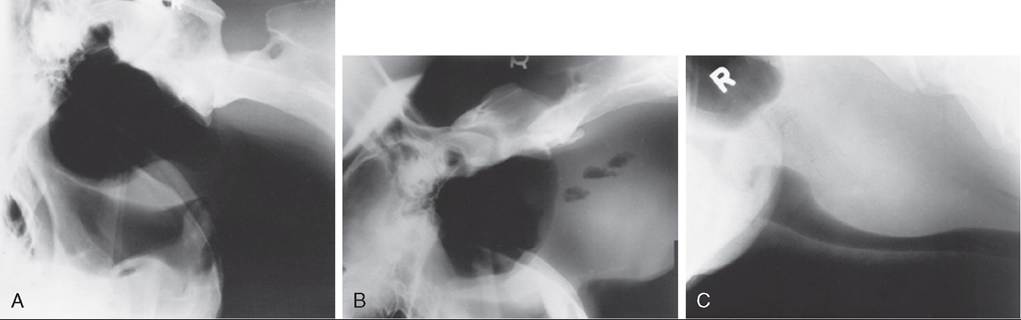
FIG.
31.40 A, Lateral radiograph. A soft-tissue density (retropharyngeal abscess) is distorting the floor of the guttural pouch. B, Lateral radiograph. There is increased soft-tissue density with gas shadows ventral to the cervical vertebrae. These changes are consistent with abscessation of the retropharyngeal lymph nodes. C, Lateral radiograph. There is increased soft-tissue density ventral to the cervical vertebrae, with compression of the dorsal border of the trachea. These changes were caused by cellulitis and abscessation of the retropharyngeal lymph nodes.infections are contained within the lymph nodes or are confined within the fibrous capsule of the abscess, cranial nerve dysfunction is not usually evident.2 Clinical evidence of dysphagia or odynophagia, such as the presence of feed and saliva at the external nares, may result from angina and from inflammation or injury of the glossopharyngeal nerve or pharyngeal branch of the vagus nerve, compression, or obstruction of the pharynx or esophagus. It has been suggested that retropharyngeal lymphadenitis may result in neuritis of the pharyngeal branch of the vagus nerve in young horses and contribute to the pathogenesis of dorsal displacement of the soft palate.17
Respiratory distress may occur when retropharyngeal lymph node enlargement compresses or obstructs the nasopharyngeal, laryngeal, or tracheal lumen, and the disease caused by S. equi subsp. equi in horses is appropriately called strangles.
The most common cause of pharyngeal inflammation and infection in cattle is pharyngeal trauma associated with balling guns, dose syringes, paste wormer guns, esophageal feeders, or nasogastric tubes. A careful history to determine whether any of these devices were used is important in determining the source of pharyngeal abscessation. Such infections usually involve mixed bacterial flora, because the trauma is directly related to the oropharynx.
■ Epidemiology Infection with S. equi usually results from contact (inhalation or ingestion) with pasture, feed, or water contaminated with nasal discharge from infected horses or asymptomatic carriers.18 The likely bacterial reservoir in carrier horses is the guttural pouch, particularly if chondroids are present18-20 or if there are swollen or discharging lymph nodes in the floor of the medial compartment of the guttural pouch.
Infection of the pharyngeal and nasal mucosa results in an acute pharyngitis and rhinitis, and drainage to regional lymph nodes results in lymphadenopathy and possible abscessation.8CLA is spread through discharges from ruptured lymph nodes. The causal agent, C. pseudotuberculosis, may persist in the environment for long periods, and infection results from inhalation or from contact of shearing, docking, or castration wounds with contaminated soil, equipment, or freshly ruptured abscesses. Sheep dips have been reported as another source of infection.8 Spread of infection from skin wounds often leads to involvement of local nodes and abscess formation.
■ Necropsy Findings Fatalities are rare and typically occur from respiratory compromise or septicemia. Necropsy lesions include cellulitis with compression and ventral displacement of the larynx and cranial aspect of the cervical trachea. Abscesses are variable in size and may contain either caseous (C. pseudotuberculosis) or liquid (S. equi subsp. equi) material. A thick, fibrous capsule may occur in response to the infectious process and may account for the surrounding tissue compression. Occasionally, draining tracts may connect the abscess to the pharynx, guttural pouch, or skin.10,21
■ Treatment and Prognosis Treatment goals are relief of respiratory distress and control of infection. Temporary tracheotomy may be needed for relief of respiratory distress and may be prudent, before percutaneous drainage is attempted. After surgical drainage, appropriate systemic antibiotics are administered, and supportive therapy to further reduce swelling may be beneficial.
Surgical approaches include percutaneous drainage, intraoral drainage, and marsupialization.2,12 Percutaneous drainage is commonly used in horses because the long narrow oral cavity makes an intraoral approach very difficult. For abscesses visible through the mucosal lining of the guttural pouch, endoscopically assisted drainage into the pouch can be considered. Surgical access to the retropharyngeal space includes dorsal, ventral, and lateral approaches and access through Viborg's triangle.3 A ventral surgical approach is recommended because of the relative lack of vital structures encountered and because excellent ventral drainage can be achieved. In standing sedated horses, less invasive drainage can be established by ultrasound-guided percutaneous needle placement into abscessed lymph nodes. Affected nodes can have a wall thickness of 1 to 2 cm and a diameter of 5 to 11 cm.16 Aspiration of purulent matter and cavity lavage with antiseptic solutions and concurrent administration of parenteral antibiotics may be sufficient for resolution. If aspiration is not possible because the purulent material is too viscous, incision directly along the needle shaft, after careful consideration of regional anatomy, provides adequate exterior drainage and access for cavity lavage with antiseptic solutions or use of a seton or gauze packing. If the abscess is endoscopically visible beneath the guttural pouch mucosa, drainage into the guttural pouch and subsequent lavage of the purulent material can be accomplished. Before or at the time of abscess drainage or excision, the horse should be started on broadspectrum antimicrobials, followed by the appropriate specific antimicrobial drug when results of microbial susceptibility testing are known.
Occasionally, medical management alone may resolve infection; however, this is less likely if abscessation has occurred. Because the most common bacterial isolate in horses is S. equi, parenteral antimicrobial therapy with procaine penicillin G (22,000 IU∕kg IM twice daily) or potassium penicillin (22,000 IU/kg IV four times daily) is recommended. Systemic NSAIDs are useful to reduce inflammation and swelling, and fluid and electrolyte therapy may be necessary if there is odynophagia or dysphagia. Aspiration pneumonia can occur with dysphagia or if there is oral or nasal regurgitation associated with painful swallowing.
In cattle with pharyngeal trauma, an existing wound is often draining from the retropharyngeal area into the oropharynx, making surgical drainage unnecessary, and response to parenteral broad-spectrum antimicrobial therapy is typically favorable.22 Parenteral antimicrobial therapy alone has been ineffective in treating retropharyngeal abscesses when there is no draining tract.12 Intraoral or percutaneous drainage has been used successfully in conjunction with broad-spectrum, parenteral antimicrobial therapy. After drainage, the abscess cavity is flushed daily with an antiseptic or antibiotic solution12 with the head lowered so that exudate or flush solution is not aspirated; inspection of the granulating abscess cavity is necessary if feed impaction is suspected.2,12 Aspiration pneumonia may be a serious complication when dysphagia is present.
In sheep and goats, walled-off C. pseudotuberculosis abscesses can be safely drained by marsupialization before opening the capsule, which prevents contamination of other retropharyngeal structures and markedly reduces postsurgical cellulitis. Although C. pseudotuberculosis is susceptible in vitro to a number of antimicrobial agents, these abscesses are typically not well controlled by antimicrobial therapy. Walled-off C. pseudotuberculosis abscesses are difficult to eliminate solely with antimicrobial therapy, and drainage or removal of the entire lymph node gives optimal results.
■ Prevention and Control Preventive measures to limit infection and abscessation of retropharyngeal lymph nodes include isolation of horses affected with viral or bacterial upper respiratory tract disease, vaccination against strangles, vigorous treatment in the early stages of streptococcal infection, and correct administration of therapeutic agents with balling guns and dose syringes. Reducing environmental sources of contamination and preventing contamination of shearing equipment, dipping vats, and feeders with C. pseudotuberculosis are important to limiting spread in sheep. Culling affected sheep and goats may also help reduce the incidence of CLA.
Pharyngitis
John R. Pascoe
■ Definition and Etiology Pharyngitis is inflammation of the pharyngeal tissues. It is not generally considered to be a specific disease entity but rather a response to other diseases, particularly viral and bacterial respiratory disease, and to a lesser extent to local physical, chemical, or allergic causes. Acute and chronic forms are recognized.
Although physical and chemical causes of pharyngitis may be identified with certainty, the role and specificity of microbial pathogens as causative agents remain controversial. In horses, Streptococcus spp. and various viral respiratory diseases have been incriminated as specific causes of pharyngitis, but given the ubiquitous nature of some virus groups in horses, a direct causal association remains unsubstantiated.1,2 In cattle, True- perellapyogenes, Actinobacillus spp., and Fusobacterium necrophorum are frequently isolated.3
Synonyms for chronic pharyngitis in horses include pharyngeal lymphoid hyperplasia (PLH), chronic pharyngitis, chronic lymphoid follicular hyperplasia, follicular pharyngitis, and follikelkatarrh.4-6
■ Clinical Signs and Differential Diagnosis In acute pharyngitis, signs are associated with pharyngeal pain (odynophagia, dysphagia), nasal discharge (serous, seromucous, mucopurulent, purulent, feed-contaminated), regional lymphadenopathy (submandibular, retropharyngeal nodes), ptyalism (especially in cattle), respiratory noise (often inspiratory), pharyngeal swelling, and cough. Mouth breathing may occur in cattle when there is increased resistance to breathing associated with excessive exudate, diphtherous membranes, and lymphadenopathy. Pharyngitis from local pharyngeal trauma or incarcerated foreign bodies may be associated with odor of nasal discharge or the breath. Cattle with necrotic laryngitis, pharyngitis, and stomatitis have a characteristic malodorous breath. Acute laryngeal inflammation and edema of unknown cause can occur in horses and ruminants and is characterized by marked inspiratory difficulty and stertor without malodorous breath. Treatment of acute edema with dexamethasone (0.05 mg/kg IM; avoid in pregnant heifers or cows) and broad-spectrum antimicrobials has produced rapid clinical improvement.
Signs observed on endoscopic or oropharyngeal examination in cattle include pharyngeal hyperemia and edema, lympho- nodular swelling, and either a moist appearance of the pharyngeal surface or the presence of exudate or a diphtherous membrane adhering to the pharyngeal surface. Focal necrosis or ulceration of the mucous membrane and tonsillar tissue may occur; signs associated with rhinitis and laryngitis may be evident. Signs of chronic pharyngitis are similar. In horses, there may be endoscopic evidence of more marked hyperplasia of the lymphonodular follicles within the pharyngeal mucosa, and single or multiple lymphonodular masses may be within, or protrude from, the pharyngeal mucosa. Biopsy and cytologic evaluation are recommended to rule out neoplasia, particularly squamous cell carcinoma, lymphoma, and lymphosarcoma. Differential diagnostic possibilities include rhinitis and laryngitis, and in cattle, rabies should be strongly considered before oropharyngeal examination. If the predominant sign is dysphagia (see Chapter 7), other diagnostic rule-outs include foreign bodies in the tongue, fractures of the hyoid apparatus or jaws, and in the horse, diseases of the guttural pouches. If exercise intolerance is the primary complaint in a horse, pharyngitis should be considered only after other possible causes of impaired performance have been eliminated (see Chapter 5).7-11 Pharyngitis is not a risk factor for poor racing performance in racing Thoroughbreds12 or Standardbred trotters.10 More severe PLH grades were found in poorly performing endurance horses (primarily Arabian horses); however, more definitive causes for poor performance were identified in these horses.11
Upper airway inspiratory pressures recorded during strenuous exercise in horses with grade IV PLH are not different from those of normal horses under the same exercise conditions.8 Assuming that airflow in both groups of horses was comparable, severe PLH does not appear to cause functional upper airway obstruction. It is conceivable that pharyngeal pain associated with PLH may contribute to impaired performance; however, this effect remains unproven.
■ Clinical Pathology Changes in the hemogram and serum biochemical profiles are likely to result from concurrent respiratory disease (increases or decreases in absolute or differential leukocyte counts, hyperfibrinogenemia, anemia) or to reflect abscess formation (neutrophilia, hyperfibrinogenemia) or dehydration and fasting associated with dysphagia. Electrolyte losses associated with drooling may alter serum electrolyte and acid-base status.
■ Laboratory Aids and Definitive Diagnostic Tests Although a presumptive diagnosis can be made from clinical signs, definitive diagnosis requires observation of the pharynx (Fig. 31.41) and, more important, exclusion of other conditions that have similar signs. Radiography of the pharynx can provide information on pharyngeal anatomy, radiodense foreign bodies, soft-tissue masses, fractures, and in horses, guttural pouch disorders. Ultrasonography of the pharyngeal region and, if indicated by the clinical examination, both radiographic and ultrasonographic examination of the thorax may help define the extent of concurrent pulmonary disease.
Microbial culture of pharyngeal secretions can be considered, but interpretation is difficult because (1) the pharynx normally has resident microflora with considerable individual variation, and (2) many of the microorganisms isolated are capable of opportunistic infection. In horses with grades III and IV PLH, the number of bacteria recovered per gram of pharyngeal secretion was almost 100-fold greater than in normal horses.9 The pattern of microbial isolation was not consistent among horses, suggesting that these organisms were not the source of the pharyngitis but rather that other factors had made conditions for colonization more favorable.
Biopsy and cytologic examination are indicated in refractory cases and when abnormal masses are present to rule out neoplasia.
■ Pathophysiology Acute pharyngitis occurs as a sequela to inflammation of regional lymphoid tissue (see Kumar and colleagues13 for a description of the morphologic and histochemical features of the normal equine nasopharyngeal tonsil).14 In horses, the pharyngeal tonsil consists of discrete lymphoid follicles diffusely distributed in the dorsal and lateral walls of the pharynx. In ruminants, the pharyngeal tonsil is located caudal to the pharyngeal septum in the caudodorsal wall of the pharynx and is bounded by long ridges and grooves into which mucous glands open. In response to local or lymphogenous spread of infection, the tonsillar tissue becomes inflamed and the tonsillar crypts become filled with desquamated epithelium, leukocytes, and bacteria. Clinically this is seen as hyperemia and edema of the pharyngeal tonsil with diffuse

FIG. 31.41 Endoscopic view showing the nodular appearance of pharyngeal lymphoid hyperplasia.
white or yellow tips to the lymph nodules. The edematous appearance is associated with hyperplasia of the lymph nodules and sequestration of perinodular inflammatory fluid.
If extensive destruction of the lymphoid cells or subsequent invasion of the nodules or supporting soft tissue is evident, the result is focal or diffuse necrosis, which may be seen as pinpoint areas of follicular necrosis or diffuse necrosis with associated purulent or fibrinonecrotic exudate. With resolution, atrophy of some follicles and increased fibrosis are present. Follicular atrophy also occurs with aging.
■ Epidemiology No specific epidemiologic data are available. When pharyngitis occurs as a sequela to respiratory tract infection, the population demographics should be similar to those known for the specific respiratory disease. For example, grade II PLH was identified in 60% of foals with distal respiratory tract infection and in only 13% of control foals.15 Because physical and chemical injury to the pharynx occurs sporadically, no universal epidemiologic characteristics would be anticipated.
PLH is prevalent in horses younger than 5 or 6 years of age, and the severity of PLH grades5 is inversely correlated with age.4,12,16,17 In endoscopic surveys of primarily Thoroughbreds in race training, prevalence of PLH ranges from 29% to 34%, with grade II PLH observed in 45% to 63% of 2-year-olds and less than 12% to 20% of horses older than 5 years affected.16 Similar results are reported from Japan in racing Thoroughbreds with a history of cough or abnormal respiratory noise18 and in a mixed population of horses in Calgary, Canada.17 Pharyngeal mucus scores are not correlated with PLH, transtracheal wash aspirate, or BAL fluid variables, suggesting that PLH is not directly a manifestation of lower
y
1719
airway inflammation or disease.1,19
■ Treatment and Prognosis Approach to treatment is largely symptomatic and directed at palliation of pharyngeal pain and maintenance of unobstructed breathing until the initiating disease process has abated. In many instances, the signs are sufficiently mild that treatment is unnecessary. When pharyngeal angina is causing inappetence or dysphagia, administration of NSAIDs should be considered. Dehydration should be corrected by either parenteral or enteral fluid administration. Enteral fluid therapy may be difficult because passage of a nasogastric tube may elicit too much pain. For inappetent animals, nutritional support may be necessary until pharyngeal pain subsides sufficiently for normal eating to resume. Soft feeds, especially green grass, should be offered when available to encourage animals with pharyngeal discomfort to eat.
Antimicrobial therapy is probably not indicated, but it is often given to limit development of secondary bacterial infection. Infections caused by foreign body injury should be treated with antibiotics that have a broad aerobic and anaerobic spectrum of activity. Daily lavage of any cavitary wounds, debridement, and removal of feed material may be necessary to prevent additional abscess formation and hasten healing.
Custom topical preparations, usually containing an antibiotic, an antiinflammatory drug, and a hygroscopic agent (glycerin) or DMSO, are often used for palliation of clinical signs, especially in horses with PLH. These preparations are usually administered two or three times daily and sprayed onto the pharyngeal surface through a transnasal catheter. Despite frequent use, the efficacy of this therapy is unknown, and response may reflect natural resolution of the predisposing cause.
Treatment of PLH is empirical and generally palliative. Rest from training for 4 to 8 weeks is commonly recommended, and although some horses have recurrence when training resumes, this enforced rest is beneficial as convalescence for any concurrent subclinical respiratory disease. Horses kept
in training are often initially treated empirically with sulfa compounds and topical throat preparations. With continued clinical signs, penicillin or broad-spectrum antibiotics are often administered. If PLH does not improve or resolve after therapy, pharyngeal cautery may be used. Techniques for pharyngeal cautery include topical application of trichloroacetic acid, electrocautery, freezing with liquid nitrogen or Freon, and photoablation by neodymium:yttrium aluminum garnet (Nd:YAG) laser with either a contact or a noncontact technique.20 Although cauterization techniques have received considerable testimonial support, it is likely that cautery does not effect a cure but simply obliterates reactive tissue so that it is no longer clinically evident.
Routine immunization for known viral respiratory pathogens is also recommended for treatment and prevention of PLH.21
■ Prevention and Control Methods used to control and prevent most of the common viral and bacterial respiratory diseases (see Chapter 48 for vaccines) should limit herd problems with acute pharyngitis. Non-respiratory disease-related causes such as trauma from balling guns, nasogastric tubes and dose syringes, foreign objects, and chemical burns can be minimized by improved husbandry practices.
Prevention of PLH in horses by prophylactic immunization against common equine viral respiratory agents at regular intervals has been discussed at length, but there is no evidence to support this practice. Nevertheless, racetrack veterinarians maintain that frequent immunization (60-day intervals) against influenza and rhinopneumonitis markedly reduces the severity of PLH and improves exercise tolerance.21 Considering the mobility of racing and show horse populations, this approach should at least be beneficial for limiting outbreaks of viral respiratory disease and consequently perhaps limiting chronic PLH. Until more is understood about the clinical appearance of the pharyngeal tonsil in horses, along with normal variations that occur with aging in exercised and nonexercised horses, and these findings can be correlated with immunopathologic events and indices of performance, it will remain difficult to treat, control, and prevent pharyngitis in a systematic manner.