Equine Thoracic Neoplasia
Fabio Del Piero • Pamela A. Wilkins
Surveys of equine neoplasms indicate a low prevalence of thoracic neoplasia in the horse. In an abattoir survey in London of 1308 horses, only 2 horses had pulmonary tumors: one granular cell tumor and one bronchiolar adenoma.1 Two other necropsy surveys of 155 and 687 equines reported no thoracic neoplasms.2,3 A report on chronic pulmonary disease in the horse states that the practical importance of lung tumors in this species is negligible.4 University of Pennsylvania researchers examined 5629 horses between 1968 and 1987.
Thirty-five horses had neoplasia involving the thoracic cavity, corresponding to a prevalence of 0.62%.5The prevalence of primary lung neoplasms of any type is reported to be less than 1% of all reported neoplasms in domestic animals.6 The lungs are susceptible to tumor emboli because of the filter action of the capillary bed associated with small capillary diameter and, perhaps, specific adhesion factors. It can sometimes be difficult or even impossible to distinguish metastatic disease from primary pulmonary neoplasia; thus an important part of the diagnosis is exclusion of possible primary sites elsewhere in the body. Primary pulmonary tumors reported in the horse include granular cell tumor, bronchial myxoma, adenoma, adenocarcinoma, anaplastic bronchogenic carcinoma, and pulmonary carcinoma (Fig. 31.39). Other primary thoracic tumors reported in the horse include pulmonary chondrosarcoma, pleural mesothelioma, thymoma, and lymphosarcoma. The majority of these neoplasms generally occurs in the mature or aged horse. The exception is lymphosarcoma, which may also be observed in young animals.
Antemortem diagnosis of thoracic neoplasia depends first on recognition of thoracic disease. Most of the reported cases of thoracic neoplasia involve metastatic disease.
The horses' clinical signs are generally related to the primary site of the neoplasm; therefore the clinician often has no reason to suspect thoracic involvement. When respiratory signs such as dyspnea, tachypnea, hemoptysis, cough, cyanosis, nasal discharge, and epistaxis are present, relevant diagnostic tests are more likely to be performed. Ultrasonography and bronchoscopy increase the frequency of antemortem diagnosis of thoracic neoplasia.Granular cell tumors are the most frequently reported primary pulmonary neoplasm of the horse. They are usually confined to the lungs and are characterized by single to multiple well-defined, whitish, dense nodules associated with a major bronchus, often protruding into the bronchial lumen or more distally within the parenchyma. Most granular cell tumors have been diagnosed only at postmortem examination, often as incidental findings. These homogeneous growths of granular eosinophilic cells express S-100 and occasionally neuron-specific enolase.7 The ultrastructural morphology of this tumor may suggest a neural origin as well. Primary pulmonary chondrosarcoma has been reported in the horse.8 Cytologic examination of pleural fluid and antemortem needle aspirate of the pulmonary mass revealed neoplastic chondrocytes. Another report describes metastatic chondrosarcoma in the lungs of a horse with a primary tumor in a rib.9 A primary bronchial myxoma, characterized by loose spindloid mesenchymal cells, was reported in a 25-year-old Arabian mare with a history of intermittent coughing, hyperpnea, and respiratory disease of 2 years' duration.10
Primary pleural tumors are also rare. The type reported in the horse is pleural mesothelioma. The tumor is frequently associated with a large volume of pleural effusion. Cytologic examination of the pleural effusion revealing numerous pleomorphic mesothelial cells may aid in the antemortem diagnosis.
Thymomas are neoplasms of thymic epithelial cells, regardless of the presence or absence of lymphocytes.
They are infrequently reported in the horse.11-13 Equine lymphosarcoma occurs in mediastinal, alimentary, multicentric, cutaneous, and generalized forms; combinations of one or more of these are not infrequent.14,15 In a 1973 review of 54 cases of equine lymphosarcoma,3 the lung was involved in 16.6% of the cases, whereas the thoracic lymph nodes were involved in 35.2%.16 In the University of Pennsylvania survey, lymphosarcoma was the single most common neoplasia of the thorax and was present in 19 (54%) of the cases.3 Pleural fluid cytologic evaluation was diagnostic in six (75%) of the eight horses. Diagnosis was made by biopsy of a peripheral lymph node in several cases. In a report from the University of Bristol, thoracic malignant lymphoma accounted for 74% of the cases of thoracic neoplasia.16 Metastatic adenocarcinoma accounted for 20% of the cases in the University of Pennsylvania study5 and 11% of the cases in the University of Bristol study.16 The primary sites of the tumor were thought to be kidney, uterus, thyroid, and ovary.Gastric squamous cell carcinomas commonly metastasize to the thoracic cavity. Cytology of pleural fluid with identification of neoplastic epithelial squamous cells has allowed for antemortem diagnosis of the carcinoma in several cases. Metastatic squamous cell carcinoma of the thorax was found in 14% and 5% of the cases in the University of Pennsylvania5 and University of Bristol16 surveys, respectively. Neoplastic epithelial cells may also be identified in biopsy specimens via indirect immunohistochemistry using antibodies recognizing cytokeratins of various molecular weights.
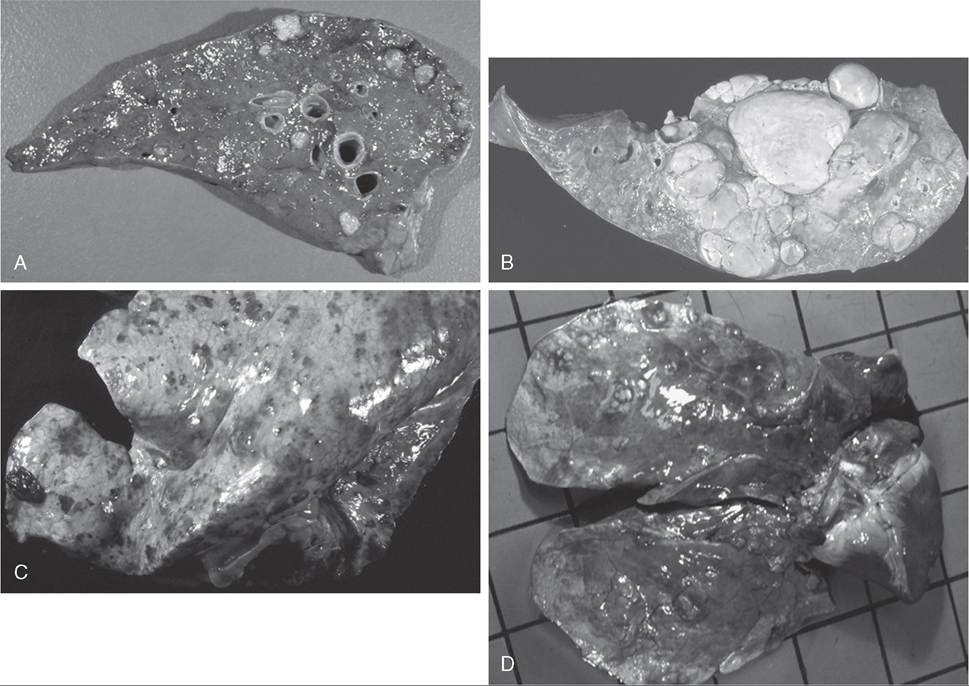
FIG. 31.39 A, Metastatic undifferentiated sarcoma. B, Granulosa cell tumor. C, Metastatic hemangiosarcoma. D, Metastatic squamous cell carcinoma.
Hemangiosarcoma with pulmonary involvement was found in 9% of the horses in the University of Pennsylvania survey.5 Hemothorax, anemia, and dyspnea were commonly seen with this type of neoplasm. Tentative antemortem diagnosis of the hemangiosarcoma can be made by transcutaneous direct thoracoscopy and observation of hemorrhages over the visceral and parietal pleural surfaces as well as tissue biopsy of these sites. Identification of neoplastic endothelial cells demarcating irregular, sometimes blood-filled cavities allows diagnosis from the biopsy specimen.
Malignant melanoma in a 20-year-old gelding had widespread infiltration of many organs, including the lungs and pleura.16 This pattern of distribution is not uncommon in malignant, less pigmented melanomas. Amelanotic melanomas are rare in the horse, and microscopic identification of melanin simplifies the diagnosis of these tumors. Equine melanocytes express S-100 and PNL2 proteins, and their detection can be used to diagnose melanocytic neoplasms.
Other pulmonary metastatic tumors reported are mammary carcinoma,17 seminoma,18 and malignant pheochromocytoma.19 Pulmonary hamartomas are occasionally observed in the newborn foal. Although they are nonneoplastic growths, they appear as tumorlike masses that can compress the surrounding parenchyma and cause systemic passive congestion and hydrops of the amnion in the fetus. Their histologic characterization is that of bronchiolar-like structures lined by cuboidal epithelium with lack of alveolar development or by normal alveoli, bronchi, and blood vessels but with an alveolus/artery ratio greater than normal. Generally they are not compatible with a long period of extrauterine life.
An unusual progressive idiopathic multifocal granulomatous pneumonia of adult horses may resemble neoplasia behaviorally and morphologically during clinical examination.20,21 Pulmonary biopsy may allow the identification of equine multinodular pulmonary fibrosis (EMPF), which has been associated with EHV-5 infection21 (see Figs. 31.29 and 31.30).
Clinical signs of thoracic neoplasia are often inapparent or nonspecific—for example, depression, inappetence, weight loss, and pyrexia. More specific signs include cough, epistaxis, and dyspnea. Cytologic examination of tracheobronchial aspirate, BAL fluid, or pleural fluid and histologic examination of a thoracic mass tissue biopsy with ancillary histochemistry and indirect immunohistochemistry may allow for antemortem diagnosis of the neoplasm. Occasionally, electron microscopy may provide additional information. In equine patients with respiratory signs, all causes of infectious or allergic lung disease should be eliminated before neoplasia is considered in the differential diagnosis.