Surgical Disorders of the Large Intestine
Anthony T. Blikslager • John F. Marshall
Simple Obstruction
Simple obstructions of the large intestine tend to have a more gradual onset than those of the small intestine and, in the case of large colon impactions, are frequently amenable to medical therapy.1 Cecal impactions present much more of a dilemma because of the greater propensity of the cecum to rupture2 and the relative difficulty of surgically manipulating it.3
■ Cecal Impaction Cecal impaction may develop as a primary condition or may arise as a complication in horses with another disease state, particularly those that have been hospitalized and undergone surgery.4,5 Reasons for development of cecal impaction in hospitalized horses are unclear, although motility disturbances arising from postoperative pain may play a role.
Primary cecal impactions typically manifest as firm ingesta-filled impactions, whereas impactions that occur as an apparent secondary impaction tend to manifest as gross distention of the cecum with fluid ingesta. The latter has been termed cecal dysfunction and may be initiated by abnormalities in cecal motility. Evidence in favor of this supposition includes the fact that the right ventral portion of the colon is typically empty in horses with cecal dysfunction, which suggests a lack of aborad movement of digesta through the cecocolic orifice. However, clinical differentiation of cecal impaction and cecal dysfunction may be very difficult.6 Horses with primary dry ingesta-filled cecal impactions tend to have a gradual onset of abdominal pain over a number of days. Such impactions have a propensity to rupture before the development of severe abdominal pain or systemic deterioration and therefore must be closely monitored.5 In many horses with secondary cecal impactions, such as an impaction that arises in a horse hospitalized for surgery, it is very difficult to detect onset of colic because there is an expectation for horses to show some degree of depression after surgery and because many affected horses are already receiving analgesics such as NSAIDs or opiates. One potential method of detecting these cases is to closely monitor fecal output in the postoperative period.7 Normal horses should produce six to eight piles of manure per day, whereas abnormal horses may produce no evidence of defection or a marked reduction in fecal production (less than three piles of manure per day). The latter should be carefully evaluated for both pain and intraabdominal evidence of an impaction and treated accordingly.The diagnosis of cecal impaction is based on rectal palpation of a firm, impacted cecum or a grossly distended fluid-filled cecum. According to one study, such findings were detected in 89% of horses with cecal impaction that underwent rectal palpation of the abdomen.6 However, there are cases in which only the cupula is impacted, and these are reportedly not palpable rectally.8 Treatment for horses with dry ingesta-filled cecal impactions may include initial medical therapy, including aggressive administration of intravenous fluids, judicious use of analgesics, and administration of oral laxatives (e.g., 2 to 4 L of mineral oil per 500 kg).9 Other oral laxatives have also been recommended, including magnesium sulfate (1 g/kg in 4 L of water PO up to twice daily for up to 3 days) and psyllium (1 kg q6-8h).
However, if the cecum is grossly distended or if medical therapy has had no effect within a reasonable period of time, surgical evacuation of the cecum via a typhlotomy is indicated. In one comparison of treatment of cecal impaction medically or by surgical intervention, horses that had surgery had a significantly improved prognosis for survival.5 As far as surgery, it has been difficult to determine whether a cecal bypass should be performed. In some cases, if the cecum is not bypassed, cecal impaction recurs. This may be because the cecum becomes dysfunctional as a result of the impaction or because cecal dysfunction was the initial reason of impaction.10 However, in another study in which horses that had had typhlotomy alone were compared with those that had had both typhlotomy and a cecal bypass via jejunocolostomy, there was no significant difference in outcome.5 Nonetheless, this aspect of surgical treatment remains controversial.11,12
With regard to the prognosis, a study of 150 horses with cecal impaction showed that horses treated medically had a short-term survival rate of 61%, which was significantly lower than that of horses treated surgically (82%).
One year later, 57% of horses treated medically were still alive, whereas 70% horses treated with typhlotomy were still alive, as 73% of those treated with typhlotomy and jejunocolostomy.5 As previously mentioned, there was no significant difference in prognosis with the two surgical approaches. However, clinicians should be aware that there may be regional differences in the types of cecal impactions and prognoses. For example, in a study from the United Kingdom, cecal bypass was preferred because of the authors' experience with recurrence of cecal impaction.12■ Large Colon Impaction Impactions of the large colon with ingesta occur at sites of anatomic reductions in luminal diameter, particularly the pelvic flexure and the right dorsal portion of the colon.13 Although a number of reported risk factors have been reported, most have not been proven. However, a sudden restriction in exercise in association with musculoskeletal injury appears to be frequently associated with onset of impaction. In addition, one study of 120 horses with large colon impaction showed that 41% of cases were diagnosed in the winter,14 possibly in relation to reduced water intake or changes in diet. Equine feeding regimens may be very important in the development of large colon impactions. For example, twice-daily feeding of concentrate are associated with secretion of large volumes of fluid into the small intestine, which results in transient hypovolemia (15% loss of plasma volume).15 This leads to activation of the renin-angiotensin-aldosterone system; aldosterone stimulates absorption of fluid from the large colon, which may may dehydrate colonic contents.15,16 Large concentrate meals may also decrease small intestinal transit time, which results in increased presentation of soluble carbohydrate to the cecum and large colon. Large amounts of fluid enter the colon occur as concentrates are readily fermented in the large intestine, which would also be expected to activate the renin-angiotensin-aldosterone system.
This in turn also triggers net fluid absorption from the large colon. The effects of these large fluid fluxes on development of large intestinal disorders remains to be fully characterized, but undoubtedly they play some role in the syndrome of colic. From a practical standpoint, intestinal fluid fluxes may be reduced with frequent small feedings in horses requiring concentrate to maintain condition.15Clinical signs of large colon impaction include slow onset of mild colic that is typically well controlled with administration of analgesics but becomes increasingly more severe and refractory if the impaction does not resolve.14 The diagnosis is based on rectal palpation of a firm mass in the large colon. However, the extent of the impaction may be underestimated by rectal palpation alone because much of the colon is out of reach. Adjacent colon may be distended if the impaction has resulted in complete obstruction. Initially, medical treatment should be attempted. Intermittent abdominal pain is controlled with administration of analgesics (flunixin meglumine, 0.25 mg/kg IV q6h to 1.1 mg/kg IV q12h; butorphanol, 0.05 mg/kg IV as needed; or xylazine, 0.3 to 0.5 mg/kg IV as needed). Detomidine (4 to 10 mg IV as needed) can be administered but with great caution because this agent readily masks severe pain. If there are concerns about use of nonselective COX inhibitors, including flunixin meglumine, COX-2 inhibitors such as firocoxib can be used. Considerations related to nonselective COX inhibitors relate to concerns about gastrointestinal mucosal integrity, or other organ systems such as the kidneys. In these instances, a COX-2 inhibitor may be indicated for control of pain. These drugs include meloxicam, which is not labeled for horses in the United States and only modestly targets COX-2, or the highly selective COX-2 inhibitor firocoxib, which is available in the United. States. Firocoxib must be administered in an off-label loading dose (0.3 mg/ kg), followed by the labeled dose (0.1 mg/kg, IV, q24h).17
In addition to analgesics, an oral laxative should be administered via nasogastric tube.
Although mineral oil (2 L/500 kg to 4 L/500 kg PO) is commonly used as a laxative, hydration of the colonic contents can be better achieved by magnesium sulfate (1 g/kg in 4 L of water PO) or sodium sulfate (1g/kg in 3 L of water PO) by stomach tube.18 Sodium sulfate has been shown to result in greater colonic content hydration than does magnesium sulfate, but it also results in significant thirst and hypocalcemia; therefore magnesium sulfate is preferred.18 Access to feed should not be permitted, but water should be freely available. For impactions that persist, aggressive oral or intravenous fluid therapy, or both, should be instituted. One study demonstrated the increased efficacy of a continuously administered oral rehydration solution in softening feces in comparison with intravenous fluids, which are probably best suited to restoring the systemic extracellular fluid compart- ment.19 If the impaction remains unresolved, if the pain becomes uncontrollable, or if extensive gas distention of the colon occurs, surgery is indicated. At surgery the contents of the colon are evacuated via a pelvic flexure enterotomy. The prognosis is good for horses in which impactions resolve medically (95% long-term survival in one study) and fair for horses that require surgical intervention (58% long-term survival in the same study).1■ Enteroliths Enteroliths are mineralized masses typically composed of ammonium magnesium phosphate (struvite).20 One study has suggested that an increase in magnesium in the diet may predispose to the formation of enteroliths.21 Enteroliths almost always form around a nucleus such as a silicon dioxide stone, a nail (Fig. 32.70), or a piece of rope that has been ingested and are most commonly found in the right dorsal and transverse portions of the colon. Although enterolithiasis has a wide geographic distribution, the incidence in California is high. In one California-based study, horses with enterolithiasis represented 28% of the surgical colic population.
In addition, Arabian, Morgan, and American Saddlebred horses and donkeys are at risk of this disease.22 A prospective, unmatched casecontrol study performed in California indicated that horses fed a diet composed predominantly of alfalfa hay are at risk for development of enterolithiasis, and allowing horses to graze on pasture was protective against this disease.23Initially, clinical signs include intermittent abdominal pain in mature horses (almost always older than 4 years of age),24
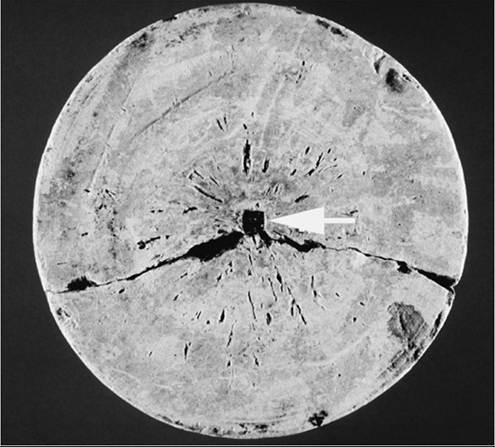
FIG. 32.70 Cut section of an enterolith. Note the presence of a nail head (arrow) that served as a nucleus for the formation of a struvite enterolith. (Courtesy Dr David G. Bristol.)
with few abnormalities on rectal examination. As enteroliths become larger, they may occlude the lumen of the colon and cause acute pain and large colon distention that necessitate surgical exploration. In some cases an enterolith is forced into the small colon, where it causes acute small colon obstruction. Enteroliths may be diagnosed on abdominal radiographs or at surgery. On rare occasions, an enterolith may be palpated rectally, particularly if it is present in the distal small colon.
In general, surgery is required for these cases, although there are reports of enteroliths being retrieved rectally. In fact, in one study, 14% of horses that presented for treatment of enterolithiasis had a history of passing an enterolith in the feces.22 However, enteroliths are typically located in the right dorsal portion of the colon, transverse colon, or small colon. At surgery the enterolith is gently pushed toward a pelvic flexure enterotomy, but removal frequently requires a separate enterotomy of the right dorsal portion of the colon to prevent rupture of the colon. After removal of an enterolith, further exploration must be conducted to determine whether other enteroliths are present. Solitary enteroliths are usually round, whereas multiple enteroliths have flat sides. The prognosis is good (the rate of 1-year survival among 900 horses that underwent surgery in one study was 92%) unless the colon is ruptured during removal of an enterolith.22 Colon rupture occurred in 15% of the 900 cases.22
■ Sand Impactions of the Large Colon Sand impaction of the large colon is common in horses with access to sandy soils, particularly horses whose feed is placed on the ground. Sand accumulates in the large colon, particularly the right dorsal portion of the colon and pelvic flexure, but may be present in multiple locations.25,26 In addition, sand may trigger diarrhea, presumably as a result of irritation of the colonic mucosa.27 In horses with sand impactions, clinical signs are similar to those of horses with large colon impactions. In addition, sand may be found in the feces, and auscultation of the ventral abdomen may reveal sounds of sand moving within the large colon.28 Radiography of the cranioventral portion of the abdomen may be useful for the detection of sand within the large colon and can serve to monitor resolution of sand accumulation.29 In particular, one study showed that horses with a greater area of sand accumulation, multiple sand accumulations, and more gas on radiographs were significantly more likely to require surgery.30 The diagnosis is definitively made at surgery but may be tentatively based on clinical signs compatible with a large colon impaction, together with evidence of sand in the feces. To determine the presence of sand, several fecal balls are placed in a rectal palpation sleeve or other container, which is subsequently filled with water. Sand, if present, will accumulate at the bottom of the container.
Initially, medical therapy should consist of a laxative such as mineral oil, magnesium sulfate, or psyllium in combination with enteral or intravenous fluid therapy; this is usually successful in the management of uncomplicated sand enteropathy.29 Administration of psyllium hydrophilic mucilloid in water by stomach tube may facilitate passage of sand, although an experimental study failed to show a benefit of this treat- ment.31 If colic becomes intractable, surgical evacuation of the large colon should be performed. Care must be taken to prevent tearing of the colon as a result of the weight of sand during exteriorization.32 The prognosis is good; for instance, in one study, more than 94% of horses survived to discharge, regardless of whether they were treated medically or surgically.30
Nonstrangulating Obstruction of the Colon
Several configurations of displacements, including nephrosplenic entrapment of the colon, obstruct the colonic lumen but do not compromise the colonic blood supply. Therefore these are technically simple obstructions. However, the lumen may not be completely obstructed, and some degree of venous congestion is common.34 In some cases, nonstrangulating obstructions are difficult to differentiate from large colonic volvulus because a volvulus of less than 270 degrees does not result in strangulation of blood supply but can cause considerable abdominal pain and gas distention of the abdomen. In this regard, nonstrangulating obstructions represent early stages of strangulating obstructions. Clinical signs include mild to moderate colic with evidence of large colon distention on rectal palpation of the abdomen. The diagnosis is confirmed at surgery.35 However, there is evidence that horses with suspected displacements can be successfully treated with a medical regimen, including fluids, analgesics, and exercise.33 However, if pain is recurrent, particularly if it is of increasing intensity and frequency, or if there is evidence of intestinal compromise (particularly progressive changes in abdominal fluid and cardiovascular parameters indicating systemic deterioration), the horse should undergo surgery immediately. The prognosis for nonstrangulating obstructions of the large colon is good; more than 80% of horses in one report survived to hospital discharge.36
■ Right Dorsal Displacement of the Large Colon With right dorsal displacement of the colon, the colon is displaced to the right of the cecum. Findings on rectal palpation typically include colonic bands coursing horizontally across the abdomen, with evidence of colon lateral to the cecum. In the most common configuration of right dorsal displacement, the large colon wraps around the cecum (pivoting counterclockwise around the cecum, in a view from above the horse), with the pelvic flexure lying in the left dorsal quadrant. Alternatively, the colon may wrap around the cecum in the opposite direction, with the pelvic flexure lying in the right dorsal quadrant.37 One study suggested that although the prognosis for recovery after surgical correction of right dorsal displacement is good, this condition is associated with an increased risk of colic episodes in the postoperative period.38 The reason for this has not been elucidated but may reflect an etiologic difference between right dorsal displacement and other simple obstructions of the large colon.
■ Nephrosplenic Entrapment (Left Dorsal Displacement) of the Large Colon On the left side of the equine abdomen, colon displacements most commonly involve entrapment of the colon over the nephrosplenic ligament, although left dorsal displacements may be detected before the colon is fully entrapped. Clinical signs include gradual onset of mild to moderate colic as the entrapped colon fills with gas. Rectal palpation reveals gas distention of the ventral portion of the colon and displacement of the spleen toward the center of the abdomen. Careful palpation by following colonic bands up to the left dorsal quadrant often reveals the presence of colon between the left kidney and the spleen. Diagnosis may be based on rectal palpation of the colon traversing the nephrosplenic ligament. Alternatively, a tentative diagnosis can be reached with abdominal ultrasonography.39 The spleen can be visualized on the left side of the abdomen, but the dorsal spleen and left kidney are obscured by gas-distended bowel, the dimensions of which may extend cranially from the paralumbar fossa. As with other examination techniques, ultrasonography is not uniformly reliable and occasionally yields false-positive results and false-negative results. A definitive diagnosis may necessitate surgery.
Treatment has traditionally been surgical intervention, during which the colon is gently rocked free of the nephrosplenic space. However, good success rates have been reported for nonsurgical intervention such as either light exercise (trotting) or physical manipulation (rolling) to return the colon to a normal location.40,41 In addition, phenylephrine (3 to 6 μgZkg/ min over 15 minutes) may be administered before exercise or rolling to decrease the size of the spleen.42 In affected horses exhibiting mild pain and normal abdominocentesis findings, light trotting exercise for a period of 30 to 45 minutes may help correct the displacement.40,43 Alternatively, the horse is anesthetized and placed in right lateral recumbency in preparation for rolling. The horse is rotated up to dorsal recumbency, rocked back and forth for 5 to 10 minutes, and then rolled down into left lateral recumbency.44 One study showed that rolling is more effective than other medical treatments, including administration of phenylephrine and exercise.45 Regardless of nonsurgical technique adopted, the resolution of displacement should be monitored by repeat rectal palpation of the nephrosplenic space and by ultrasonography to determine whether the entrapment has been relieved. If the entrapment remains, or there is any deterioration in clinical signs, the horse should undergo surgery.
Regardless of technique, the prognosis is good. Several studies have demonstrated survival rates exceeding 90%.40,46 Recurrence of left dorsal displacement has been described and may affect up to 23% of horses.47 To prevent recurrence, laparoscopic closure of the nephrosplenic space may be performed after correction of the displacement.47-49
■ Atresia Coli Atresia of any segment of the colon is a rare congenital abnormality in horses (Fig. 32.71).50 The heritability and causes of the condition are unknown. One potential mechanism for development of the lesion is intestinal ischemia during fetal life, which secondarily results in necrosis of a segment of intestine. Clinical signs include a failure to pass meconium and colic within the first 12 to 24 hours of life. Secondary abdominal distention results from complete intestinal obstruction, and abdominal radiographs may reveal gas distention of the colon. The diagnosis is made at surgery. Any portion of the colon may be absent, but the distal segment of the large colon or the proximal small colon is usually most severely affected. If sufficient tissue is present, anastomosis to the proximal blind end of the colon may be attempted. The prognosis depends on which segment of the colon is absent but is usually poor because of an absence of distal portion of the colon.

FIG. 32.71 Operative view atresia coli in a foal. Complete atresia of the pelvic flexure has resulted in a blind-ended ventral portion of the colon (arrows), which in turn resulted in gas distention of the colon. The ventral portion of the colon was subsequently anastomosed to the dorsal portion of the colon in this case.
Strangulating Obstruction
Although simple obstruction of the large colon carries a very favorable prognosis, strangulating obstruction of the large colon is associated with high fatality rates in most centers.51 However, this is likely to be dependent on the duration of disease: In at least one referral center, early referral was associated with a marked increase in survival.52 Two forms of strangulating obstruction are recognized: hemorrhagic strangulating obstruction, in which the arterial blood flow remains patent while veins are collapsed, and ischemic strangulating obstruction, in which both the arteries and veins are collapsed. The differentiating factor between the two is probably how tightly twisted the volvulus is. It has been suggested that ingesta-filled intestine is more likely to develop a hemorrhagic lesion during the development of volvulus because the intestinal contents prevent the intestine from twisting tightly.53
■ Large Colonic Volvulus Clinical signs of large colonic volvulus include rapid onset of severe, unrelenting abdominal pain.54 Although postparturient broodmares appear to be at risk, this association has not been conclusively determined. However, one study demonstrated that Thoroughbred horses are at significant risk for volvulus.51 Once the large colon is strangulated (>270-degree volvulus), gas distention is marked, leading to gross distention of the abdomen, respiratory compromise as the distended bowel presses against the diaphragm, and visceral pooling of blood as the caudal vena cava is compressed. This condition is frequently refractory to even the most potent of analgesics. Affected horses may prefer to lie in dorsal recumbency, presumably to take weight off the strangulated colon. An abbreviated physical examination is warranted in these cases because the time elapsed from the onset of strangulation to surgical correction is critical.52 In experimental conditions, the colon is irreversibly damaged with 3 to 4 hours of 360-degree volvulus of the entire colon.55
Despite severe pain and hypovolemia, the heart rate may be paradoxically slow, possibly in relation to increased vagal tone. A fast heart rate can be associated with a poor prognosis.56 More accurate prognostic information can be obtained from plasma lactate. A plasma lactate concentration of 6.0 mmol/L or higher is 84% sensitive and 83% specific for predicting death.57 In another study, preoperative PCV of more than 46% was associated with a significantly increased risk of death.52 Results of abdominocentesis are often not indicative of the degree of colon compromise,58 and in many cases abdomino- centesis is not advisable because of extreme colonic distention. Rectal palpation reveals severe gas distention of the large colon, which often restricts access of palpation to the abdomen beyond the pelvic brim. In most cases, colonic bands can be palpated, which indicate that the ventral portion of the colon is uppermost and crossing the abdomen horizontally. The diagnosis may be tentatively based on signalment, severity of pain, and degree of distention.
At surgery the volvulus is typically located at the mesenteric attachment of the colon to the dorsal body wall, and the most common direction of the twist is dorsomedial with the right ventral portion of the colon as a reference point. However, the colon may twist in the opposite direction, twist more than 360 degrees (up to 720 degrees has been reported), or twist at the level of the diaphragmatic and sternal flexures. In all cases, the colon should be decompressed as much as possible, and in many cases, evacuation of colon contents via a pelvic flexure enterotomy helps correct the volvulus. However, in horses in which colonic volvulus is diagnosed in the early stages, the volvulus can be corrected within the abdomen without evacuation of the colon.52
After correction of the volvulus, the colon should be assessed for irreversible injury. This determination is frequently based on mucosal color and bleeding (if an enterotomy has been performed), palpation of a pulse in the colonic arteries, serosal color, and appearance of muscular motility. However, determination of viability on the basis of these parameters is unreliable. Currently, one of the most reliable techniques for determining viability is histologic evaluation of frozen sections of colonic mucosa. Biopsy samples may be obtained at the pelvic flexure because it has been determined that mucosal changes are uniform throughout strangulated colon.59 A prediction of viability can be based on the degree of luminal and crypt epithelial loss and the interstitium-to-crypt ratio (calculated from measurements of the crypt width and the width of interstitial space between crypts). In one study, morphologic changes consisting of an interstitium-to-crypt ratio of less than 3 and a 60% or less loss of glandular epithelium were predictive of survival with a sensitivity and specificity of 95% and 92%, respectively, in a population of 52 horses.60
In addition, it has been suggested that accuracy of viability determination can be increased by combining histologic evaluation with surface oximetry or laser Doppler determination of blood flow.61 Unfortunately, frozen histologic sections are not available at most referral centers on an emergency basis. A retrospective study of formalin-fixed biopsy specimens of pelvic flexure from 28 horses found that morphologic scoring was not accurately predictive of short-term survival.62 In another study, investigators assessed intraoperative colonic intraluminal pressure as a more practical potential indicator of outcome in horses with large colonic volvulus but found this measurement inaccurate for making this determination.63 In a more recent study of formalin-fixed biopsy samples of pelvic flexure from a population of horses recovered from surgery for large colonic volvulus, a combination of both interstitium-to-crypt ratio and mucosal hemorrhage score was accurately predictive of survival.51
If the colon is judged to be irreversibly damaged, the feasibility of a large colon resection can be considered. Although 95% of the colon can be resected (that part of the colon distal to the level of the cecocolic fold), damage from the volvulus usually exceeds what can be resected. In these cases surgeons may advise euthanasia or may elect to resect as much damaged bowel as possible; however, resection of the colon has not been found to improve survival.51
Postoperative complications include hypovolemic and endotoxemic shock, extensive loss of circulating protein, disseminated intravascular coagulation, and laminitis. In addition, large colonic volvulus has a propensity to recur. The prognosis for survival to hospital discharge for cases of large colonic volvulus has been reported as between 58% and 88%.52,64-67 Studies in which long-term follow-up has been completed have demonstrated that survival rates decline to between 34% and 66% after 2 years.63,64 Although one study documented a recurrence rate of less than 5%,58 some authors believe recurrence may be as high as 50%. Methods of preventing recurrence can be considered in patients considered at risk for recurrence.68,69
■ Intussusception The most common intussusception of the large intestine is cecocolic intussusception, although in comparison with all forms of colic, it is a relatively rare condition of horses, accounting for 11 (1.3%) of 842 horses taken to surgery because of colic at one hospital.70 The condition tends to occur in young horses (2 to 3 years of age) and may be associated with intestinal parasites, particularly tapeworms71 and a heavy larval cyathostome burden.72
Clinical signs include acute onset of colic that varies in severity according to the degree of intussusception. Initially, the cecal tip inverts, creating a cecocecal intussusception, which does not obstruct flow of ingesta. As the intussusception progresses, the cecum inverts into the right ventral portion of the colon (cecocolic intussusception), which obstructs flow of ingesta and often causes severe colic. In one report on cecocecal and cecocolic intussusception, 26 of 30 horses presented with signs of acute colic.71 However, the condition may also manifest as a chronic disease.71 The cause of abdominal pain is often difficult to differentiate in these cases, although it is sometimes possible to detect a mass on the right side of the abdomen and the concurrent absence of a palpable cecum. Treatment involves manual surgical reduction by retracting the intus- susceptum directly or via an enterotomy in the right ventral portion of the colon, with or without a partial typhlotomy.71 The prognosis is usually regarded as poor because of severe compromise to the cecum and the risk of cecal rupture or severe contamination during surgery. However, a report of 18 horses without peritonitis that recovered from surgery showed that 15 survived long term.71
Colocolic intussusceptions are rare but have reportedly affected the pelvic flexure and the left portion of the colon.73-76 The condition is reportedly more common in young horses, but some older horses are affected. Clinical findings may include a palpable mass on the left side of the abdomen. Ultrasonography may also be useful. Treatment requires manual reduction of the intussusception at surgery, or resection of affected bowel.