Diseases of the Paranasal Sinuses
Sinusitis
John R. Pascoe
■ Definition and Etiology Sinusitis, inflammation of the paranasal sinuses, results from primary microbial infection or from secondary bacterial infection associated with dental or other sinus disease.
Lined by respiratory mucosa, the paranasal sinuses are at risk for developing diseases affecting the respiratory tract. Sinus empyema, accumulation of pus within a sinus cavity, may result from bacterial or viral infection.Incidence of sinusitis is relatively low, likely less than 0.5% of disease in equine practice.1 In two longitudinal retrospective studies, covering 25 years, of 477 horses referred with sinonasal disease, the distribution of causes was primary sinusitis (subacute or chronic; 33%), dental-associated sinusitis (21%), sinus cysts (13%), sinonasal neoplasia (7%), ethmoid hematoma (6%), sinonasal trauma (6%), mycotic lesions (4%), dental-related oromaxillary fistula (3%), and miscellaneous causes (6%).2,3 The caudal maxillary, rostral maxillary, ventral conchal, and conchofrontal sinuses are more commonly involved, and the sphenopalatine sinus is affected less often.4 The median age of horses affected with sinonasal disease is 7 to 11 years.2
Acute or chronic upper respiratory tract infections of viral or bacterial origin can result in primary sinusitis; Streptococcus spp. infection is the most common. Maxillary sinusitis caused by disease of the third (caudal roots) through sixth cheek teeth (modified Triadian numbers 109 to 111, 209 to 211) often results from alveolar periostitis, patent infundibula, fractured or split teeth, or deep diastemata between caudal maxillary teeth. Dental defects can permit access of food material or bacteria to the tooth root and sinus cavity, with extension to the frontal sinus likely through the frontomaxillary opening.
Reported neoplasms include osteoma, osteosarcoma, adenocarcinoma, lymphosarcoma, squamous cell carcinoma, neuroendocrine tumors or neuroblastoma, fibroma, and chondrosarcoma.5-7■ Clinical Signs and Differential Diagnosis Signs vary depending on cause, location, and extent of sinus involvement, with unilateral nasal discharge (serous, mucoid, mucopurulent, purulent) being the most frequent sign.2,3 Physical examination of a horse with sinusitis should include observation for epiphora, facial asymmetry, altered nasal airflow, abnormal breath odor, mandibular lymphadenopathy, and sinocutaneous fistula.
Nasal discharge is typically unilateral because the nasomaxillary opening is located rostral to the caudal edge of the nasal septum. Intermittent or continuous nasal discharge need not be related to a previous upper respiratory tract infection. Although malodorous discharge is commonly associated with dental sinusitis and sinonasal mycosis, it has been reported to occur in 14% to 27% of primary sinusitis cases.2,3 Mucopurulent discharge is more commonly associated with sinus cysts.2 Sanguineous discharge is common with ethmoid hematoma and sinonasal trauma; however, guttural pouch mycosis, pulmonary hemorrhage, nasal turbinate necrosis, and neoplastic or granulomatous lesions should also be considered. Other differential diagnoses of nasal discharge should include guttural pouch empyema or mycosis, acute pharyngitis (strangles, rhinopneumonitis, influenza, trauma), neoplasia or necrosis of the turbinates, ethmoid hematoma, and pulmonary disease.
After nasal discharge, submandibular lymphadenopathy is the most common sign, particularly when microbial infection is a component of sinusitis.3 Facial swelling occurs with frequency similar to that of lymphadenopathy, typically when sinus drainage is obstructed, there is an expansile mass within the sinus, or as an acute sign after facial trauma. Occasionally exophthalmos can occur with marked sinus distortion.
Patency of the nasomaxillary opening generally precludes facial distortion. Loss of patency occurs when inspissated exudate accumulates or mucosal lining tissue reaction obstructs the opening. Expansion of the sinus may result in reduced ipsilateral nasal airflow caused by distortion of the architecture of the nasal passages. In these cases abnormal respiratory noise rather than nasal discharge may be the primary presenting sign.
Epiphora occurs if there is nasolacrimal duct involvement from trauma, compression, or destruction of the duct associated with sinus disease. Approximately 20% to 50% of horses with dental sinusitis, sinus cyst, or sinonasal trauma have epiphora as a presenting sign.2,3
Percussion of the affected sinus may reveal dullness or pain, although normal resonance does not preclude the possibility of sinusitis. If there is bone thinning over gas above a fluid line (as can occur with some maxillary sinus cysts), percussion may elicit increased resonance.
Careful examination of the oral cavity for signs of dental or periodontal disease should be performed when any of these signs are present. Particular attention should be paid to examination of the occlusal surface of the teeth with a very fine dental pick (e.g., 22-gauge needle); however, it should be recognized that periapical abscess formation can occur without defects in the occlusal surface. Accuracy of diagnosis of dental disease is substantially enhanced by use of intraoral endoscopy and computed tomography (CT).
■ Clinical Pathology The hemogram generally remains within the normal range, although acute sinusitis of infectious origin may be associated with neutrophilia with or without hyperfibrinogenemia. With chronic sinusitis, there may be concurrent hyperfibrinogenemia and hyperglobulinemia. Sinus fluid obtained by percutaneous centesis should be examined cytologically (including a Gram stain) and submitted for microbial culture and susceptibility testing to differentiate among bacterial, fungal, and neoplastic disease.
Flecks of feed material indicate sinusitis secondary to dental abnormalities.■ Laboratory Aids and Definitive Diagnostic Tests A presumptive diagnosis of sinusitis can be made from the physical examination and associated clinical signs.2,3,8 Procedures most helpful in establishing a diagnosis are sinonasal endoscopy, oral cavity examination, imaging (radiography, CT, scintigraphy, magnetic resonance imaging [MRI]), sinus centesis, and sinoscopy.4,8,9
Nasal cavity endoscopy may permit identification of exudate draining from the nasomaxillary opening or, in advanced cases, may reveal distortion of the nasal cavity secondary to sinus enlargement. Middle meatus examination is an important component of endoscopic examination. Diagnosis beyond recognition of the potential source of the nasal discharge is limited unless an obvious mass or abnormal tissue is observed. Sinoscopy can be accomplished by using an arthroscope10 or flexible endoscope11 inserted through small trephine holes in either the maxillary or the frontal sinus.9 Examination of the rostral compartment of the maxillary sinus requires a separate portal unless the bony septum between the rostral and caudal compartments has been destroyed. Observation may be limited by fluid or tissue, especially in the rostral compartment of the maxillary sinus, but can potentially be enhanced after sinus lavage and aspiration. Alternately, fenestration of the ventral conchal bulla can be used to facilitate endoscopy of the rostral compartment of the maxillary sinus.4
Standard radiographic projections include standing lateral, dorsoventral, and right and left oblique views.12,13 Radiographic findings include fluid lines within the sinus, space-occupying soft-tissue densities, areas of decreased bone density, fractures, or dental abnormalities. Dental root disease is identified radiographically by a loss of continuity of the lamina dura and lysis of the tooth root or surrounding bone, combined with new bone formation and cement deposition.12 Anatomy of normal equine skulls as demonstrated by CT and MRI has been described.14-18 Diagnostic accuracy, especially determination of the extent of involvement of structures within the skull, can be enhanced by CT.19,20 MRI may be useful in some sinonasal disorders.21,22
Findings associated with dental caries include hypoattenuation of cementum, destruction of enamel, and filling of the infundibular cavity with gas, whereas with dental decay there is gas accumulation in the root area or fragmentation of the root and sinus mucosal thickening.
Additional changes with sinusitis typically involve the maxilla with endosteal sclerosis, thickening, periosteal reaction, and deformation, especially involving the facial crest.20 Scintigraphic examination may improve specificity in identifying dental involvement in sinusitis.23,24Percutaneous sinus centesis may provide a definitive diagnosis and allow an avenue for subsequent therapy. Cytologic evaluation, with concurrent microbial culture and antibiotic susceptibility testing, may elucidate the cause of the sinusitis. Isolation of a single organism such as Streptococcus spp. generally indicates a primary sinusitis, whereas polymicrobial infection is more compatible with sinusitis of dental origin. Visual examination of the oral cavity, especially intraoral endoscopy, and careful probing of the occlusal surfaces with a dental pick may help identify dental abnormalities.
■ Necropsy Findings Affected sinuses contain fluid or tissue of variable color and consistency. Fluid character ranges from clear and odorless with cystic sinus disease to white, yellow, or green purulent fluid with a variable but often putrid odor in sinusitis resulting from other causes. Sinusitis of dental origin has a characteristically pungent and unpleasant odor. Granulomatous lesions often appear as large, lobular, gelatinous masses filling the sinus cavity. The gross appearance of neoplastic lesions within the sinus cavity depends on the type of neoplasm. Neoplasia may cause surrounding soft-tissue and bony destruction, whereas large, benign space-occupying lesions may result in distortion of the nasal turbinates and nasal septum, as well as visible facial bone distortion.
■ Treatment and Prognosis Not infrequently, horses with a chronic mucopurulent nasal discharge from sinusitis have a history of response to antimicrobial therapy, followed by recurrence of the discharge after antibiotic therapy ceases. Definitive diagnosis of sinusitis can be accomplished using the techniques described earlier.
Sinoscopy permits examination of the paranasal sinuses and in some instances facilitates treatment.25,26Suggested treatment for primary sinusitis or empyema involves daily lavage of the sinus through a percutaneous centesis site with 1 L of saline, to which a broad-spectrum antibiotic or antiseptic has been added. Once the results of microbial culture and susceptibility testing are available, the appropriate antibiotic should be administered locally in the flush solution, as well as systemically, for 14 days. Resolution or reduction in the volume of nasal discharge is an indication of successful therapy. Sinus lavage often fails to remove inspissated material, which is often the nidus for continuing sinusitis and must be removed for resolution.8 If little progress is made after 10 to 14 days of lavage or if drainage recurs, sinusotomy (trephination or bone flap technique, standing or recumbent anesthetized) is recommended to remove inspissated material22 or identify other causes. The prognosis is generally favorable if primary sinusitis is not chronic and if the mucous membrane is not markedly thickened.26,27 Chronic sinus disease (longer than 6 months) carries a poor prognosis, and for resolution to occur, surgical removal of the thickened, infected mucous membrane is required; creation of sinonasal drainage by sinus fenestration is also recommended.
Sinusitis that results from secondary factors is generally not responsive to medical management. Such conditions include diseased teeth, granulomas, or neoplasia; surgical removal of the inciting cause is required, and adjunctive treatment may be required. The prognosis for sinusitis associated with dental abnormalities is usually favorable once the diseased tooth has been removed.26,27 Complications are lower with oral extraction than with repulsion of diseased teeth.27 Generally, failure of oral extraction and subsequent tooth or tooth fragment repulsion results in lower morbidity than initial repulsion.27 If the periodontal ligament is intact, endodontic therapy can be used to save the tooth. This is accomplished by surgical apicoectomy and retrograde occlusion of the root canal after debridement of the pulp. In geriatric horses with dental-associated sinusitis, when economic constraints limit surgical options, sinusotomy and periodic sinus lavage and antibiotic therapy have been used successfully to manage nasal discharge.
The prognosis for resolution of granulomatous lesions is generally guarded and depends on surgical access and extent of the lesion. Neoplastic lesions are often well established and have metastasized, either locally or regionally, by the time they become clinically apparent; the prognosis for resolution is generally guarded to poor.4
■ Prevention and Control Prevention of sinusitis in horses is difficult because of the variety of causes. Isolation of horses from those with upper respiratory bacterial or viral diseases may be of benefit in preventing primary sinusitis. Regular dental care and a proper diet may help circumvent sinusitis caused by dental abnormalities, although many cases most likely result from a variety of causes not yet defined or over which the owner or veterinarian has no control.
Ethmoid Hematoma
John R. Pascoe
■ Definition and Etiology Ethmoid hematomas (progressive ethmoidal hematoma1; hemorrhagic nasal polyps2) are slowly expanding angiomatous masses (median dimensions: 3.8 ? 9 ? 13 cm)3 originating principally from the mucosal lining of the ethmoid conchae. Smaller hemangiomas arising from the mucosal lining of the frontal, maxillary, and sphenopalatine sinuses have been recognized, but the relationship between these benign endothelial tumors and ethmoid hematoma remains uncertain. Ethmoid hematoma is a relatively uncommon condition of unknown cause. Distinctly different histologic features characterize ethmoid hematoma and paranasal sinus cysts,4 which makes it unlikely that these lesions are variants of each other with a common cause.5 Although ethmoid hematomas have been reported in a 4-week-old foal and in 3-year-old horses, most affected horses are older than 8 years and are generally Thoroughbred, Arabian, or warmblood horses6,7; males (geldings) seem to be more commonly affected.3
■ Clinical Signs A blood-tinged nasal discharge with intermittent epistaxis from one or both nostrils is the most common clinical sign. Unilateral or bilateral epistaxis varies from blood-tinged, mucoid, or mucopurulent discharge to blood spots or a trickle of blood. Fulminant or fatal epistaxis is uncommon. If the hematoma occupies the choanae or nasal cavity, a mucopurulent, occasionally malodorous nasal discharge with some blood discoloration is more commonly seen. Typically there is a history of abnormal respiratory noise, both inspiratory and expiratory, especially during exercise. With nasal cavity involvement, airflow may be reduced or absent on the affected side. Facial distortion or asymmetry is uncommon and more likely to occur with involvement of the frontal and maxillary sinuses. Secondary mycotic infections and empyema may be associated with intraparanasal sinus ethmoid hematoma.8 Less commonly there may be an associated history of coughing, choking, ptyalism, increased respiratory effort during resting breathing, and either head shyness or headshaking.1 If the hematoma has expanded into the paranasal sinuses, percussion yields a dull sound.
■ Laboratory Aids and Definitive Diagnostic Tests Confirmation requires endoscopy of the ethmoid conchae and diagnostic imaging (Fig. 31.44). Although survey radiography is useful to identify the mass, its origin and extent are delineated more accurately with CT, which is also more reliable
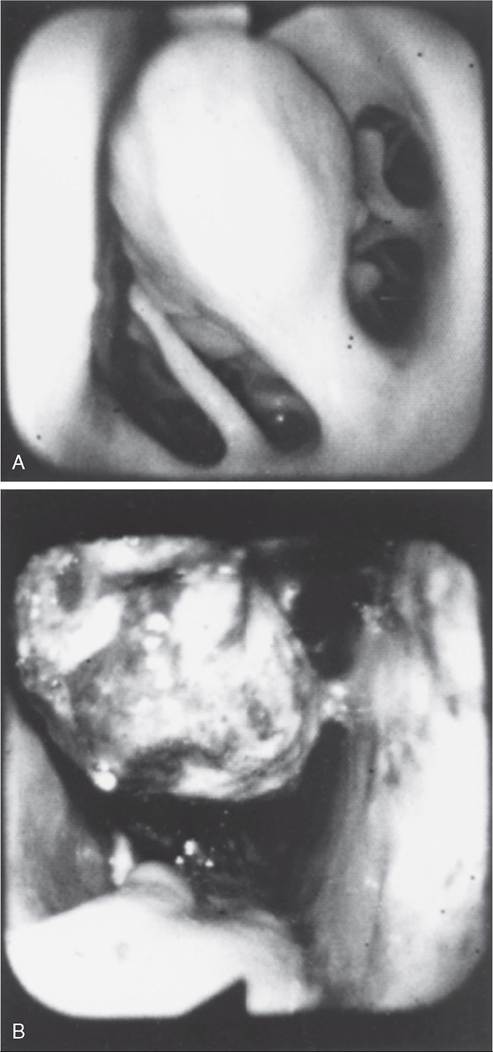
FIG. 31.44 Endoscopic view of left ethmoturbinate. A, Normal appearance. B, Ethmoturbinate obscured by an ethmoid hematoma.
than a combination of clinical examination, endoscopy, and conventional radiography.3 Limited information is available to assess the value of MRI for diagnosis of ethmoid hematoma.9,10 In the absence of CT, sinoscopy may be of diagnostic value when the ethmoid hematoma involves the paranasal sinuses without nasal cavity protrusion. Rarely, ethmoid hematoma infiltrates the nasal conchae; these lesions, identifiable by CT, may be missed on sinoscopy. Definitive localization of ethmoid hematoma involving the sphenopalatine sinus is unlikely by radiography or sinoscopy.3
Ethmoid hematomas are bilateral in 30% to 50% of affected horses, so it is prudent to examine both ethmoidal conchae. The ethmoidal labyrinth is visible approximately 25 cm from the nares, with the endoscope positioned in the ventral nasal meatus and the viewing tip deflected dorsally. The rostral surface of the ethmoidal concha does not protrude beyond the caudal aspect of the nasal cavity; it has a bulbous shape and a moist pink to pale red mucosal covering. Distal to the rostral surface are numerous pillars that form the ethmoidal conchae and separate the ethmoidal spaces (cellulae ethmoidales). Ethmoid hematomas that project into the ventral meatus or through the choana into the nasopharynx often obscure the ethmoidal concha. Unilateral ethmoid hematomas that expand into the nasopharynx may extend into the contralateral ventral meatus and obscure that ethmoidal labyrinth.
The origin of hematomas that expand dorsally into the frontal sinus may not be visible on endoscopy, but hemorrhage that originates deep to the visible portion of the ethmoidal conchae may be evident or noticed from the region of the nasomaxillary opening in the middle meatus. Visible ethmoid hematomas vary in color from deep red to red-purple or may have a yellow-brown or yellow-green-brown to bronze color. The surface is irregularly rounded, with small punctate hemorrhages or erosions, and may be partially covered in yellow-white mucopurulent material that may be admixed with blood. Often the floor of the ventral meatus and regions of contact with the nasal cavity have pooled exudate (blood and mucopurulent matter). Manipulation of the hematoma surface with the endoscope may cause bleeding or oozing.
Radiographic recognition of a discrete, often smooth-surfaced homogeneous radiodensity originating from the ethmoidal conchae and extending into the frontal, maxillary, or sphenopalatine sinuses, or into the pharynx or nasal cavity, is suggestive of ethmoid hematoma. Precise definition of the hematoma origin is difficult to determine from radiographic projections, and small hematomas contained within the ethmoid labyrinth may not be visible.
CT examination allows more accurate assessment of the origin of the ethmoid hematoma,3 allows determination of the extent of involvement of the paranasal sinuses (especially the sphenopalatine sinus) and conchae, and facilitates surgical planning. On CT scans, masses are often associated with bone destruction, especially of the ethmoturbinates and infraorbital canal, and typically abut the cribriform plate in 50% of cases. Masses commonly have mild to moderate signal heterogeneity and a hyperdense swirling appearance consistent with recent hemorrhage or mineralization, which are also common morphologic features.3
■ Necropsy Findings Morphologic features have been described from surgical specimens, but few skulls with intact ethmoid hematomas have been examined.2,3 Except in regions with necrosis or secondary infection associated with contact with the sinus or nasal cavity walls, the hematoma is a smoothsurfaced saclike structure containing blood in various stages of organization. The sac lining is generally healthy respiratory mucosa originating from a pedunculated region of the mucosal covering of the ethmoturbinate or sinus wall. On section, contents are amorphous red-black to chocolate brown, and in larger masses some evidence of irregular compartmentalization by fibrous tissue exists, especially on the inner surface of the sac.
Morphologic features include an outer covering of respiratory epithelium (flattened columnar or cuboidal ciliated epitheliumcontaining glands, and occasionally stratified squamous epithelium4) overlying an irregular zone of submucosal fibrous tissue, containing hemosiderophages, occasional plasma cells, and lymphocytes, less commonly neutrophils, that forms a pseudocapsule around hemorrhage in varying states of organization. There is variable organization of the fibrous tissue components. Endothelial cells do not show evidence of neoplasia. Thin endothelium-lined sinuses are often present within the myxomatous stroma. The respiratory epithelium is sometimes focally ulcerated and infiltrated with neutrophils, and occasionally there are squamous metaplastic changes. Ethmoid adenocarcinoma with a similar gross appearance to ethmoid hematoma has been reported.3,11
■ Treatment and Prognosis Ethmoid hematomas slowly and progressively increase in size and can cause skull distortion if there is paranasal sinus involvement, so removal is recommended. Treatment method depends on location and size. Surgical ablation has been the preferred method; however, destruction of the hematoma by intralesional injection of formaldehyde solution is associated with less morbidity, although recurrence rates are similar to those achieved by other methods.6-8,12,13 Surgical access is achieved by sinusotomy and then hematoma ablation by curettage, cryosurgery, or use of an Nd:YAG laser13; photoablation can be achieved through the biopsy channel of an endoscope. If sinusotomy is necessary, the pedunculated origin of the hematoma is identified by digital palpation and then dissected, frozen, or photoablated, and the hematoma is removed. If the hematoma is friable, intact removal may not be possible, and hemorrhage may make observation of the origin of the mass difficult. After removal, the paranasal sinuses and nasal cavity are packed with gauze to control postoperative hemorrhage.
Surgical curettage can be associated with marked intraoperative blood loss typically from the turbinates or sinus mucosa rather than the hematoma. Temporary occlusion of both carotid arteries14 can reduce blood loss until the sinus cavity is packed with gauze. Blood loss is minimized with cryosurgical extirpation and photoablation techniques, but these approaches are not always practical with large hematomas. Although blood loss is minimal with transnasal photoablation, this technique requires multiple procedures to destroy large masses but can be performed in the standing sedated horse. Photoablation (Nd:YAG laser, 100 W in noncontact technique) is effective in controlling remnants after surgical extirpation or subsequent regrowth.15 A complication of severe epistaxis, subarachnoid hemorrhage and peracute, severe neurologic signs that occurred during laser photoablation of an ethmoid hematoma in the right nasal cavity have been reported in one horse.16
Destruction of ethmoid hematomas by endoscopically guided intralesional injection of formalin in standing sedated horses may reduce the need for surgical ablation.12,17 A catheter passed through the endoscope biopsy channel is advanced through the rostral surface of the mass toward its origin, then 10% formalin (4% formaldehyde solution) is injected intralesionally. Commercially available catheters with a beveled needle tip are available, but relatively stiff plastic tubing that slides through the biopsy channel will penetrate the hematoma capsule. Sufficient volume (10 to 100 mL) is injected until fluid leaks back alongside the catheter or from the mass. For visibly pedunculated masses, formalin should be injected at the origin or neck of the mass. Tissue necrosis and slough occur within 5 to 10 days and may be associated with nasal discharge. Repeat injections, typically at no longer than 10- to 14-day intervals, may be needed to destroy the mass. Removal of necrotic tissue can be facilitated by use of long, grasping forceps and hydropulsion. Mycotic plaques may cover the treated site during healing but typically resolve without treatment; endoscopically delivered topical natamycin has been used if mycotic plaque is extensive and associated with malodorous, purulent discharge.18 If the hematoma has a paranasal sinus extension, necrosis of that tissue within the sinus, after destruction of the ethmoturbinate origin of the hematoma, may result in sinus empyema, mycotic infection, or both,8 requiring ancillary treatment.
Occasionally progression of the ethmoid hematoma may result in weakening or loss of the cribriform plate or roof of the sphenopalatine sinus.18 During mass removal, loss of this protective bony covering may result in intraoperative or postoperative neurologic complications. Recognition of loss of the integrity of these bony plates may not occur until sinus lavage. In a rare complication, death occurred after intralesional formalin injection in a horse where the cribriform plate had been eroded by the ethmoid hematoma.19 Erosion of calvarial bone is rare, but careful CT evaluation of these regions in horses with extensive hematoma formation involving the frontal or sphenopalatine sinuses is warranted.3
Irrespective of treatment method, recurrence of the hematoma occurs in 17% to 50% of cases from several months to years after the initial surgery.2,3,6-8,12,13,18 Increased use of CT to guide surgical planning and for postoperative evaluation is likely to contribute to a reduction in recurrence rates.