Guttural Pouch Diseases
John R. Pascoe
■ Definition and Etiology The guttural pouches are paired, air-filled diverticula of the eustachian tubes that communicate between the middle ear and the pharynx.
Located ventral to the atlas, dorsocaudal to the pharynx, and rostrodorsal to the retropharyngeal lymph nodes, they occupy a large part of the retropharyngeal space. Each pouch has a capacity of approximately 300 mL and is divided into medial and lateral compartments by a stylohyoid bone that courses through the caudolateral aspect of each pouch. The larger medial compartment accounts for approximately two thirds of the volume, and they appose each other on the midline, separated by a membranous septum. The medial compartment contains cranial nerves IX (glossopharyngeal), X (vagus), XI (spinal accessory), and XII (hypoglossal); the cranial cervical ganglion; and the cervical sympathetic trunk. The internal carotid artery lies deep to the caudolateral wall of the medial compartment. The pharyngeal branch of the vagus nerve and the cranial laryngeal nerve are immediately ventral to the floor of the medial compartment. In the lateral compartment, the facial nerve (VII) is located caudodorsally, and the external carotid artery and its branches, notably the maxillary artery, are associated with the roof of the lateral compartment.1 The intimate relationship of these vessels and nerves with the mucous membrane lining the guttural pouches explains why epistaxis and nerve dysfunction frequently accompany guttural pouch disease. Communication with the pharynx occurs through a slit-like opening rostral and ventral to the pharyngeal recess. This funnel-shaped pharyngeal opening is wider rostrally than caudally. A mucous membrane fold within the pouch, the plica salpingopharyngea, contributes to the caudal narrowing of the opening and makes catheterization of the guttural pouch difficult. Redundancy of this tissue fold may contribute to guttural pouch tympany.1Lined with pseudostratified ciliated epithelium containing goblet cells,2 the guttural pouch is an extension of the pharynx and is not a sterile environment. In 30 normal horses, 59% of percutaneous guttural pouch lavage aspirates had bacterial growth, although only 7% had bacteria considered to be pathogenic; no fungi were isolated.3 Aspirates were considered normal if they had less than 5% neutrophils; typical cell distribution was primarily ciliated columnar epithelial cells, a few nonciliated cuboidal epithelial cells, and less than 1% monocytes, lymphocytes, and macrophages.3 Inflammatory cell counts and altered cell distribution were correlated with recovery of bacteria. Horses exercised strenuously on a regular basis had lower total cell counts, lower neutrophil counts, and fewer bacteria isolated.3 Preventing horses from head lowering for 12 to 24 hours increases the frequency of bacterial isolation, especially at 24 hours, including an increase in neutrophil counts, likely indicating a reduced ability to clear guttural pouch secretions.4 Interpretation of microbial isolates from guttural pouches requires correlation with cytologic characteristics of guttural pouch fluid and clinical signs.5
Three disease conditions commonly affect the guttural pouches: tympanitis, empyema, and mycosis. Less common conditions include neoplasia,6 fractures of the hyoid bone, temporohyoid osteoarthropathy, foreign bodies,1 and cystic structures.7
Guttural Pouch Tympany
Tympany of the guttural pouch occurs infrequently. It can be recognized in foals from birth to 1.5 years of age8-10; affected foals are usually identified within the first 2 weeks of life. Fillies are more commonly affected, with the ratio of females to males ranging from 2: 1 to 4: 1. Familial and complex inheritance of guttural pouch tympany occurs in Arabian horses and German Warmblood horses, and sex-specific quantitative trait loci have been identified.11
Tympany is characterized by unilateral or bilateral distention of the guttural pouch with air.
The exact cause is unknown, but congenital redundancy of the plica salpingopharyngea has been suggested. This mucosal fold acts as a one-way valve apparently permitting airflow into but not out of the pouch. Upper airway infection or inflammation has been postulated to result in enlargement of the fold or neuromuscular dysfunction contributing to air trapping.■ Clinical Signs and Differential Diagnosis Affected foals usually have a nonpainful, soft, fluctuant swelling in the retropharyngeal space (Fig. 31.42, A) with variable respiratory distress, extension of the head and neck, nasal discharge, signs of dysphagia, and possible development of aspiration pneu- monia.8,9 Guttural pouch fluid accumulation and empyema can occur. Mild tympany may not result in signs other than swelling of the throatlatch (retropharyngeal) region. Respiratory distress occurs when continued distention of the pouch compresses the pharyngeal area. The differential diagnosis for throatlatch regional swelling should include guttural pouch empyema and retropharyngeal abscesses or cellulitis.
■ Clinical Pathology Stress leukocytosis may occur if there is marked respiratory distress.
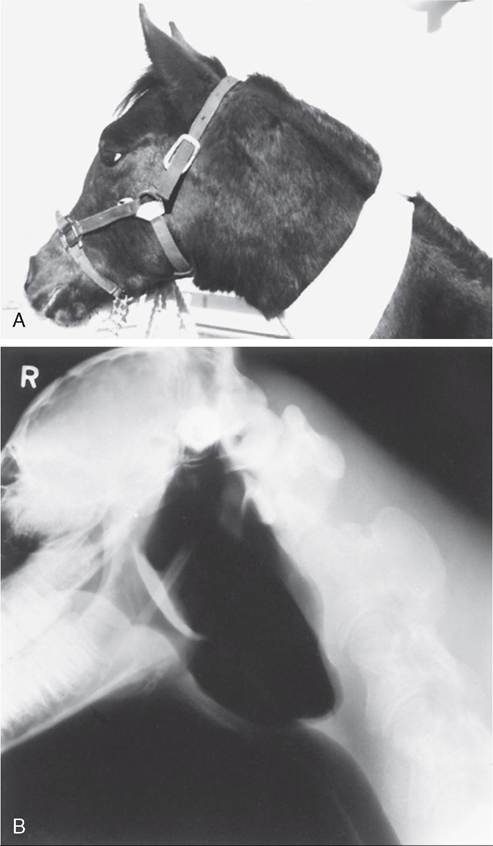
FIG. 31.42 A, Foal with guttural pouch tympany. Note the protrusion of the soft tissues over the lateral and ventral aspects of the throatlatch. B, Lateral radiograph of a foal with tympanitis of both guttural pouches.
■ DiagnosticAids Diagnosis of guttural pouch tympany is based on recognition of characteristic swelling in the retropharyngeal space and confirmation by clinical examination. Although distention is most often unilateral, extreme distortion of a single pouch may give the impression of bilateral involvement. Differentiation between unilateral and bilateral involvement can be difficult and may require deflation of the affected guttural pouch by catheterization or percutaneous needle aspiration combined with external compression.
Other adjunctive diagnostic procedures include radiographic demonstration of gas distention of one or both pouches (Fig. 31.42, B) and endoscopic observation of pouch distention and pharyngeal distortion.■ Treatment and Prognosis Guttural pouch tympany and respiratory distress can be alleviated temporarily by aspiration of air from the affected pouch by percutaneous decompression at the point of greatest distention through Viborg's triangle or by introduction of a catheter through the pharyngeal opening of the guttural pouch. These measures are palliative, and the pouch rapidly refills after decompression. Treatment methods include surgical excision of the plica salpingopharyngea and part of the medial lamina of the eustachian tube; partial resection or photoablation of the plica; fenestration of the median septum between the two pouches by excision, electrosurgery, or photoablation; or creation of a salpingopharyngeal fistula by photoablation and temporary stenting of the fistula.8-10,12-15 The latter technique is similar to an older, successful approach that involved incising the floor of the guttural pouch into the pharynx. If the condition is bilateral, fenestration of the median septum alone is usually insufficient, and excision of one or both plica salpingopharyngea, in combination with septal fenestration or septal fenestration and salpingopharyngeal fistula formation, must be performed. After surgery the prognosis for resolution of guttural pouch tympany is generally favorable10 unless complicating factors such as aspiration pneumonia exist.9 Early recurrence after surgery can range from 15% to 30%, but further resection of the plica salpingopharyngea or refenestration of the median septum or enlargement of the fenestration 9 10
typically results in resolution of signs.9,10
Guttural Pouch Empyema

FIG.
31.43 Lateral radiograph demonstrating distinct fluid lines in both guttural pouches.(Fig. 31.43) or radiodense masses (chondroids) within the pouch on standing lateral radiographs supports a diagnosis of empyema. Physical and endoscopic examination or oblique radiographic projections may be needed to identify which pouch is involved. Endoscopic examination permits identification of the affected pouch and evaluation of the character of the fluid. Endoscopic examination of the lateral compartment is important to avoid missing sequestered fluid or chondroids.23 Absence of fluid at the pharyngeal ostium does not preclude the possibility of guttural pouch empyema, as the fluid may be inspissated or the ostium may be sealed.24 Fluid identified on radiographs should be characterized by endoscopic examination of the pouches or aspiration of the fluid with cytologic and microbial analysis. Fluid samples can be aspirated through the pharyngeal ostium using a sterile artificial insemination pipette, Chambers catheter, or tubing advanced through the biopsy channel of an endoscope. Alternately, fluid can be aspirated percutaneously but should be performed cautiously to minimize the likelihood of bacterial contamination along the needle tract and development of cellulitis.
■ Pathophysiology Guttural pouch empyema may result from extension of the upper respiratory tract infection with S. equi subsp. equi (strangles) to the guttural pouches or from rupture of retropharyngeal lymph node abscesses into the guttural pouch.17 Commonly isolated bacteria from guttural pouch empyema include S. equi subsp. equi, S. equi subsp. zooepidemicus, E. coli, and Klebsiella spp.22 Not all horses with empyema have a history of strangles or previous respiratory infection, and empyema seemingly can occur by many of the same mechanisms as middle ear infection; that is, fluid accumulates in the area, and uncontrolled growth of bacteria normally present results in inflammation and exudation.
■ Treatment and Prognosis Treatment of guttural pouch empyema is complicated by poor drainage from the affected pouch. The pharyngeal opening of the guttural pouch is located rostrodorsal to the floor of the guttural pouch, and drainage can be achieved only by lowering the horse's head; however, adequate drainage may not occur if there is ventral distortion of the pouch. Inflammation of the lining mucosa may result in swelling of the tissue surrounding the pharyngeal opening, further compromising normal drainage.
Treatment approach depends on the duration and nature of the empyema and the presence of chondroids. Parenteral antimicrobial therapy may reduce the quantity of the nasal discharge, but relapse often occurs after treatment stops.22 The early stages of empyema may respond to daily lavage of the affected guttural pouch. Because of the thin nature of the mucosal lining and the proximity of cranial nerves VII and IX to XII and the cranial sympathetic trunk, it is important to use nonirritating solutions (e.g., physiologic or saline antibiotic solutions) to avoid neural inflammation or neuritis. Large volumes have caused guttural pouch rupture. Typically, 500 mL should be flushed into the pouch under moderate pressure to create contact with as much of the interior of the guttural pouch as possible. During lavage the head should be lowered to prevent aspiration of fluid and facilitate drainage. Purulent fluid from the affected guttural pouch should be aspirated on initial catheterization and submitted for microbial culture and antimicrobial susceptibility testing. Fluid collection can be accomplished with most flexible uterine culturettes under direct endoscopic observation. Parenteral antimicrobial drugs should be administered on the basis of susceptibility testing results. Streptococcal isolates may be resistant to potentiated sulfonamides and sulfadimethoxine.22 Although medication may be of benefit in treating empyema, adequate drainage and local therapy are of primary therapeutic importance.
Indwelling catheters in normal guttural pouches cause increasing purulent discharge over time, which diminishes after catheter removal and is typically resolved within 3 days. Although indwelling catheters are convenient, daily catheterization and irrigation using an artificial insemination pipette or Chambers catheter should be considered when treating an already inflamed guttural pouch to diminish the inflammatory response associated with indwelling catheters. However, daily catheterization must be weighed against the stress, possible tissue trauma, and time requirements for intermittent catheterization.
Treatment with parenteral antimicrobials and local lavage is successful and requires a patent opening for adequate drainage, but the course of treatment may be protracted. Povidone-iodine (1% available iodine) diluted to a 10% solution (0.1% available iodine) for lavage of the guttural pouch caused considerable reaction, including inflammatory infiltrates, hemorrhage, necrosis, and lymphoid reaction.25 Likewise, antimicrobial concentrations of chlorhexidine gluconate are not recommended.26 Although acetylcysteine, a mucolytic, has been used to resolve inspissated empyema,27 subsequent reports have shown lack of efficacy and concern for added mucosal inflammation.28 If response to lavage is poor or if secretions reaccumulate and empyema returns, surgical drainage of the guttural pouch should be considered.
Surgery is generally indicated when purulent material becomes inspissated or chondroids have formed,29 although resolution was reported in one horse after prolonged lavage (14 days) through an indwelling catheter.30 Surgical approaches include percutaneous drainage through standard approaches to the guttural pouches in anesthetized recumbent or standing sedated horses and creation of a nasopharyngeal fistula by use of an Nd:YAG laser.31 Other approaches when chondroids are present include removal by retrieval devices passed endoscopically, standing removal through a modified Whitehouse approach,32 and removal from the contralateral pouch after fenestration of the median septum when the ipsilateral ostium is closed.24
The prognosis for guttural pouch empyema is generally favorable if it is recognized promptly and treated appropri- ately.22 Likewise, removal of chondroids typically has a good prognosis.22
Guttural Pouch Mycosis
Guttural pouch mycosis is a fungal disease of the guttural pouch that typically affects the dorsocaudal region of the medial compartment, although lesions affecting larger areas, including the lateral compartment, occur.33-35 Fungal invasion of neurovascular structures coursing through the walls of the guttural pouches results in clinically apparent disease. The exact cause is unknown, although a number of fungi, especially Aspergillus (Emericella) nidulans and Aspergillus fumigatus, have been isolated from lesions.35-39
■ Clinical Signs and Differential Diagnosis Lesions are usually unilateral but can occur bilaterally. The wide spectrum of clinical signs that can occur with guttural pouch mycosis reflects the degree of fungal invasion and subsequent inflammation of vascular structures or nerves beneath the mucous membrane lining the guttural pouch; however, the size of the lesion is not correlated with the severity of clinical signs. Intermittent spontaneous epistaxis and dysphagia are the common clinical signs that stimulate owners to seek veterinary care; however, the earliest clinical sign in most affected horses is nasal discharge (serous to mucopurulent).40 Epistaxis generally results from fungal erosion of the wall of the internal carotid artery in the roof of the medial compartment and less commonly from erosion of the external carotid artery (or its branches; e.g., caudal auricular artery) and maxillary artery in the lateral compartment. Epistaxis is usually unilateral from the ipsilateral nostril, but it can be bilateral because the pharyngeal openings of the guttural pouches are located caudal to the caudal border of the nasal septum.34 Episodes of epistaxis typically occur at rest and vary from mild to severe, with several premonitory bleeds that generally culminate in a fatal episode of epistaxis.34,35 Occasionally a horse dies from a single episode of epistaxis without previous clinical signs. Epistaxis may recur at intervals varying from 24 hours to 3 weeks.34
Dysphagia, the second most common clinical sign, likely results from damage to the pharyngeal branches of the vagus and glossopharyngeal nerves and generally occurs later than epistaxis in the course of the disease.34 Horses with dysphagia cough during attempts to eat solid food, and in addition to food material in the nasal discharge, a considerable quantity of food is coughed from the mouth. Recovery from dysphagia may occur,34 but in general the prognosis for full recovery is poor.
Other clinical signs include parotid pain, abnormal head posture, unilateral or bilateral nasal discharge, head shyness, abnormal respiratory noise from pharyngeal paralysis or laryngeal hemiplegia, sweating and shivering, Horner's syndrome, visual disturbances, colic, and facial paralysis.34,35 These signs are the result of angina and dysfunction of cranial nerves and the sympathetic nerves.
The differential diagnosis for a horse with epistaxis should include EIPH, ethmoid hematoma, guttural pouch or pharyngeal neoplasia, tracheobronchial foreign bodies, and guttural pouch mycosis.34 Differentiation of these diseases is aided by a thorough history and endoscopic examination. Differential diagnosis for dysphagia should include fractures of the hyoid apparatus; pharyngeal and guttural pouch fistula; cleft palate; esophagitis; pharyngeal paralysis; foreign body entrapment in the mouth or esophagus; pharyngeal neoplasia; lead poisoning; bacterial, viral, and mycotic central nervous system infections; and guttural pouch mycosis.34
■ Clinical Pathology If epistaxis is the presenting complaint, moderate to severe anemia with accompanying hypoproteinemia may also be present. Differential white cell distributions may be normal or may indicate a stress response. If dysphagia becomes a dominant clinical sign, other hematologic changes indicative of infection secondary to aspiration pneumonia may be evident.
■ Diagnostic Aids Clinical signs of epistaxis or cranial nerve dysfunction are suggestive of a diagnosis of guttural pouch mycosis. A thorough physical examination may reveal abnormal sensitivity on digital palpation of the parotid area on the affected side.33 A definitive diagnosis of guttural pouch mycosis requires endoscopic observation of the characteristic diphtheritic lesion in the dorsocaudal aspect of the medial compartment, typically covering over the temporohyoid joint and internal carotid artery, or elsewhere within the guttural pouch.34 Aneurysm of the internal carotid artery is rarely present. A healed lesion may be identified by presence of scar tissue within the mucous membrane.34 Lesions vary in color (brown, yellow, black, or white) and size (from discrete nodules to diffuse irregular patches covering the roof of both the medial and the lateral compartments)35; erosion with fistula formation can occur into the opposite guttural pouch or pharynx. Occasionally the characteristic lesion is obscured by clotted blood, so that the diagnosis is based on the clinical signs of epistaxis correlated with blood present in the guttural pouch. Because hemorrhage may originate from the internal carotid, external carotid, or maxillary arteries, it is important to identify the source of bleeding before therapy, particularly if surgical intervention is being considered. Care should be taken not to dislodge a thrombus and produce further hemorrhage. If dysphagia is apparent, food and saliva may be identified during endoscopy of the pharynx and nasal passages.
In guttural pouch mycotic infections, radiographs are of limited value because only minimum suppuration is associated with mycotic infections; however, a lateral projection may allow assessment of the degree of fibrous reaction and loss of normal air space. Radiography may also aid in diagnosing some of the long-term sequelae, such as fibrous deposits in the pouch and associated bony changes.
Serum titers to A. fumigatus are not diagnostic; however, reactivity to 22-kd and 26-kd serum antigens measured by immunoblot analysis may be diagnostic for guttural pouch mycosis.37
■ Pathophysiology The pathogenesis and predisposing factors leading to guttural pouch mycosis and arterial erosion are unknown, but it is believed that the disease is initiated by some stress (inflammation, trauma, vascular insult) to the soft tissues where the mycotic plaques are generally found.35 Aneurysm formation is not well correlated with the severity of the plaque formation. Although the nature of the initiating lesion remains unclear, it is generally agreed that the later stages are associated with deep fungal infections.37 Fungal plaques have been induced experimentally after systemic and topical (guttural pouch) corticosteroid administration within 2 days of pouch inoculation with A. fumigatus; however, lesions resolved spontaneously within 15 to 28 days without apparent vascular or nerve involvement or induction of clinical signs.38 A. nidulans and other Aspergillus spp. have been isolated and may be the causative agents35-41; A. nidulans is rarely pathogenic but may grow as an opportunist in the warm, humid environment of the guttural pouch.35 The mycotic lesions show no predilection for either the right or the left guttural pouch.34 Fungal infection of the pouch, erosion of major blood vessels, and involvement of nerves (IX, X, XI, XII, cranial cervical ganglion, and postganglionic sympathetic fibers) that traverse the area account for the epistaxis, local pain, and neurologic signs associated with guttural pouch mycosis.34,35
■ Epidemiology No apparent age, sex, breed, or geographic predispositions have been observed. Guttural pouch mycosis is a sporadic disease that tends to arise during the warmer months of the year and rarely affects more than one horse in a particular stable.34 Affected horses are afebrile; infection is diagnosed when clinical signs such as epistaxis and dysphagia occur, although nasal discharge is often the earliest reported sign.34
■ Necropsy Findings Lesions are confined to the pharyngeal muscles, guttural pouch, and bones of the skull.33 Gross findings may include large blood clots in the nasal passages and at the pharyngeal opening of the guttural pouch. Unilateral denervation atrophy of the ipsilateral pharyngeal or laryngeal muscles may occur if there is involvement of the pharyngeal and recurrent laryngeal branches of the vagus nerve.33 Examination of the guttural pouch generally reveals clotted blood and a diphtheritic plaque in the dorsocaudal aspect of the medial compartment that is firmly adherent to the underlying tissue and is clearly demarcated from surrounding tissue.35 The lesion may be localized or may affect the entire roof of the pouch. If hemorrhage has occurred, the lesion may be obscured by clotted blood, pus, or mucus.35 An intense inflammatory reaction may be evident in response to acute fungal infection, whereas the inflammation may subside with chronic healing lesions so that scar tissue is evident.35 Active inflammation may also predispose to osseous lesions of the petrous temporal and stylohyoid bones.33,35 Some cases of guttural pouch mycosis may not have associated clinical signs and may be diagnosed only on necropsy.34
■ Treatment and Prognosis Without treatment a poor prognosis is warranted because affected horses are at risk for a fatal episode of epistaxis. Both medical and surgical treatments have been recommended, with variable results; however, surgical treatment by an intraarterial occlusion technique is generally considered to yield the best prognosis.42-44 Although apparently uncommon, spontaneous regression of guttural pouch mycosis can occur and must be considered when the various medical or surgical treatments are being evaluated.34
Medical treatment is topical therapy of the mycotic lesion through the pharyngeal opening of the guttural pouch by means of a catheter. Bathing the lesion in medication may be facilitated by anesthetizing the horse and positioning it in dorsal recumbency. Instilling fungicidal and fungistatic drugs, topical enzymes, and organic iodine compounds into the guttural pouch has been attempted with variable success.45,46 The necessity and efficacy of these treatments are unknown, and systematic treatment is hampered by a lack of knowledge of the pathogenesis of guttural pouch mycosis.47 Parenteral administration of antibiotics, corticosteroids, thiabendazole, ketoconazole, and iodine compounds also has questionable efficacy.47 The response of guttural pouch mycosis to local and parenteral treatment is protracted; thus the risk of fatal hemorrhage exists 48 49 long after initiating treatment.,
Surgical treatment of guttural pouch mycosis appears to offer the best prognosis for eventual cure. The internal carotid artery is not an end-artery, and blood can enter this vessel from the bifurcation of the common carotid or return from the cerebral arterial circle. Various surgical techniques have been described,50 and use of a balloon-tipped catheter inserted into the distal internal carotid artery combined with proximal ligation of the internal carotid artery,48-51 transarterial coil 435253 54
embolization,43,, or transarterial nitinol vascular plugs54 induces thrombus formation and prevents hemorrhage from normal and retrograde blood flow. Thrombosis sufficient to prevent hemorrhage may develop in the distal internal carotid artery within 10 days of catheter placement.51 Mucosal healing and complete regression of the fungal plaque have been reported to occur as early as 5 weeks after arterial catheterization49 and as early as 15 days after coil embolization.43 Insertion of a balloon-tipped catheter successfully prevented fatal epistaxis in 13 horses.48 Topical or systemic treatment of the mycotic plaque is considered unnecessary after arterial catheterization.48 Intraarterial insertion of latex balloons, embolization coils, or nitinol vascular plugs also results in lesion resolution,54-57 although progression of a mycotic plaque after coil embolization and subsequent development of neurologic signs have been reported.58 Complications associated with each of these arterial occlusion techniques have been reported.59