Disorders of the Stomach
Gayle D. Hallowell
Various diseases affect the equine stomach and include equine squamous gastric disease (ESGD), equine glandular gastric disease (EGGD), parasitic disease (Gasteropbilus spp., Habronema spp., Draschia spp.), gastric impactions, gastric rupture, and squamous cell carcinoma.
This section covers these conditions with a particular focus on EGGD, about which a number of reports have been published.■ Equine Squamous Gastric Disease Historically, this has been the most prevalent disease identified in the equine stomach. However recent personal communications and anecdotal reports suggest that the prevalence of this condition has fallen since 2005, particularly in sports and leisure horses.1 This change in prevalence may be actual, secondary to an understanding of risk factors and subsequent changes in management, or different diseases are diagnosed instead because more veterinarians have longer gastroscopes and thus are able to examine the pylorus and pyloric antrum.
ESGD can be a primary problem or, occasionally, a secondary problem that results from obstruction of gastric outflow with subsequent backflow of acid gastric juices or alkaline biliary secretions. The focus of this section is on primary squamous disease. The management of secondary squamous disease is largely dictated by treatment of the primary disease causing delayed gastric outflow.
PATHOPHYSIOLOGY. ESGD results from increased exposure of the squamous mucosa, which has limited mechanisms of defense against highly acidic gastric contents. Horses constantly secrete gastric acid,2,3 and hydrochloric acid is primarily responsible for the damage to the squamous mucosa. Damage occurs rapidly; acid injury becomes evident within 30 minutes of exposure in vitro.4 Horses are constant grazers, and in pasture conditions, the consumption of roughage creates a basketballsized bolus of feed in the stomach that acts as a buffer to absorb gastric acid and physically prevents the splashing of gastric contents into the dorsal region of the stomach that is lined by squamous mucosa (Fig.
32.50). Any disruption in normal feeding or behavior results in breakdown of this protective mechanism and a resultant increase in the risk for ESGD. Short-chain fatty acids released during fermentation of soluble carbohydrates consumed in the diet are also likely to contribute directly to squamous mucosal injury5 and disrupt the physical protective effect of a predominantly roughage-based diet. ESGD thus is largely a disease that results from the management changes imposed on horses for a variety of purposes.CLINICAL SIGNS. Clinical signs reported with ESGD include poor appetite, poor bodily condition, and abdominal discomfort.6 Other clinical signs loosely associated with ESGD include poor appetite or “picky eating,”6-9 poor bodily condition or weight loss,6,7,10 chronic diarrhea,6,7 poor coat,8, bruxism,11 behavioral changes (including aggression and nerviousness),',12, acute or recurrent abdominal pain,6,7,8,14-16 and poor performance.7,8,17-19
PREVALENCE AND RISK FACTORS. The prevalence of ESGD mirrors exercise intensity: The risk of disease development
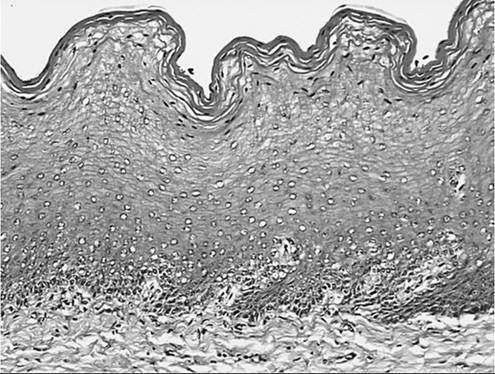
FIG. 32.50 Photomicrograph of equine gastric squamous epithelial mucosa. Multiple layers of epithelium are arranged in parallel with the luminal surface. The most superficial layers of cells are cornified, and superficial to these cells are layers of keratin. (Hematoxylin and eosin stain.)
increases as the intensity of work increases. The highest prevalence of this disease has been reported in Thoroughbred racehorses, of whom more than 70% are affected across a wide range of studies.8,11,20,21 However, it seems likely that these studies overstate the prevalence of clinically significant disease because many affected animals have only small focal lesions that are likely to be clinically insignificant but, by definition, meet the criteria for diagnosis of ESGD.
This overrepresentation has led many clinicians to dismiss ESGD as a normal finding in a performance horse. It is proposed that mild (grade II/IV) ESGD may be an incidental finding and that although it may be associated with clinical signs, horses with grade III-IV/IV ESGD are more likely to have clinical disease.22 The prevalence and significance of ESGD should be discussed in the context of the relative severity of lesions observed.The Thoroughbred racehorse is the best studied of horse breeds regarding risk factors and effective treatments. However, ESGD is identified in a wide range of other horse breeds. In a Danish study, ESGD was observed in 69% of horses with varying activities, ranging from horses at pasture to horses in hard work, and there was no association between presence of ESGD and horse use.23 Similar prevalence of ESGD has been reported in Standardbred (63% to 87%3,24), endurance (67% to 93% during competition25,26), show (58%12), and western performance (40%27) horses. The prevalence of ESGD in horses at rest is variable but typically lower and, when observed, tends to be less severe. However, in selected cases, severe (grade III-IV/IV) ESGD can be observed in horses at pasture, and ESGD should not be omitted in the differential diagnosis simply because a horse does not meet the typical risk profile.
The commencement of training, with the multitude of management changes imposed, including exercise28 and high- concentrate/low-roughage diets,29 can result in the development of ESGD within 7 days.30,31 In addition to the overall risk associated with the induction of training, specific risk factors that have been identified for ESGD include fasting,32 transport,31 stabling,3 and time in work.32 NSAIDs may induce ESGD experimentally; however, because of epidemiologic study results21 and the lack of a direct link to the pathophysiology of squamous ulceration, it is unlikely that NSAIDs contribute to ESGD in the clinical setting.
TREATMENT. Treatment of ESGD focuses on suppression of acid production and, when possible, changing management practices that may have contributed to the disease (Fig. 32.51). Acid suppression therapy does not contribute directly to healing, but the squamous mucosa has an enormous proliferative capacity,
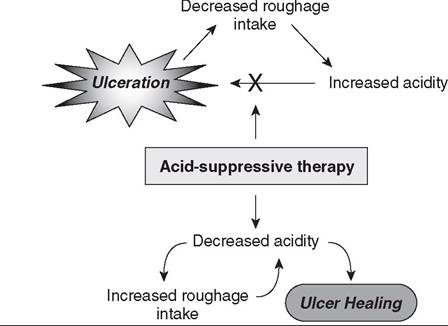
FIG. 32.51 Diagram representing the pathophysiologic process of ulceration in the equine gastric squamous mucosal epithelium and the permissive effect of acid suppression on ulcer healing.
and the removal of ongoing insult is usually sufficient for the tissues to heal. Theoretically, removal of affected horses from the risk factors that caused disease and reestablishment of a normal pH gradient in the stomach should result in healing. However, a reduction in workload is often not possible, and treatment is required in the presence of ongoing exposure to risk factors. Furthermore, even when removal from the risk factors is possible (i.e., resting of an affected horse), acid suppression therapy is often necessary to restore a normal appetite so that enough roughage is consumed to reestablish the pH gradient in the stomach and thereby allow healing to occur. If removal from work is used to manage ESGD, then follow-up gastroscopy 4 to 6 weeks later is indicated to ensure that healing has occurred.
Because the ability to remove risk factors, such as exercise and concentrate diets, can be limited, the use of acid suppression therapy remains a cornerstone in the management of ESGD. Various drugs have been used for this purpose, but oral omeprazole remains the most effective and best studied. Omeprazole inhibits the H+, K+-adenosine triphosphatase (proton) pump that secretes hydrochloric acid. Omeprazole is most commonly administered at a dose of 4 mg/kg PO q24h for 28 days, and its efficacy at this dose for treatment of ESGD has been well documented by several clinical trials.33-37 The use of lower doses has been evaluated and, under certain conditions, doses as low as 1 mg/kg have been shown to be as efficacious as 4 mg/kg in the treatment of ESGD.38 On the basis of experimental studies,39-45 it is widely believed that once-daily administration of omeprazole results in 24 hours of acid suppression; however, one study has suggested that the duration of acid suppression after dosing at 4 mg/kg may be as short as 12 hours; thus in nonresponders, administration twice daily may be warranted.46 As exercise is considered to be the peak risk period for ESGD development,28 timing of omeprazole administration should be considered before exercise.
However, one study revealed no advantage of administration of omeprazole 1 to 4 hours before exercise over administration after exercise.47Reported healing rates at 28 days for horses that stay in work are typically around 70% to 8O%.33,34,37,47.Although the majority of affected animals improve by 28 days,33,38,47,48 repeated gastroscopic examination is recommended before therapy is terminated to ensure that healing has occurred.
The H2 receptor antagonists ranitidine and cimetidine are the other drugs that historically have been used for treating ESGD. Both drugs work by competitively blocking the H2 receptor on the parietal cell, and their efficacy is dependent on maintaining plasma concentrations. Ranitidine, administered most commonly at 6.6 mg/kg PO q8h, has been shown to effectively suppress gastric acidity in experimental studies2,14,49,50 and provides an alternative option for acid suppression. However, in a direct comparison of the efficacy of ranitidine with that of omeprazole, ranitidine was shown to be inferior,35 and thus omeprazole remains the treatment of choice. Cimetidine has been poorly studied in this context, and its use is not justified.
For nonresponding patients, which usually is only 10% of animals with ESGD, or those animals to which oral paste cannot be administered, long-acting injectable omeprazole (4 mg/kg IM q5-7 days) should be considered. It can be administered every 5 to 7 days, and studies have shown that it results in effective acid suppression during this period.51 A small-scale clinical study demonstrated healing in 14 days in 100% of patients.51 This drug should be administered via deep intramuscular injection into the gluteal mm. Transient swelling has occasionally been reported.1
Nonpharmaceutical methods, such as feed supplements and antacids, are popular among owners for the treatment of ESGD because of their low cost and availability.
Although antacids can effectively reduce gastric acidity, their effect is short-lived (2 hours)14,52 and so their use cannot be recommended. Mucosal protectants, such as pectin-lecithin complexes, may play a role in providing a physical barrier between the mucosa and acid, and short-term improvement in clinical signs associated with the use of antacids is often reported. Their use in selected cases may be sufficient for control of ESGD, but they should be considered alongside management changes to prevent recurrence, and alongside omeprazole in the treatment of ESGD, rather than as a primary treatment for ESGD.PREVENTION OF RECURRENCE. To prevent recurrence of disease, management changes should be recommended. These changes include increased roughage and decreased concentrate in the diet; multiple, smaller feeds; increased turnout; and feeding a small amount of feed, such as a few handfuls of chaff, before exercise to act as a raft to protect the squamous mucosa from acid splash.22 The use of mucosal protectants such as the pectin-lecithin complexes or administration of sugar beet, which contains pectin, should be recommended in the few months after treatment and may be required longer. Historically omeprazole has been used at 1.0 mg/kg PO q24h for prevention,31 but 0.5 mg/kg PO q24h has been shown, under specific conditions, to be as effective.47 Recent data in humans have revealed an association with long-term omeprazole therapy and acute kidney injury53; no such studies or association has been performed in horses, but this approach may not be innocuous. Gastric acid is produced for a reason!
■ Equine Glandular Gastric Disease (EGGD) It is now widely accepted that EGGD is an entity separate from ESGD.1 A series of studies have clearly demonstrated that the
32 38474854
risk factors for EGGD32 and response to its treatment38,4',48,54 differ dramatically from those for ESGD, which is not surprising in view of the differences in the anatomy of the glandular mucosa (Fig. 32.52) and probable pathophysiologic features. EGGD is probably multifactorial in nature in horses.1 Since 2005, the identification and reported prevalence of this disease have increased. Many authorities believe that this is a true change in disease prevalence; squamous disease is less common as a result of improved management based on risk factors and also is less likely to be diagnosed because of increased awareness of EGGD as an individual entity. Historically, some of the difference in prevalence reported may also relate to endoscopes available; those initially available in the 1990s were only 2.5 m in length, and therefore the pyloric antrum, where the majority of glandular disease occurs,23,32,38,47,48,54 was rarely observed in clinical cases.
PATHOPHYSIOLOGY. The glandular mucosa differs from the squamous mucosa in that under normal physiologic conditions, it is exposed to highly acidic gastric contents; the pH in the ventral portion of the stomach is relatively stable at between 1 and 3.46 Whereas ESGD results from exposure of mucosa unaccustomed to acidity, EGGD may result from a breakdown of the normal defense mechanisms that protect the mucosa from acidic gastric contents, which includes bicarbonate and a layer of gastric mucus that is a mixture of glycoproteins, water, electrolytes, lipids, and antibodies.55
Lesions of the glandular mucosa are not ulcerative in most situations; they are erosive and inflammatory in nature. They often contain a mixed inflammatory population of lymphocytes, plasmacytes, and neutrophils and should thus be described as glandular gastritis.56-58 Nodular lesions typically have a lymphocytic, plasmacytic infiltrate. Although lesions that have a fibrinosuppurative cap often have a predominance of neutrophils, their presence does not indicate an infectious cause.1
As mentioned, EGGD is probably a multifactorial condition. Different lesion types and location of lesions may have different
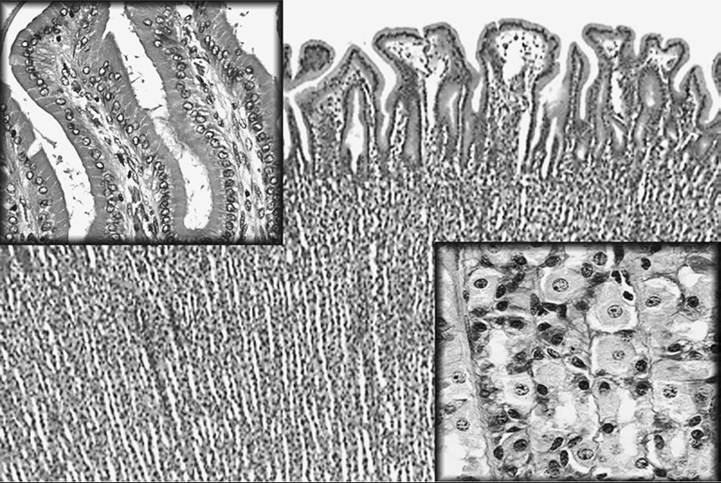
FIG. 32.52 Photomicrographs of equine gastric glandular mucosa. In contrast to the squamous mucosa, the glands are parallel to one another and perpendicular to the luminal surface. There are multiple cell types within the mucosa, with surface epithelial cells and mucus-secreting cells toward the lumen, and parietal cells, chief cells, enterochromaffin-like cells, G cells, and D cells deeper in the mucosa. The top left insert is a high-power magnification of cells lining gastric pits on the surface of the epithelium. The bottom right insert is a high-power magnification of cells lining the gastric glands deeper in the mucosa. (Hematoxylin and eosin stain.)
causes, and thus responses to treatment may be different. The glandular mucosa in the pyloric, fundic, and cardiac regions differs in anatomy, physiology, and blood flow, which may be why most of the lesions identified in adult horses occur around the pylorus or in the pyloric antrum.1
Changes in blood supply may result in breakdown of normal defense mechanisms. Stress may influence gastrin production, reduce blood supply to the glandular mucosa, and thus initiate and perpetuate this condition. Blood supply to different areas of the glandular mucosa is thought to be uneven, and both exercise and feeding could result in initiation or perpetuation of disease.1
Acid injury is unlikely to be the initiator of these lesions, but it may perpetuate mucosal damage and prevent mucosal healing.22
Because these lesions contain an inflammatory infiltrate, it is entirely possible that some lesions are gastric manifestations of inflammatory bowel disease (IBD) and may necessitate similar treatment and management strategies, including evaluation of the remaining intestinal tract.1
CLINICAL SIGNS. Clinical signs of EGGD are often nebulous, which makes assessing clinical significance of lesions challenging. According to a consensus statement,1 clinical signs that are considered associated with EGGD include changes in temperament, including nervousness and aggression; changes in rideability, including reduced willingness to work and reluctance to go forward; unexplained weight loss, probably concurrently associated with reduced appetite or altered eating patterns; cutaneous sensitivity, manifested as flank-biting or resentment of girthing, leg aids, or rugging; and mild or recurrent abdominal pain.1 It was deemed unlikely that changes in coat condition, stereotypical behavior, bruxism, and diarrhea were signs associated with EGGD.1
Although cutaneous sensitivity seems an implausible clinical sign of gastric disease, data from other species suggests that afferent pathways from abdominal viscera and the sixth to ninth thoracic spinal nerves are pooled, so that afferent signals from the skin may be affected by input and misinterpreted within the brain. In addition, viscerosomatic reflexes can result in pain and sensitivity in segmentally related structures such as the skin.59
PREVALENCE AND RISK FACTORS. EGGD prevalences of 47 to 62.5%20,32 have been reported in Thoroughbred racehorses in Australia. Among a mixed population of horses in Denmark, the overall prevalence of EGGD was 57%23; in sports horses in the United Kingdom, 65%60; and in endurance horses, 27 to 33%.25,26 Abattoir studies have reported prevalences of 57% to 67%56-58 in a variety of horse types.
Information on risk factors for EGGD are limited and occasionally contradictory. What is obvious from these studies, however, is that risk factors for EGGD are different to ESGD. Warmbloods are at greater risk for developing EGGD than are other horse types.61,62 In Thoroughbred racehorses, trainer was identified as a risk factor independent of other management factors.32 Exercising for more than 4 or 5 days per week has been shown to be a risk factor in both Thoroughbreds using for racing32 and in showjumpers,63 whereas intensity of exercise was not. Horse experience was inversely correlated with prevalence of EGGD in both polo ponies64 and showjumpers,63 which may suggest adaptation to type of work or differences in management of elite horses.1 A study in endurance horses demonstrated a doubling in EGGD prevalence during the competition season in comparison with off-season activity,26 which, as in human athletes, may be related to reduction in gastric and splanchnic blood flow during exercise.
Stress is an important risk factor in the development of glandular lesions in people.65-67 Horses with severe EGGD have greater increases in cortisol in response to novel stimuli,68 and in response to exogenous adrenocorticotropic hormone,69 which suggests that these horses may be more sensitive to stress. There is controversy regarding the association with stereotypies; no association was found in one study,32 whereas was an association with crib-biting was found in another.70 These differences may be explained by the high prevalence of both conditions in a given population, particularly as stereotypies are often regarded as a coping strategy in horses. What would be more interesting to evaluate is disease prevalence in animals that are prevented from exhibiting stereotypical behavior. The lower prevalence in more experienced polo ponies and showjumpers63,64 may relate to adaptation to physiological stress. Cortisol concentrations have been shown to be lower in more experienced show and showjumping horses than in less experienced horses.71,72 It is challenging to know what is stressful to an individual horse; changes to minimize stress should be tailored to an individual and ideally kept consistent.
It is often perceived that there is an association between orthopedic and EGGD, but thus far no such association has been demonstrated,32 and care is warranted because animals that present with poor performance often have multiple abnormalities that contribute to presenting signs.
There is currently no evidence to indicate an association between diet and EGGD, and thus making recommendations are challenging. However, grazing should be maximized (if this does not result in stress), and animals should not exercise on an empty stomach.1
In humans, bacterial agents and NSAIDs are the predominant causes of gastric disease; Helicobacterpylori-negative, NSAID- negative gastric disease is rare.73 In horses, however, there is no evidence that bacteria are involved in the pathogenesis of EGGD. Several investigations in horses have failed to consistently identify Helicobacter-like organisms in EGGD lesions.56,57,74,75 Other bacterial species such as Escherichia fer- gusonii, Streptococcus bovis, and Enterococcus faecium are potentially pathogenic and have been associated with EGGD lesions, but their pathogenicity remains unproven; they may simply be colonizers. Studies on the gastric microbiota have failed to identify a difference between horses with EGGD and those without.76 Thus no current data suggest that bacteria are an important cause of EGGD, although the potential for bacteria to cause this disease is plausible.
The theoretical potential for NSAIDs to cause EGGD is plausible as cyclooxygenase (COX) inhibition could reduce gastric and splanchnic blood flow. Glandular lesions can be induced if flunixin, phenylbutazone, and ketoprofen are administered at doses 50% higher than typically recommended,62 whereas at clinical doses, phenylbutazone and suxibuzone did not induce gastric disease when administered for 15 days.63 Moreover, the administration of NSAIDs has not been identified as a risk factor.28,32,62-64,77,78 Thus at doses commonly used in clinical cases of horses that are otherwise healthy, the risk of EGGD associated with short-duration NSAID therapy is negligible.
TREATMENT. It is widely accepted that ESGD and EGGD cannot be managed in the same way. In three studies, only 25% of glandular lesions healed with 28 to 35 days of omeprazole monotherapy at 4.0 mg/kg PO q24h, in direct contrast to an ESGD healing rate of 78%,28,37,38 which suggests that this treatment is not appropriate for EGGD and that other treatment is required.
One plausible treatment option for EGGD is a combination of oral omeprazole (4 mg/kg PO q24h) and sucralfate (12 mg/ kg PO q12h). Sucralfate is known to provide a physical barrier that prevents acid diffusion, stimulates mucus secretion (which blocks acid diffusion), inhibits pepsin and bile acid secretion, promotes epithelialization by preventing fibroblast degradation, stimulates epidermal and insulin-like growth factors, and increases mucosal blood flow through increased production of prostaglandin E. Data on its efficacy varies between studies. One study79 demonstrated an 80% improvement and a 63% healing rate with this combination at 28 days, whereby healing was reported to represent grade 0 or 1 EGGD lesions, although improvement rates were lower for lesions around the pyloric antrum (67.5%). Another study,80 in which the end point for healing was a completely normal appearance of the pyloric antrum, demonstrated a healing rate of only 22% at 28 days, although improvement rates were similar to those in the previously described study. If this combination is to be used, omeprazole should be administered on an empty stomach, and the animal should not be fed for 30 to 60 minutes after administration.1 Sucralfate is not licensed for veterinary use, and so appropriate consent should be obtained before administration.
A second plausible treatment for this condition is administration of oral misoprostol (5 μg∕kg q12h), which is licensed for treatment of refractory gastric disease in humans; however, it is not licensed for veterinary use. Misoprostol is a prostaglandin E analogue and as such probably improves mucosal blood flow. It has also been shown to effectively suppress acid production in horses81 and inhibits neutrophilic inflammation.82 One study80 demonstrated healing, defined as return to normal appearance, in 73% of horses with significant pyloric glandular lesions that were treated with misoprostol; in contrast, the healing rate among those treated with combined omeprazole and sucralfate therapy was only 22%. Side effects are rare, but those reported with misoprostal administration include mild, transient diarrhea, mild abdominal pain, and urticaria. Care must be taken in administration to pregnant mares because this drug can induce abortion, although some safety data suggest that it can be safely administered to mares between 100 and 130 days pregnant.83 Appropriate consent should be obtained before administration because this drug is not licensed for veterinary use and because of the potential for causing abortion in people, it should not be dispensed to women who are pregnant or planning to be pregnant. There is no rationale for combining this drug with oral omeprazole.
A third plausible option for the treatment of EGGD is long-acting injectable omeprazole. This drug administered at 4 mg/kg IM has been shown to be more effective than oral formulations in increasing pH in the ventral portion of the stomach51; acid suppression is maintained for 4 to 7 days, and so this drug should be administered at 5- to 7-day intervals. Thus far, the data available on the efficacy of this drug in clinical cases are limited. However, in a small study of Australian racehorses, 75% healing and 100% improvement was reported at 2 weeks after two injections.51 Some unpublished data from sports and leisure horses demonstrated 64% healing, defined as mucosal appearance returning to normal and 96% healing at 2 weeks after two injections given 7 days apart.1 Transient swelling has been reported in fewer than 10% of cases at the injection site, which is most common if administered into the pectoral muscle or neck. It is thus recommended that this drug be administered, after warming, as a deep intramuscular injection into the gluteal muscle. Appropriate consent should be obtained when this drug is used because it currently is not licensed for veterinary use.
If some of these lesions are extensions of inflammatory bowel disease, there may be some rationale in the use of glucocorticoids. Anecdotal reports indicate that they are beneficial in the subgroup of animals that do not respond to more conventional therapies listed previously. In a consensus, morning administration of prednisolone, 1 mg/kg PO q24h, or dexamethasone, 0.05 to 0.1 mg/kg PO q 24h, was suggested. Either dosage can be tapered over a 4- to 5-week period.1 Other recommendations may include simplification of the diet (in view of underlying causes of IBD in other species, such as cereal proteins or alfalfa).
As stated previously, the role of bacteria in EGGD is unknown, but Helicobacter-like organisms are not consistently identified and are not considered an important factor in the initiation or perpetuation of EGGD.22 In one study, the combination of omeprazole (4 mg/kg PO q24h) and trimethoprimsulfadimidine (30 mg/kg PO q24h) failed to improve the treatment response in comparison with omeprazole therapy alone (4 mg/kg PO q24h).54 In one consensus, investigators believed that antimicrobials were not an appropriate first-line treatment for EGGD; their use was deemed appropriate only if based on histologic and bacteriologic findings1 and was necessary in fewer than 1% of cases.
There is no evidence that ranitidine, aloe vera, pectin-lecithin complexes, polysaccharides, kaolin, bismuth subsalicylate, sea buckthorn, acupuncture, or homeopathy is efficacious in the treatment of EGGD.1
If ESGD and EGGD lesions are found concurrently, treatment should be aimed at EGGD. No additional treatments are required because ESGD would be expected to heal with any of the first-line treatments discussed for EGGD (combined omeprazole-sucralfate, misoprostal, and injectable omeprazole).
Expectations for Healing and Monitoring. Rates of healing are difficult to predict and probably vary by lesion. Raised, nodular, and fibrinosuppurative lesions probably take longer to heal than do flat, hemorrhagic lesions. Mucosal restitution can occur within 3 to 5 weeks, but complete resolution may take several months, especially where raised areas or nodules are visible.
Affected horses should be evaluated monthly with gastroscopy until resolution is complete. Once lesions have resolved, treatment should be discontinued. There is no rationale for reducing the dose of the drugs discussed previously, with the exception of glucocorticoids. Affected horses should also be monitored for return of clinical signs. The need for follow-up gastroscopy depends on the case being managed.
MANAGEMENT OF REFRACTORY CASES. Because many EGGD lesions are not healed in 28 to 35 days, it is prudent to have a rational plan of what to do when lesions are still present. The aims of treatment should be complete resolution with a mucosa that has a normal appearance. If treatment is prematurely discontinued, lesions may worsen again and clinical
1
signs will recur.1
If first-line treatment yields no improvement at 28 to 35 days, or if an affected horse's condition deteriorates, an alternative first-line treatment should be used. If the alternative treatment produces improvement, it should be continued up to a maximum of 3 months. If the lesions have not resolved by 3 months, biopsy samples of the lesions should be obtained and investigations performed to establish evidence of concurrent intestinal disease.1 If the biopsy reveals neutrophilia and if cultures of multiple sections yield a predominant bacterial species, treatment with an antimicrobial is warranted; many clinicians opt for oral doxycycline. If there is evidence of lymphocytic-plasmacytic inflammation or of IBD, then glucocorticoid treatment may be warranted. The finding of an eosinophilic infiltrate may be suggestive of parasitic organisms (Habronema spp. or Draschia spp.), and management with anthelmintics is warranted; these organisms, however, are extremely rare.
PREVENTION OF RECURRENCE. Prevention of EGGD, either as primary disease or as recurrence, is problematic. In a series of studies, worsening of EGGD grade was observed in 23% of horses despite omeprazole monotherapy at doses ranging from 1 to 4 mg/kg PO q24h.38,47,48 Furthermore, it has been suggested that gastric hyperplasia may be present in a percentage of EGGD cases, and that in such cases omeprazole therapy is contraindicated.84 As stated previously, no data are available as to whether long-term omeprazole therapy results in acute kidney injury, as it does in humans.53
On the basis of the known risk factors for EGGD listed previously, which differ from those for ESGD, the following management changes are recommended. Ideally, horses should have a minimum of 2 rest days per week if possible. Stress should be minimized; for example, environments should be calm, and affected horses should have a minimal number of carers and the same equine field companions. Horses should be turned out, unless this is obviously stressful to a horse. Horses should be fed 2 L of chaff or equivalent of forage 30 to 60 minutes before exercise.1 If IBD is suspected, diets should be simplified to include one straight and forage. Any irritant supplements (such as those containing magnesium sulfate) should be stopped.
In one study, the addition of corn oil, 0.3 to 0.45 mL/kg/ day (150 to 225 mL/day for a 500-kg horse), decreased gastric acid output and increased prostaglandin E2,85 both of which are, in theory, beneficial in the treatment and prevention of EGGD. Thus addition of corn oil at a rate of up to 0.5 mL/ kg/day may be beneficial. Lastly, in view of the fundamental role of failed mucosal defenses in the pathogenesis of EGGD, the use of mucosal barrier protectants is logical, and the use of pectin-lethicin at 150 g q12h or feeding sugar beet pulp (a cheaper alternative) may be beneficial.84
DIAGNOSIS. Gastroscopy remains the only reliable method for diagnosing ESGD and EGGD. Adequate patient preparation, plus some operator skill and patience, is required for a complete diagnostic evaluation of the entire stomach. A fasting period of at least 12 to 16 hours is required in most horses, and even small amounts of residual food hamper access to the pyloric antrum. In horses on low-roughage diets (e.g., racehorses), the duration of fasting may be shorter. Removal of water 1 hour before examination is advantageous but not mandatory. Examination of the stomach should be complete and methodical. Observation of the squamous mucosa is straightforward, whereas passage through to the pyloric antrum is more technically demanding. However, observation of the pyloric antrum is critical because the majority of glandular lesions in adult horses occur in this region. ’ ’ ’ ’ Observation of the most ventral portion of the fundus is typically not possible because of the presence of fluid, but it can be possible with adequate patient preparation; however, disease in this region is rare.84 The squamous and glandular mucosa should be assessed and scored separately and, although a variety of scoring systems have been described, the author prefers the system first described by the Equine Gastric Ulcer Syndrome (EGUS) council,87 shown in Table 32.2, for squamous disease. It is now widely accepted that the grading system for EGGD does not reflect severity of disease and until a better system is developed, lesions should be described according to the consensus statement by the European College of Equine Internal Medicine and the American College of Veterinary Internal Medicine.22 These descriptors include focal, multifocal, and diffuse; mild, moderate, and severe; nodular, raised, flat, and depressed; and erythematous, hemorrhagic, and fibrinosuppurative. A more recent consensus statement focused on EGGD suggested that flat, erythematous lesions were likely to heal more rapidly than were those with a nodular, raised, and fibrinosuppurative or hemorrhagic appearance.1 Examples of the normal appearance of the gastric and duodenal mucosa and lesions encountered in horses and foals undergoing gastroscopy are shown in Color Plates 32.4 through 32.12.
Fecal occult blood tests88 and sucrose permeability tests89 for diagnosing gastric disease in adult horses have been shown to be unreliable and cannot be recommended.
■ Gastric Disease in Foals and Weanlings Gastric disease is commonly identified in foals; the prevalence ranges from 21 to 98%.90-94 Before weaning, the prevalences of squamous and glandular disease is similar,94 whereas after weaning, the prevalence increases to levels similar to those
■ TABLE 32.2
Scoring System for Equine Gastric Ulcer Syndrome
Glandular
| Grade | Squamous Mucosa | Mucosa |
| 0 | Intact epithelium, no appearance of hyperkeratosis (yellow appearance to the mucosa) | Intact epithelium, no hyperemia (reddening) of the mucosa |
| I | Intact mucosa, but areas of hyperkeratosis | Intact mucosa, but areas of hyperemia |
| II | Small single, or multifocal lesions | Small single, or multifocal lesions |
| III | Large single or multifocal lesions, or extensive superficial lesions | Large single or multifocal lesions, or extensive superficial lesions |
| IV | Extensive lesions with areas of apparent deep ulceration | Extensive lesions with areas of apparent deep ulceration |
among adults, and lesions are twice as likely to be found in the squamous mucosa as in the glandular mucosa.94 As in adults, diagnosis is confirmed with gastroscopy. Results of one study suggested that a sucrose permeability test is a useful screening tool for detecting gastric disease in weanlings; with a sucrose cut-off level of of 24 μmol∕L, this test had excellent sensitivity (84 to 95%) and average to good specificity (47 to 71%).94
The pathophysiologic origins of this condition in foals are probably complex and, as in adults, probably differ between the squamous and glandular mucosa. Acid production is extremely variable in foals; in fact, gastric fluid is often alkaline,95 which suggests that acid damage is unlikely to be a prevalent cause. Underlying diseases such as perinatal asphyxia syndrome, hypovolemia secondary to other disease and use of NSAIDs probably results in reduced gastric and splanchnic blood flow, and improvement of this should be the focus for prevention and treatment. Gastric disease in foals often co-occurs with lesions that extend into the esophagus and duodenum.
Clinical signs observed in this age group are nonspecific but are often more severe than in adults; they include diarrhea, abdominal pain (restlessness, rolling, lying on the back), excessive salivation, bruxism, and anorexia.96 However, with such high prevalence, determining which lesions are clinically significant in the absence of clinical signs is challenging,93 but because of the risk of intestinal perforation, which is fatal, many authors believe that these lesions should be treated.96,97
Because of the pathophysiologic process of this condition, the rationale for the use of sucralfate98 or misoprostal81,99 for prevention and treatment is significant. Omeprazole may play a role in the treatment of gastric lesions but should not be used for prophylaxis. Use of omeprazole prophylaxis in human patients was associated with an increased risk of pneumonia and C. difficile diarrhea,100,101 and in foals in a multicenter study, it was associated with an increased risk of diarrhea.102
■ Gastric Impaction Gastric impaction is relatively common. Clinical signs are diverse, with inappetence the most common manifestation and representing 50% of cases in one study.103 Affected horses typically eat small amounts and have a significantly decreased total daily intake. Acute and recurrent 103 104
colic are also common manifestations.1, The causes or gastric impaction are unclear, and although poor dental care has been 105
proposed as a predisposing factor,105 cases commonly occur in horses with no dental abnormalities. Three types of gastric impaction are recognized: Type I is impaction of feed material without increase in the stomach size; type II is impaction of feed material with increase in the stomach size and, although difficult to prove, an underlying motility disorder is suspected in these cases on the basis of the poor response to treatment and prognosis; and type III impactions occur after the formation of a phytobezoar secondary to persimmon seed ingestion.104,106 Classification of the type of gastric impaction is important because treatment and prognosis vary depending on the type. Distinguishing between types I and II can be difficult.
Diagnosis of gastric impaction in the field is difficult, but it should be part of the differential diagnosis in any horse with signs of mild abdominal pain that dramatically worsen after the administration of fluids via a nasogastric tube; in horses with unexplained inappetence; and horses with abdominal pain that appears to resolve with fasting, only to relapse with the reintroduction of feed. The clinical signs observed with type I impactions are typically mild, with a normal heart rate.70 Signs may be more pronounced in type II impactions, and displacement of the spleen may be palpable on rectal examination. Type III impactions more commonly manifest with mild to severe colic, weight loss, or both.104,106 Definitive diagnosis is made when, after an appropriate period of starvation, entry to the stomach with a gastroscope is obstructed by feed material. Alternatively, in type I, the stomach can often be entered and distended with air, but a clearly defined ball of feed material extending above the level of the margo plicatus is visible. In type III impactions a phytobezoar is typically visible once the stomach has been otherwise emptied of feed material. Ultrasonography can help distinguish between type I impactions, in which visualization of the stomach is difficult or limited, and type II impactions, in which the stomach distention often extends for several rib spaces.
In all cases, any concurrent systemic abnormalities such as hypovolemia, dehydration, and electrolyte derangements should be corrected, and resolution of the impaction should be confirmed by gastroscopic examination before food is reintroduced. The different types are treated as follows:
• For type I, the use of enteral fluids is highly effective; isotonic electrolyte solution (1 L/100 kg q2h) is administered via an indwelling large-bore nasogastric tube. Depending on the response, the rate and volume can be increased or decreased Administration of analgesia (e.g., flunixin meglumine, 1.1 mg/kg IV q12h) is recommended until resolution of the impaction, because signs of abdominal discomfort are common. The use of indwelling, small-bore nasogastric tubes for the administration of enteral fluids has been described107; in theory, the bolus administration of fluids should result in a more pronounced stimulation of the gastrocolic reflex, but the use of these tubes will probably cause less abdominal discomfort. With enteral fluid therapy alone, the prognosis is excellent (90% survival to discharge),103 and so alternative therapies probably offer little advantage, although gastric lavage with water or the addition of carbonated cola drinks may be helpful.
• For type II impactions, treatment is similar to that of type I impactions, but caution should be exercised in the volume of fluids administered because the stomach wall is often friable and gastric rupture can occur. Concurrent intravenous fluid therapy should be considered if hypovolemia cannot be corrected and maintenance fluid requirements cannot be met with enteral therapy alone. The response of type II cases to treatment is often poor, and the addition of prokinetics may be beneficial in some cases; however, the response to prokinetic therapy is often disappointing. Bethanechol (0.025 mg/kg SC q4-6h) is the prokinetic of choice,17 but
it is often difficult to obtain; erythromycin (1 mg/kg IV q6-8h) is a reasonable alternative. Surgery should be considered for types I and II impaction if the animal is showing signs of systemic deterioration or if the impaction does not resolve with medical therapy within 5 to 7 days; successful treatment by gastrotomy has been reported.108 The prognosis for type II impactions has not been reported, but in anecdotal reports, it is guarded because gastric rupture can occur (even without enteral fluid therapy) and recurrence is common. The use of low-bulk diets during the refeeding stage is logical.
• Type III impactions by persimmon seed phytobezoars are generally refractory to standard enteral and intravenous fluid therapy. The use of carbonated cola drinks has been reported with a variety of techniques ranging from constant infusion of 1 L/h for 1 to 3 days to bolus administration of 700 mL q12h via nasogastric tube. The mechanism is believed to be a combination of the mucolytic effects of sodium bicarbonate, the acidifying effects of the cola, and mechanical disruption of the fibers of the phytobezoar by the stable carbon dioxide bubbles.104 Constant infusion via a small-bore nasogastric tube appears to be the treatment of choice, and the use of caffeine-free diet cola is recommended to reduce the risk of caffeine toxicosis or laminitis secondary to carbohydrate overload. The prognosis for type III impactions appears to be good; five of eight horses responded to medical therapy in one report.104 In the same report, two additional horses were successfully treated surgically via laparotomy, with manual manipulation of the phytobezoar but without gastrotomy; the horse in which a gastrotomy was attempted was euthanized at surgery because of extensive contamination of the abdominal cavity.104
■ Miscellaneous Diseases of the Stomach A variety of miscellaneous disease conditions, including gastric rupture, abscesses, tumors, and pyloric stenosis, also affect the stomach of horses.
GASTRIC RUPTURE. Gastric rupture is most commonly secondary to obstruction of the small intestine or chronic gastric impaction. Idiopathic rupture accounted for 17% of cases in one report,109 which suggests that a variety of other causes can result in rupture.
GASTRIC ABSCESSATION. These lesions are rare and are most common in foals. They can be secondary to gastric disease, R. equi bacteremia, foreign body penetration, and septic peritonitis. Signs are nonspecific and include fever, neutrophilia, increased serum concentrations of fibrinogen and serum amyloid A, anemia, weight loss, and, on occasional. abdominal pain. Diagnosis usually is made through gastroscopy and ultrasonography. Often a diagnosis is not made until a late stage of the disease, and although long-term antimicrobial therapy can be attempted, the prognosis is usually poor.
GASTRIC TUMORS AND OTHER MASSES. Squamous cell carcinoma (Fig. 32.53) is the most commonly reported of the tumors that affect the equine stomach, representing nearly 80% of cases in one report.110 Other neoplastic conditions that affect the equine stomach include primary gastric adenocarcinoma, metastatic lymphoma, mesothelioma, and bile duct carcinoma. Gastric squamous cell carcinoma affects the squamous mucosa and can metastasize to other abdominal viscera or extend into the esophagus. As with other forms of neoplasia, presenting signs include chronic weight loss, abdominal pain, and spontaneous nasogastric reflux. No breed or sex predilection exists, and a wide range of ages are affected, although gastric squamous cell carcinoma usually affects older horses. Diagnosis is typically based on gastroscopic and ultrasonographic examination
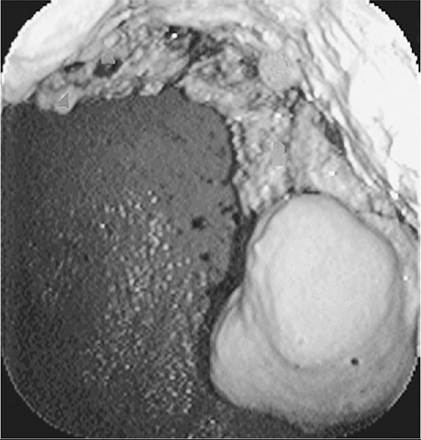
FIG. 32.53 Endoscopic view of a gastric squamous cell carcinoma.
findings, and the prognosis is poor because there is no described treatment.
Nonneoplastic masses that can be identified in the stomach include lesions associated with Draschia megastoma, Habronema spp. (Fig. 32.54), proliferative granulation tissue, and adenomatous masses in the antrum and pylorus. Lesions around the pylorus can be challenging to differentiate from EGGD.
PYLORIC STENOSIS. Pyloric stenosis is an uncommon condition that typically affects foals and young horses,111 although horses of any age can be affected. It is thought to result most commonly from chronic gastric disease, although other space-occupying lesions may be the cause. Affected animals typically have a history of weight loss, poor appetite, postprandial abdominal pain, or recumbency.111 Excessive ptyalism or spontaneous reflux of gastric contents from the nasal passages is common. Diagnosis is typically made via gastroscopy, although ultrasonography and contrast radiography can be useful adjunctive tests. Conservative management involves acid suppression therapy; omeprazole (4 mg/kg PO q24h) is effective in less severe cases. Intravenous fluid therapy and parenteral nutrition is indicated in patients with spontaneous reflux of gastric contents or in cases in which gastric emptying is significantly delayed. Long-acting injectable omeprazole at (4 mg/kg IM every 5 to 7 days) has not been reported for management of these cases, but it is likely to be more efficacious than oral medication.51 Administration of bethanechol or erythromycin may be advantageous. Response to medical therapy is often disappointing and early surgical intervention is indicated in such cases. Long-term survival rates of 50 to 69% have been reported for gastrojejunostomy,112,113 which further supports early surgical intervention in nonresponsive cases.
Endotoxemia and Sepsis
Kelsey A. Hart • Erin McConachie Beasley •
Robert J. MacKay
■ Definitions The term endotoxin was originally coined to describe toxic bacterial components that were contained within or on the bacterial cell, in comparison with exotoxins that were secreted from outside bacterial cells. The heat-stable endotoxic activity of Vibrio cholera, identified by Richard F. J. Pfeiffer in the late nineteenth century, resides in lipopolysaccharide
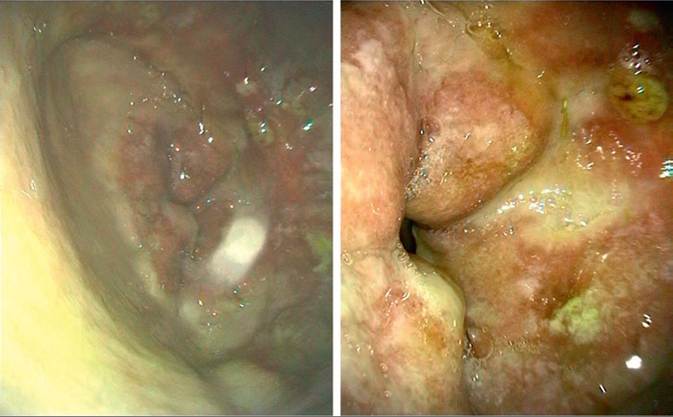
FIG. 32.54 Images from the pylorus and pyloric antrum of a horse with recurrent colic. Biopsies of these lesions confirmed gastric habronemiasis. The horse was treated on several occasions with ivermectin, and within 3 months the lesions had resolved and clinical signs disappeared.
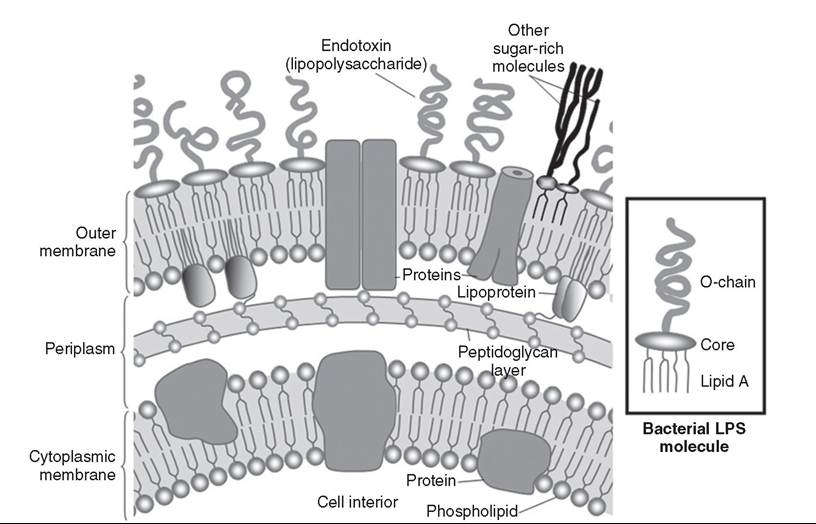
FIG. 32.55 Illustration of a cross-section of the double lipid bilayer that forms the cell membrane of Gram-negative bacteria. Lipopolysaccharide (LPS) is the principal component of the outer leaflet of the outer membrane. The insert shows a single LPS molecule with an O-polysaccharide chain, a two-part core oligosaccharide, and a hydrophobic lipid A phospholipid. R-mutant bacteria lack the O-chain and the phospholipid; varying amounts of the core oligosaccharide are present.
(LPS), the principal component of the outer leaflet of the outer membrane of all Gram-negative bacteria1 (Fig. 32.55). Today, the terms endotoxin (the activity) and LPS (the molecule) are used synonymously to refer to this specific Gram-negative bacterial membrane component, except when purified LPS is being referenced.2 Each LPS molecule has three structural domains: a polar polysaccharide O region, which projects into the aqueous extracellular environment; a hydrophobic lipid A region, which is largely buried in the bacterial outer membrane; and a core acidic oligosaccharide region connecting the other two. The O-region is highly variable, consisting of repeating units each of one to eight glycosyl residues, and contains antigens specific for each bacterial strain; the core glycolipid region is relatively constant among bacteria and mediates most of the toxic effects of endotoxin. On bacterial death or during bacterial proliferation, large (molecular mass > 106 D) aggregates of LPS and membrane protein are released. It is these protein-lipid micelles that constitute native endotoxin.
Endotoxemia literally is the presence of endotoxin in the blood. However, when the term is used clinically, it implies the presence of clinical signs typically caused by the inflammatory response to circulating endotoxin. Endotoxemia—actual circulating endotoxin or related clinical signs—can occur with Gram-negative bacterial infection in any tissue or through exposure to Gram-negative enteric bacteria any time the intestinal mucosal barrier is compromised.
The ability to respond to minute local concentrations of endotoxin by mounting vigorous inflammatory responses is well conserved across species.3 Endotoxemia as a clinical syndrome in equine patients was first recognized in the mid-1960s.4 The potential clinical importance of equine endotoxemia is clear from reports that intravenous infusion of LPS into horses reproduced many of the adverse clinical signs of diseases such as colitis, metritis, and strangulating intestinal obstruction.5-10 Further evidence of the importance of endotoxemia was the detection of circulating endotoxin in some horses with experimentally induced laminitis11 or intestinal strangulating obstruction12 and in horses with naturally occurring gastrointestinal diseases or septicemia,13-1' hemostatic disorders,16 and exhaustion associated with endurance18 or racing19 events. Since these original descriptions, a large body of review literature has documented the efforts that have been made to understand and, more importantly, treat equine endotoxemia.20-23
Endotoxemia should not be confused with either bacteremia, which refers only to the presence of viable circulating bacteria and can occur without clinical signs, or septicemia, which refers to systemic disease caused by any circulating microorganisms or their products, or both. Sepsis is a related term that is best defined as clinical evidence of an infection (documented or suspected) coupled with the presence of a systemic inflammatory response syndrome (SIRS).24,25 SIRS is characterized in humans and animals by alterations in any two or more of the following: body temperature, heart rate, respiratory rate, and leukogram parameters (Table 32.3).24-28 The presence of SIRS does not confirm infection, inasmuch as a variety of noninfectious conditions—such as trauma, hemorrhage, thermal injury, or toxin exposure—that result in the release of tissue damage- derived host molecules can also induce a systemic inflammatory of response. However, clinical findings consistent with SIRS should raise the clinician’s level of suspicion that an infectious process is present and support a diagnostic search for a potential infectious process.
A scheme showing increasingly severe stages of SIRS and sepsis, from local infection to death, is shown in Fig. 32.56, and adapted definitions for SIRS in horses and foals are listed in Table 32.3. In general, severe sepsis includes sepsis (infection plus SIRS) and evidence of organ dysfunction, and septic shock includes severe sepsis plus acute circulatory failure (usually manifested by persistent hypotension after appropriate volume resuscitation).25 Dysfunction of two or more organs in severe sepsis/septic shock is termed multiple-organ dysfunction syndrome (MODS) and has a high rate of mortality in human beings29 and in horses with gastrointestinal disease.30,31 The lethality of each grade increases from the base to the apex of Fig. 32.56; reported mortality rates for sepsis are 10 to 20%, those for severe sepsis are 20 to 50%31 and those for septic shock are 40 to 80% in humans.32 Comparable mortality data in horses are not currently available for increasing severity of sepsis. However, in horses with gastrointestinal disease, the presence of SIRS, increased severity of organ dysfunction and increased number of dysfunctional organs are all associated with an 2830
increased risk of death.28,30
■ TABLE 32.3
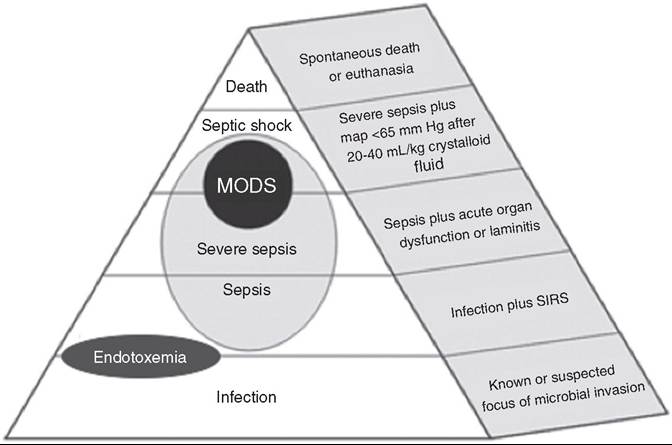
FIG. 32.56 Scheme for classification of the degree of sepsis. Systemic inflammatory response syndrome (SIRS) and organ dysfunction are defined in Tables O Γ J - JlJ ∖ Z DJ
32.1 and 32.2 and in several studies.28,30,41,44 MODS, multiple organ dysfunction syndrome.
Criteria for Diagnosis of Systemic Inflammatory Response Syndrome in Horses and Foals28,30,41,44
| Criteriaa | Adult | Foal |
| Alteration in body | 102.5°F | |
| (38.6° C) | (39.2° C) | |
| Alteration in the | 12,500/ μL | |
| or >10% band | or >10% band | |
| neutrophils | neutrophils | |
| Tachycardia | >52 beats/min | >120 beats/min |
| Tachypnea | >25 breaths/min | >30 beats/min |
| or PaCO2 | 24 hours||
| Cardiovascular | Vasopressor therapy for >24 hours |
aFor diagnosis, two or more criteria must be present.
The fundamental difference between serious sepsis in humans and the syndromes seen in equids is the propensity for the latter to be associated with laminitis. In the context of sepsis, laminitis is often life-threatening. Moreover, it appears that the same types of global inflammatory and coagulation disorders that lead to MODS in patients with sepsis also are involved in the pathogenesis of both carbohydrate- and black walnut- induced experimental laminitis.33-37 In view of their likely common pathogenesis, laminitis is considered—along with evidence of cardiac, renal, hepatic, neurologic, coagulation, or gastrointestinal compromise—part of the spectrum of MODS in equine sepsis.30 Several researchers have utilized these or similar criteria for SIRS, MODS, or septic shock in horses or foals (Table 32.4; see Table 32.3 and Fig. 32.56).28,30,38-44
The extraordinary ferocity of SIRS as triggered by endotoxin was nicely captured by Thomas45:
“The Gram-negative bacteria...display lipopolysaccharide...™ their walls and these macromolecules are read by our tissues as the very worst of bad news. When we sense lipopolysaccharides we are likely to turn on every defense at our disposal; we will bomb, defoliate, blockade, seal off, and destroy all tissues in the area.. Cells believe that it signifies the presence of Gram-negative bacteria, and they will stop at nothing to avoid this threat.”
Although this modern conception of the early immune response to endotoxin is still accurate, it has become clear that a variety of other pathogen-derived molecules set off similar or identical host responses. For example, toxic shock syndrome resulting from Staphylococcus aureus infection46 and streptococcal toxic shock47 are examples of hyperinflammatory septic syndromes in horses that resemble diseases characterized by true endotoxemia (circulating LPS). Thus in sepsis—including putative endotoxemia in horses—it is likely that the clinical presentation is an aggregate of responses to multiple or varied microbial signals, as well as to certain “danger” signals generated by the host itself. In the case of horses, circulating endotoxin is not always detectable in horses described as “endotoxic”—in fact, it is typically found in fewer than 30%48,49—which suggests that other microbial components and host inflammatory molecules probably trigger similar clinical signs. Thus sepsis or SIRS is a more appropriate term than endotoxemia for the accurate description of the clinical findings usually attributed to endotoxin in horses (e.g., hyperemic or toxemic mucous membranes, fever, tachycardia, tachypnea, leukopenia). In this section, sepsis implies SIRS in response to any microbial infection, and endotoxemia refers specifically to the presence of endotoxin in the blood or to the specific clinical signs related to documented circulating endotoxin. However, the molecular basis of sepsis in horses via mechanisms other than endotoxemia is poorly understood at best, and so the majority of the following discussion centers on endotoxemia as an important component of equine sepsis.
■ Pathophysiology
ENTRANCE OF ENDOTOXIN OR OTHER MICROBIAL PRODUCTS INTO THE CIRCULATION. Although endotoxin and other microbial components are ubiquitous in the environment, both free and as a component of intact bacteria, these components normally are excluded from the body by the skin and mucous membranes. If the protective integument or mucosae are subjected to bacterial infection or otherwise damaged, bacteria or bacterial components such as endotoxin may reach the blood in sufficient amounts (engages TLR4 on cells of the innate and adaptive immune systems, especially mononuclear phagocytes (monocytes and macrophages), neutrophils, endothelial cells, and dendritic cells. Although endotoxin binds predominantly to TLR4, a number of TLRs (13 identified in mammals to date) are available to bind to other PAMPs/DAMPs (Table 32. 7).63 During sepsis, this diversity of TLRs allows redundant signaling of inflammatory cells. For example, non-LPS components of Gramnegative bacteria may bind other TLRs (e.g., flagellin binds to TLR5, lipoprotein and peptidoglycan bind to TLR2), whereas PAMPs from Gram-positive bacteria, viruses, or fungi bind different TLRs in the course of polymicrobial sepsis.63 Equine TLR signaling has been characterized in many cells and tissues.64-66 Of interest is that whereas LPS is a potent stimulator of equine monocytes via TLR4, flagellin (via TLR5) preferentially stimulates neutrophils and induces little response from monocytes,67 which suggests differential expression of these TLRs between cell types in horses that could play a role in clinical sepsis. Thus although TLR ligand-specificity appears to be well conserved across species, specific TLR expression varies among cells, tissues, and species and can result in varied responses to the same PAMP. Tissues subject to attack by mediators produced after the initial round of TLR binding can also amplify the inflammatory response by releasing DAMPs
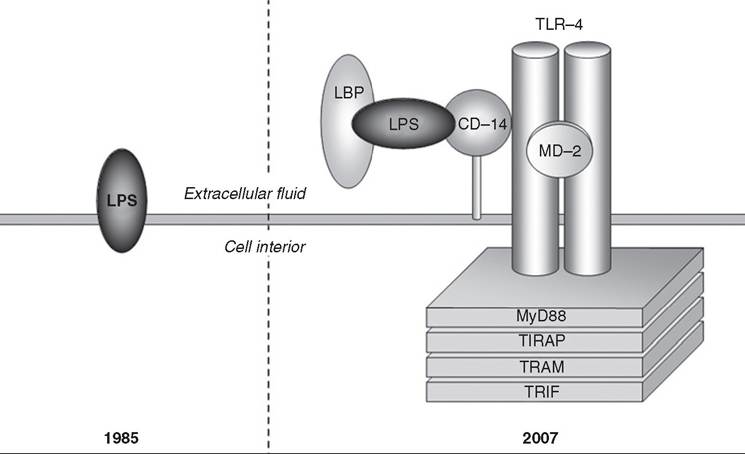
FIG. 32.57 Binding of lipopolysaccharide (LPS) to mammalian cell membranes. Initially (in 1985) it was widely believed that LPS initiated cellular signaling by hydrophobic interactions with the plasma membrane, but by 2007 the components of the signaling complex were more fully understood. In addition to the extracellular receptor components (discussed in the text), the intracellular Toll-interleukin-1 receptor (TIR) domain is shown interacting with four adaptor molecules (MyD88, TIRAP, TRAM, TRIF) to initiate a molecular signaling cascade that ultimately leads to gene activation. CD-14, cluster of differentiation 14; MD-2, lymphocyte antigen 96; TLR, Toll-like receptor.
| ■ TABLE 32.7 | |
| Seven Ligands fo | r Human Toll-Like Receptors56,226 |
| TLR1 | Triacyl lipopeptides |
| TLR2 | Lipoprotein Peptidoglycan (Gram-positive bacteria) Lipoteichoic acid (Gram-positive bacteria) Zymosan (yeast) Lipoarabinomannan (mycobacteria) |
| TLR3 | Viral double-stranded RNA |
| TLR4 | LPS Respiratory syncytial virus fusion protein HSP70 |
| TLR5 | Flagellin |
| TLR6 | Diacyl lipopeptides Zymosan |
| TLR7 | Viral single-stranded RNA |
| TLR8 | Viral single-stranded RNA |
| TLR9 | CpG oligodeoxynucleotide Herpes virus DNA |
| TLR10 | Not determined |
| TLR11 | Profilin-like protein (Toxoplasma gondii) |
| TLR12 | Profilin-like protein (Toxoplasma gondii) |
| TLR13 | 23s Ribosomal RNA (bacteria) |
CpG, Cytosine triphosphate deoxynucleotide followed by guanine triphosphate deoxynucleotide, linked by phosphodiester; HSP, Heat shock protein; LPS, lipopolysaccharide; TLR, Toll-like receptor.
(e.g., high-mobility group box 1)68, which in turn can bind to TLR or other PRRs.
During cellular activation, endotoxin and other microbial products can also interact with soluble PRRs normally present in plasma. Of particular importance is that endotoxin binds to complement proteins to initiate the lectin-dependent and alternative pathways of complement activation and activates coagulation factor XII (Hageman factor) to set off the “contact” system of coagulation.
RELEASE OF MEDIATORS. Endotoxin-induced NF-κB activation in peripheral blood and tissue leukocytes (and many other cell types) acts via multiple signaling pathways to induce the expression of more than 200 genes, many of which are involved in the pathogenesis of sepsis.52,60,69 These include genes for proinflammatory cytokines (e.g., tumor necrosis factor [TNF], interleukins 1β, 6, 8, 12, and 18 [IL-1β, IL-6, IL-8, IL-12, IL-18]), chemokines (e.g., IL-8, macrophage inflammatory protein [MIP]), type 1 interferons (IFNs), procoagulants, adhesion molecules, immunoreceptors (e.g., TNF receptors), enzymes (e.g., elastase), and acute-phase proteins (e.g., fibrinogen). NF-κB activity is further amplified by the paracrine actions of these proinflammatory cytokines and by other DAMPs, cellular hypoxia, cellular necrosis, and chemical stress (including oxidant stress). Two of the cytokines secreted by macrophages, IL-12 and IL-18, stimulate IFN-γ synthesis and secretion from natural killer and other cells.70 Because IFN-γ is a potent stimulator of both innate and acquired immune responses, it is considered a principal link between the two systems.
Endotoxin activates coagulation factor XII (Hageman factor), which leads both to liberation of bradykinin and to initiation of intravascular coagulation. Of even more importance is that complement is activated by alternative, lectin-mediated, and classical pathways to yield numerous active peptide products that play a role in opsonization, inflammatory cell trafficking, and microbial cell lysis. Other microbial structural components and products similarly stimulate inflammation, complement activation, and coagulation, although specific pathways and molecular mechanisms are less well characterized in humans than in horses.
Systemic Inflammatory Response Syndrome in Early Sepsis
The initial (early) phase of sepsis is often referred to as the “hot” phase and is characterized by inflammation, coagulation, and necrosis. The principal NF-κB-mediated events during early sepsis are summarized in Fig. 32.58. This phase has been described as a “cytokine storm,” during which there is flooding of inflammatory, procoagulant, and vasoactive mediators throughout the body. The net effects of these mediators promote microvascular injury and hypotension. The singular contributions of many mediators to sepsis is demonstrated by experiments with sepsis models in which blocking or deleting a single mediator has had a positive effect on outcome.
In early stages of sepsis, large numbers of neutrophils accumulate on the endothelial surfaces of organs undergoing failure, and insult to one organ can trigger the widespread recruitment and sequestration of neutrophils in others. Such a scenario may contribute to the association of laminitis with severe intestinal disease,71-74 although altered insulin and glucose dynamics,75,76 vascular derangements,72 or contributions of multiple inflammatory mediators77 may also play a role in the development of laminitis in septic horses.
PAMPs (including LPS), inflammatory cytokines, and complement peptides induce expression of selectins on endothelial cells, and neutrophils.52 Selectins E and P on endothelial cells and selectin L on neutrophils reciprocally engage glycoprotein ligands to “tether” the neutrophil to the endothelial surface. A series of these transient interactions between ligands and receptors allows neutrophils to roll along the endothelial surface (Fig. 32.59). Neutrophil capture is most efficient in areas of low shear force such as the walls of postcapillary venules and in pulmonary capillaries. During rolling, neutrophils are activated by selectins, chemokines, and platelet-activating factor expressed on endothelial cells. The firm attachment or arrest step of the cascade is mediated by the avid interaction of neutrophil integrins with adhesion molecules of the immunoglobulin superfamily expressed on endothelial cells. During firm attachment the activated neutrophil spreads out and, in the healthy animal, squeezes between the intercellular junctions of adjacent endothelial cells and migrates into tissues up a gradient of chemotactic factors such as microbial chemotaxins, leukotriene B4, IL-8, or complement component 5a (C5a). In contrast, in comparison with normal neutrophils, those found in septic animals have defective chemotactic responses but bind with greater avidity to the endothelium and to other neutrophils. When cultured, macrophages and neutrophils from patients with Gram-negative sepsis are hyporesponsive to LPS, which suggests a functional switch to LPS tolerance during the early stages of endotoxemia78 (see Fig. 32.59). Sequestration of neutrophils on activated endothelium and in neutrophil aggregates accounts for the neutropenia found in most horses with endotoxemia. Of interest is that the life span of these sequestered neutrophils is prolonged during sepsis because normal apoptosis is prevented,79 which might potentiate the inflammatory response during early sepsis.
Tightly adherent neutrophil-endothelial conjugates formed during sepsis seal off microscopic pockets between the juxtaposed cells into which cellular products can be concentrated. Of particular significance are the reactive oxygen species (ROS) produced as a result of the activation of the reduced forms of nicotinamide adenine dinucleotide (NADH) oxidase and of nicotinamide adenine dinucleotide phosphate (NADPH) oxidase in neutrophils (respiratory burst) and xanthine oxidase in endothelial cells.51,69 Digital laminae of horses may be particularly vulnerable to the effects of ROSs because of low content of the endogenous oxidant scavenger superoxide dismutase.80
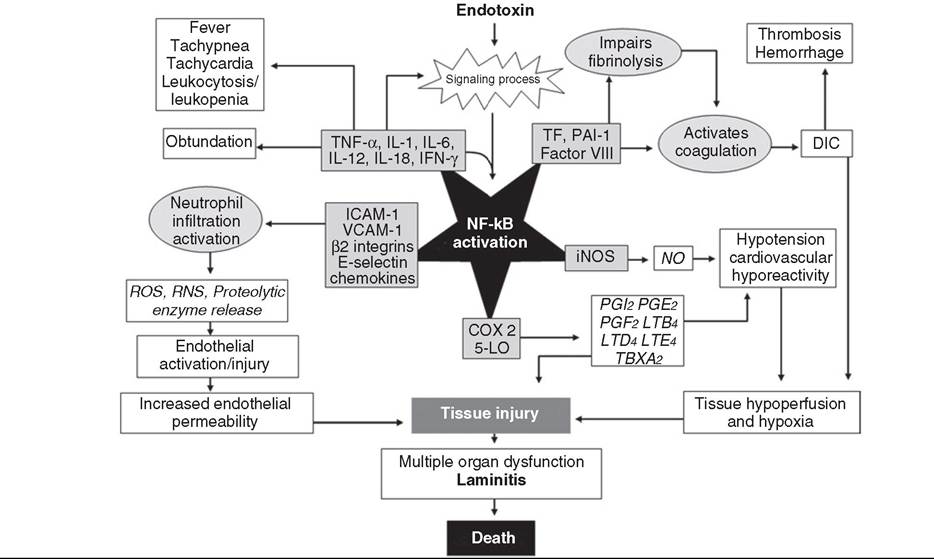
FIG. 32.58 Nuclear factor κB signaling plays a central role in the pathophysiology of septic shock. COX 2, Cyclooxygenase 2; DIC, disseminated intravascular coagulation; ICAM-1, intercellular adhesion molecule 1; IFN, interferon; IL, interleukin; iNOS, inducible nitric oxide synthase; 5-LO, 5-lipoxygenase; LT, leukotriene; NO, nitric oxide; PAI-1, plasminogen activator inhibitor 1; PG, prostaglandin; RNS, reactive nitrogen species; ROS, reactive oxygen species; TBXA2, thromboxane 2; TF, tissue factor; TNF, tumor necrosis factor; VCAM-1, vascular cell adhesion molecule 1. (Modified from Liu S, Malik A. NF-kappa B activation as a pathological mechanism of septic shock and inflammation. Am J Physiol Lung Cell Mol Physiol 2006;290:L622-L645, Fig. 3.)
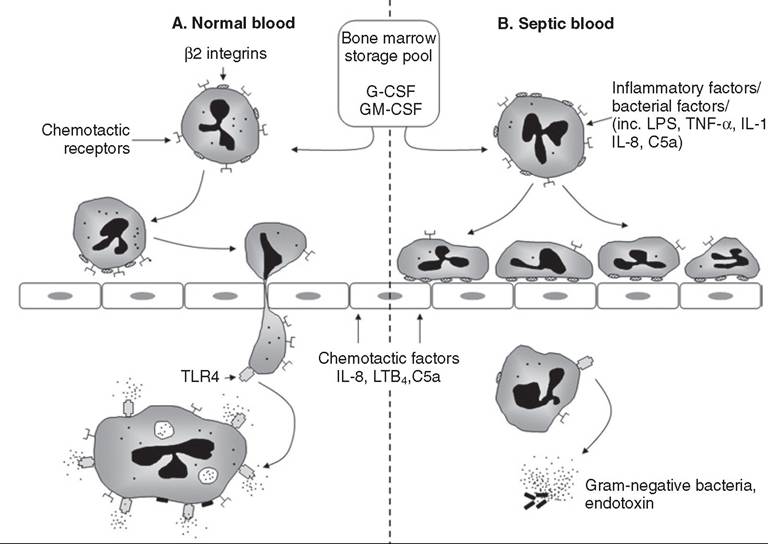
FIG. 32.59 Recruitment and activation of neutrophils in response to bacterial infection in healthy horses and septic or endotoxemic horses. In response to bacterial infection, cytokines are generated that induce the release of neutrophils from the bone marrow. In the normal state, large numbers of blood neutrophils enter sites of bacterial infection by first adhering to the activated endothelium of local postcapillary venules before migrating up a concentration gradient of chemotactic factors. Endotoxin is bound to Toll-like receptor 4 (TLR4), and bacteria are eliminated by phagocytosis. In patients with endotoxemia or sepsis, high levels of circulating inflammatory factors promote upregulation of surface integrins to promote firm endothelial adhesion to postcapillary venules. However, some of these factors also downregulate the expression of chemotactic receptors. Consequently, neutrophils are strongly bound but less responsive to underlying chemotactic factors. C5a, complement component 5a; G-CSF, granulocyte colony-stimulating factor; GM-CSF, granulocytemacrophage colony-stimulating factor; IL, interleukin; LPS, lipopolysaccharide; LTB4, leukotriene B4 TNF-α, tumor necrosis factor α. (Modified from Brown K Brain S, Pearson J, et al. Neutrophils in the development of multiple organ failure in sepsis. Lancet 2006;368:157-169, Fig. 2.)
In the presence of neutrophil granule myeloperoxidase and H2O2, highly toxic hypochlorous acid is formed on the endothelial surface. Superoxide anion generated as part of the neutrophil respiratory burst also reacts with nitric oxide (a reactive nitrogen species [RNS]) from endothelial cells to yield reactive peroxynitrite radicals (another RNS). Other potentially corrosive substances are contributed by neutrophil granules and include elastase, serine proteases, matrix metalloproteinases, and defensins. In addition to direct damage caused by membrane lipid peroxidation, ROSs and RNSs indirectly stimulate the expression of multiple inflammatory, procoagulant, and vasoactive mediators through activation of NF-κB in both neutrophils and endothelial cells.51 Mediators such as bradykinin, plateletactivating factor, C3a, C5a, and leukotriene B4 directly increase vascular permeability by promoting active retraction of endothelial cells via phosphorylation of the light chain of nonmuscle myosin.51 Vascular leak then facilitates the movement of these potentially harmful substances into tissues.
In health, the antithrombotic phenotype of endothelial cells is maintained by the presence of low amounts of prostacyclin (prostaglandin I2) and nitric oxide, and surface expression of thrombomodulin, protein S and protein C complex, and tissue plasminogen activator.81 During endotoxemia, endothelium supports extrinsic pathway activation because of leukocyte- induced physical damage, expression of the procoagulant tissue factor, downregulation of antithrombin-III and protein C, and inhibition of fibrinolysis through expression of plasminogen activator inhibitor 1.82-84 Additional procoagulant effect may be provided by deposition on the endothelial surface of all of the components of the intravascular coagulation system. Microvascular perfusion is further compromised by sepsis- associated increase in “stiffness” of both RBCs and WBCs,85 which renders such cells less able to deform and squeeze through narrow capillaries.
The effect of endotoxemia and sepsis on vascular tone depends on the stage and severity of disease and the particular organ (vascular bed) considered. Neuroendocrine responses to sepsis lead to the upregulation of predominantly pressor mediators including arginine vasopressin, angiotensin II, serotonin, epinephrine, and norepinephrine. Inflammatory mediators are a mix of vasoconstrictors (thromboxane A2, endothelin, C3a, C4a, C5a) and vasodilators (prostaglandins E2 and I2, adenosine, bradykinin, nitric oxide). In animals with serious sepsis, balances of constricting and dilating influences unique to each vascular bed, loss of vasoregulatory tone, and refractoriness of damaged endothelium to vasoactive substances causes maldistribution of blood flow among organs and systemic hypotension.
Because of poor perfusion pressure, direct microvascular injury, thrombosis, and loss of endothelial integrity (capillary leak), ischemia and hypoxia of organs and tissues occur.33 In fact, the fundamental event in serious sepsis is the development of global tissue hypoxia, perhaps also complicated by dysoxia.5 Global tissue hypoxia results when systemic oxygen delivery fails to meet the oxygen requirements of tissues, and dysoxia results when tissues are unable to effectively utilize delivered oxygen. During serious sepsis, widespread microvascular and mitochondrial injury decrease oxygen delivery and consumption at the cell, tissue, and organ levels.51,86,87 Oxygen delivery to tissues is a product of cardiac output and oxygen content (which itself is a product of hemoglobin oxygen saturation and hemoglobin concentration). Systemic oxygen delivery multiplied by the percentage of oxygen extracted (normally ≤25%) by the tissues is the systemic oxygen consumption. The balance between systemic oxygen delivery and consumption is reflected by the mixed venous hemoglobin oxygen saturation (SVO2). SVo2 has been shown in other species to be a useful surrogate for cardiac index as a target for goal-directed therapy.88 Central venous oxygen saturation, measured through a central venous line, is a reasonable and easily measurable substitute for SVO2 (which must be measured via a Swan-Ganz catheter).
Various hemodynamic combinations may create a systemic imbalance between tissue oxygen supply and demand52,89:
• Hypovolemia. Because of decreased preload caused by hypovolemia, concomitant left ventricular dysfunction, and reflex systemic arterial vasoconstriction, early endotoxemia is often characterized by low cardiac output (i.e., hypodynamic circulatory insufficiency).
• Compensated but maldistributedperfusion. After fluid-electrolyte resuscitation, compensatory mechanisms and low afterload drive transition to a hyperdynamic state. Even with normal or increased cardiac output, perfusion abnormalities may persist because of regional hypoperfusion associated with derangements in blood flow distribution, loss of vasoregula- tory control to vascular beds, and endothelial dysfunction.90 This state is often described as distributive shock.
Myocardial depression secondary to effects of inflammatory mediators and apoptosis of cardiomyocytes is the predominant cause of death in severe sepsis and septic shock.91 Myocardial injury—as indicated by increased cardiac troponin concentrations—was reported in horses undergoing emergency abdominal surgery,92 which suggests that similar pathologic processes probably develop in horses with sepsis and SIRS.
• Increased metabolic demands. SIRS increases metabolic demands, as evidenced by increased splanchnic and total body oxygen consumption.
• Impaired oxygen utilization. The bioenergetics of cellular extraction and use, as well as respiration, may be abnormal at least partially because of mitochondrial dysfunction.51,86,87
The effects of these hemodynamic derangements on clinical measures cardiovascular function and perfusion are detailed in Table 32.8.
In summary, the pathophysiologic mechanisms of early sepsis are currently thought to support development of a self-perpetuating imbalance in the systemic redox state, which results in oxidative stress that is believed to be at the root of SIRS and resultant organ dysfunction in sepsis.51,86,87 Activation of local and systemic inflammatory responses results in production of ROS and RNS, which can directly and irreversibly damage cells and inhibit normal cellular activity, as described previously. In health, ROS and RNS production is tightly regulated by inducible antioxidant enzymes, production of which is regulated by the nuclear transcription factor Nrf2.51 However, Nrf2 activity is impaired by excessive ROS and RNS production, which results in less activation of these antioxidant pathways and the generation of an overall oxidant environment.51 Mitochondria are a key source of ROS and RNS but are also very sensitive to oxidative injury. Mitochondrial dysfunction and oxidative stress can result in tissue dysoxia and organ failure, as well as further stimulate inflammatory responses and NF-κB activation, creating the vicious cycle characteristic of SIRS and MODS.
■ TABLE 32.8
Effect of Hemodynamic State on Parameters of Cardiovascular Function
| Pathologic State | MAP | CVP | ScVO2 | Lactate | CO | SVR |
| Hypovolemia | Variable | I | I | ↑ | I | ↑ |
| Compensated but maldistributed | Normal to ↑ | Normal | ↑ | Normal to ↑ | ↑ | I |
| Myocardial depression | Variable | ↑ | I | ↑ | Normal to I | Normal to ↑ |
| Increased metabolic demand | Variable | Normal | I | Normal to ↑ | Variable | Variable |
| Impaired O2 usage | Variable | Normal | ↑ | ↑ | Variable | Variable |
CVP, Central venous pressure; CO, cardiac output; MAP, mean arterial pressure; ScVO2, central venous oxygen saturation; SVR, systemic vascular resistance. Adapted from Otero R, Nguyen H, Huang D, et al. Early goal-directed therapy in severe sepsis and septic shock revisited: concepts, controversies, and contemporary findings. Chest 2006;130:1579-1995.
Immunosuppression in Late Sepsis
It has become apparent that many horses with sepsis are profoundly immunosuppressed, as evidenced by lymphopenia, anergy, and susceptibility to opportunistic infections51,52,93 (e.g., pulmonary aspergillosis in horses with enteric salmonellosis94,95). This immunosuppression, termed the compensatory antiinflammatory response syndrome (CARS), has been explained by the reactive production of antiinflammatory mediators in response to the cytokine storm.96 Although many such mediators are produced and actually can have favorable antiinflammatory effects when used as therapy in models of sepsis, it is now clear that three additional and primary mechanisms involving both innate and adaptive immune responses contribute to sepsis-associated immunosuppression: (1) widespread apoptotic death of lymphocytes (particularly B cells and CD4+ T-helper cells) secondary to activation of intracellular caspases; (2) dendritic cell loss and dysfunction, which leads to inefficient or impaired antigen presentation; and (3) impaired phagocyte 51939798
chemotaxis and killing responses. ’’’ Of interest is that macrophages and neutrophils are spared premature apoptotic death; neutrophils actually are prevented from physiologic apoptosis during sepsis and remain viable in sequestered sites.79 In humans with sepsis, aspects of this immunosuppression are characterized by loss of cutaneous delayed-type hypersensitivity responses,51 but this has not been investigated in horses to date. The relationship and interplay between SIRS and immunosuppression in sepsis is still unclear, and these phases may not always occur sequentially in the same patient.
■ Signs of Endotoxemia and Sepsis
CLINICAL SIGNS. In horses given intravenous endotoxin experimentally, the clinical signs may range from fever without obvious malaise to multiple organ failure and death. Obviously, signs of the primary disease resulting in endotoxemia (e.g., severe pain caused by intestinal strangulation or diarrhea in horses with Salmonella colitis) may greatly influence the overall clinical presentation of horses with naturally acquired endotoxemia. The clinical signs of polymicrobial or Gram-positive sepsis are generally indistinguishable from the signs associated with endotoxemia/Gram-negative sepsis described later.46,47,99,100 Typically, in an adult horse given a moderate sublethal dose of endotoxin intravenously (e.g., 0.1 to 1 μg of LPS per kilogram of body weight), an early period of mild tachypnea peaks within 30 minutes and resolves within 2 hours. During this period, mucous membranes are pale. Beginning within 90 minutes after LPS injection, depression, restlessness, and inappetance are present and rectal temperature begins to rise. Auscultable intestinal sounds usually cease during this period and remain depressed for several hours. Intermittent signs of colic usually are seen, including recumbency (usually without rolling). Small amounts of loose feces usually are passed. The heart rate peaks during the stage of maximal abdominal discomfort (approximately 2 hours after administration of endotoxin) and then temporarily declines. During this time, mucous membranes become congested, the capillary refill time is prolonged, and a dark “toxic” line may become apparent around the gingival margins of the teeth. Beginning 4 to 6 hours after endotoxin administration, there is a secondary phase of tachycardia and tachypnea that is probably related to development of systemic hypotension and fever. This secondary phase persists for several hours. Horses that present clinically with mild to moderate endotoxemia or sepsis usually resemble experimental animals during the period 2 to 6 hours after intravenous endotoxin administration.
At higher LPS doses (e.g., 100 μgZIibuprofen, platelet-activating factor antagonist, elastase inhibitor, nitric oxide synthase inhibitor, antithrombin III (AT-III), tissue factor pathway inhibitor, and drotrecogin alfa (activated protein C).108 It is clear that most experimental sepsis models do not replicate naturally occurring sepsis, at least as it occurs in humans and probably in horses. Even among sepsis models, results for the same candidate treatment are often inconsistent. For example, neutralization and inhibition of inflammatory cytokines such as TNF-α usually have salutary effects in LPS-infusion experiments; however, equivalent studies involving the cecal ligation-puncture model in mice (widely considered to be one of the best experimental sepsis models) usually have shown either neutral or negative
109
effects on mortality.109
Several of many plausible explanations for the disparity among and between the results of experimental, single-center, and large clinical studies are (1) heterogeneity of presentations among enrollees in clinical studies; (2) diversity in genetic susceptibility to sepsis among outbred populations; (3) differences between experimental and clinical study species; (4) differences in timing of potential treatments in relation to the onset of sepsis between the two study populations; and (5) a preponderance of immunosuppressive states in naturally occurring sepsis, in comparison with the “cytokine storm” of early sepsis usually re-created in experimental models.
Fortunately, there is powerful evidence to support the use of early aggressive cardiovascular resuscitation in sepsis management in clinical settings. Previous work in humans documented a reduction in in-hospital mortality from serious sepsis, from 46.5% in the group that received standard therapy to 30.5% in the group that received early goal-directed therapy (EGDT; Fig. 32.60): oxygen, fluids, pressors, inotropes, and packed RBCs during the first 6 hours after admission to achieve a sequence of physiologic goals.110 However, more recent studies have demonstrated conflicting results, with some failing to demonstrate any benefit of EGDT over standard therapy.111-113 In view of the constant improvements in standard of care in human medicine, it seems possible that reaching the specific physiologic goals laid out in EGDT protocols is less important than general aggressive cardiovascular support and close monitoring during initial stabilization. Comparable aggressive cardiovascular resuscitation protocols for equine patients with SIRS, sepsis, and septic shock are detailed in the next section.
Improvements in cardiovascular support of horses with sepsis will continue to be of much more value than any single therapeutic agent available now or in the future. In fact, because clinical sepsis probably is almost always caused by multiple pathogen and host-derived DAMPs stimulating multiple, complementary, and redundant inflammatory pathways, management of sepsis is much more likely to be successful when therapy focuses on combatting the clinical sequelae of severe SIRS and subsequent immunosuppression rather than targeting a specific inflammatory mediator or PAMP. A prioritized strategy for management of horses with sepsis or endotoxemia should include (1) cardiovascular resuscitation; (2) laminitis prevention; (3) removal of the causes of sepsis; (4) neutralization of circulating endotoxin or other PAMPs; and (5) inhibition of PAMP-induced inflammation.
CARDIOVASCULAR RESUSCITATION. Expansion of blood volume remains the cornerstone of treatment for horses with SIRS/sepsis/endotoxemia. Most cases can be treated successfully with intravenous balanced polyionic solution according to guidelines for estimating water deficits provided in the Fluid Therapy for Horses with Gastrointestinal Diseases section of this chapter. Urination should begin during the rapid replacement of estimated losses. Ideally, the fine control of fluid replacement is based on clinical evidence of blood volume and perfusion (e.g., mucous membrane color, heart rate, capillary refill time, pulse quality, jugular refill time, extremity temperature), as well as serial measurements of packed cell volume (PCV) or plasma protein concentration and blood lactate concentration. Some clinicians prefer the early use of compatible plasma (20 to 40 mL/kg) to replace the extravasated colloid lost as a result of vascular leak. Plasma has the advantage of providing immunoglobulin, acute-phase proteins, and anticoagulants and can provide antiendotoxin antibodies (described later). Synthetic colloids such as 6% hetastarch (hydroxyethyl starch solution) were advocated as excellent colloid replacement in sepsis and septic shock because of their superior oncotic activity. However, studies have demonstrated impairment of hemostasis and development of acute kidney injury in septic patients receiving some synthetic colloids, and the use of 6% hetastarch is now considered contraindicated in human sepsis.114
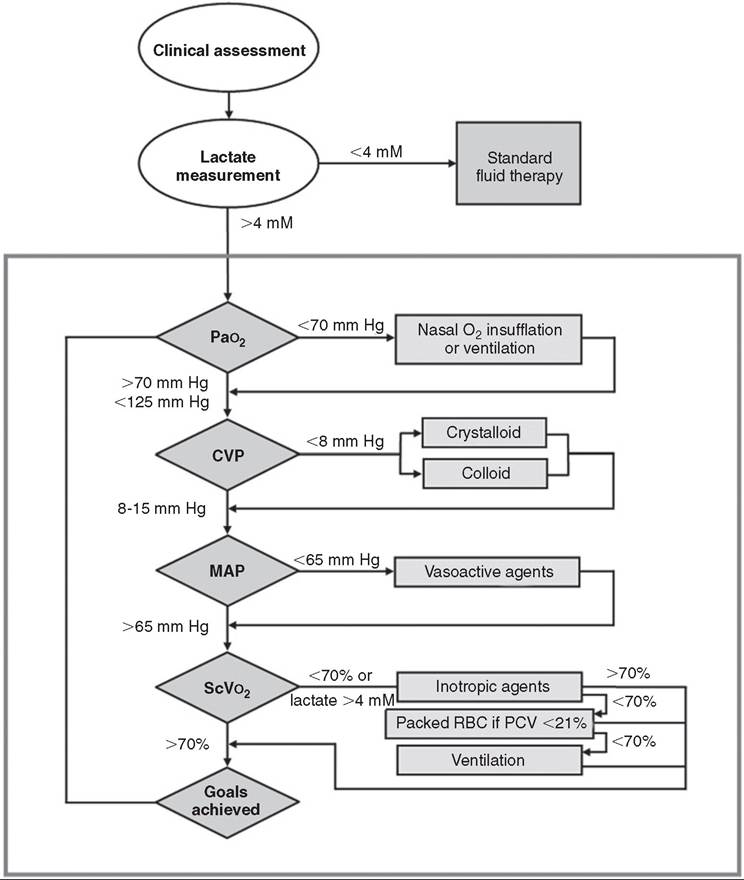
FIG. 32.60 Protocol for early goal-directed therapy. An initial 20-mL/kg bolus of isotonic crystalloid (or equivalent colloid) is given, followed by boluses of 10 mL/kg every 30 minutes until central venous pressure (CVP) reaches 8 to 15 mm Hg. If adjusted mean arterial pressure (MAP) at the heart base is still less than 65 mm Hg, vasopressors are given to effect. Norepinephrine, dopamine, or vasopressin can be used according to the clinician’s preference. If the central venous oxygen saturation (ScVθ2) is still less than 70%, the continuous-rate infusion of dobutamine can be increased in increments up to 15 μg∕kg∕min. If the packed cell volume (PCV) is less than 21% after the preceding steps and ScVθ2 is less than 70%, packed cells should be given to increase oxygen-carrying capacity. PaO2, Partial pressure of arterial oxygen; RBC, red blood cells.
In horses with severe sepsis, septic shock, or MODS, aggressive hemodynamic stabilization and monitoring is indicated. Owners should be informed that such treatment still carries at best a guarded prognosis for survival, substantial financial commitment, transfer to a referral center, and great risk of potentially life-threatening complications such as laminitis. However, early and aggressive intervention is essential in sepsis therapy; in critical care parlance, terms such as the “golden 6 hours” and the “silver 24 hours” exemplify this concept.89
Specific and critically evaluated guidelines for initial resuscitation and stabilization in equine sepsis are not available, but much has been extrapolated from human critical care. Initial fluid resuscitation should include a balanced polyionic crystalloid at 20 mL/kg as an intravenous bolus followed by reassessment of hemodynamic parameters; fluids with high chloride levels such as 0.9% sodium chloride should be avoided. Boluses of 10 to 20 mL/kg should be repeated until hemodynamic improvement is reached or three or four boluses have been given (total, 60 to 80 mL/kg).115,116 Both clinical and clinico- pathologic parameters should be monitored and at minimum should include heart rate, body temperature, mentation, capillary refill time, peripheral pulse quality, warmth of extremities, peripheral lactate, partial pressure of arterial oxygen, and mean arterial pressure (MAP). Central venous pressure (CVP) and central venous oxygen saturation can also be measured to guide resuscitation if suitable equipment is available.117 Hypoxemic patients should receive nasal oxygen insufflation, and ventilation may be needed for severely hypercapneic or hypoxemic patients. Steady improvement in these parameters with return to reference values within the first 6 to 8 hours of therapy is ideal but not always possible. If the patient is still not improved after three or four fluid boluses, as mentioned, and oxygen/ventilatory support, additional therapy with colloids (plasma, or whole blood if anemia is also present), inotropes, vasopressors, or a combination of these should be considered.
Once the patient is stabilized, fluid management should continue according to standard protocols (see the Fluid Therapy for Horses with Gastrointestinal Diseases section) with adjustments made according to the results of continued monitoring of clinical signs of blood volume status and perfusion, blood acid-base status, partial pressure of arterial oxygen, central venous oxygen saturation, lactate, CVP, and MAP. If the blood bicarbonate concentration is less than approximately 16 mmol/L after volume restoration, sodium bicarbonate should be given IV to replace calculated deficits. During correction of acidemia, intravenous fluids should be supplemented with potassium (10 to 20 mmol/L) to prevent correction-induced hypokalemia. A maintenance-rate infusion of glucose should be given to neonates with sepsis (4 mL of 5% dextrose-containing fluids per kilogram per hour) and hypoglycemic adults (2 mL of 5% dextrose or 0.2 mL of 50% dextrose per kilogram per hour). Glucose concentration should be regularly monitored, and the use of concurrent insulin therapy should be considered in persistently hyperglycemic animals.
LAMINITIS PREVENTION. Adult horses with sepsis are at high risk for the development of laminitis. Among the clinical risk factors that are probably operative in the setting of sepsis are underlying endocrine disease, previous episodes of laminitis, a period of 24 hours or longer since onset of signs of endotoxemia or sepsis, fever, prolonged central reaction time, and cold extremities. The digital laminae are probably injured early in sepsis, potentially irreversibly, by processes associated with the cytokine storm and resultant global tissue hypoxia. Insulin resistance, hyperglycemia, microvascular injury and thrombosis, and protease activation all may also be involved in the pathogenesis of sepsis-associated laminitis. There is no ideal laminitis prevention strategy that is universally effective, but according to the current understanding of laminitis pathophysiology, a combination of prompt fluid resuscitation to restore appropriate digital perfusion, NSAIDs to decrease inflammatory mediators, and digital cryotherapy is generally accepted as the minimal standard of care, and some evidence supports their use in equine sepsis., Laminitis prophylaxis must be implemented very early (preferably before an increase in digital pulses is detected) and is not universally protective.
The use of insulin infusions in septic horses may also be indicated to combat persistent hyperglycemia associated with sepsis-mediated insulin dysregulation, inasmuch as insulin dysregulation is associated with endocrinopathic laminitis. However, because insulin infusions at very high rates have been associated with laminitis development in healthy horses and ponies120,121 and hyperinsulinemia is associated with endocrinopathic laminitis,122 glucose or insulin infusions could possibly potentiate the development of laminitis in susceptible animals with sepsis. The use of insulin-sensitizing drugs such as metformin or pioglitazone could have potential in treating sepsis-mediated insulin dysregulation in horses, but to date these drugs have not been examined in clinical equine sepsis; current evidence suggests that their effects on insulin sensitivity in horses may be variable at best.123-125 If laminitis is already present, or if it develops during the course of treatment, it should be treated as described in Chapter 38.
REMOVAL OF THE CAUSE OR CAUSES OF ENDOTOXEMIA AND SEPSIS. Removal of the cause of sepsis usually involves both removal of the source of endotoxin or other microbial PAMPs, as well as correction of the abnormality that allows endotoxin or other PAMPs to enter the blood. In some cases, the source can be mechanically removed; for example, bacteria and associated inflammatory effusion can be drained from pleural or peritoneal cavities or lavaged from the postpartum uterus. Early and appropriate antimicrobial therapy also is essential. In general, broad-spectrum bactericidal drugs should be selected because septic horses may be immunosuppressed. In horses in which endotoxemia or sepsis is associated with diarrhea or other signs of colitis or typhlitis, the use of antimicrobial drugs is controversial because of their causal association with severe colitis. Antimicrobials should probably should be given to equids with colitis only in the following situations: (1) The affected horse is younger than 6 months of age; (2) clostridial or antimicrobial-associated enteritis is suspected (use of metronidazole should be considered); (3) the horse has a severe degenerative left shift or severe leukopenia with total neutrophil count of less than 1000 μg∕mL; (4) the horse has concurrent peritonitis; or (5) the horse shows clinical evidence of dyshemostasis (e.g., jugular thrombosis or abnormal coagulogram). However, these recommendations and outcomes after treatment of equine colitis with and without antimicrobials have not been critically evaluated to date. Furthermore, effective antimicrobial therapy could temporarily worsen clinical signs by causing the release of endotoxin from killed bacteria. This possibility should be anticipated and minimized by the timely use of NSAID or other antiendotoxic therapy (see later discussion).
When intestinal strangulation is the cause of sepsis, surgical correction obviously is of paramount importance. For the purposes of perioperative management, however, it should be noted that resumption of intestinal blood flow could worsen endotoxemia and sepsis: Sequestered endotoxin and other microbial components may be flushed into the circulation through compromised intestinal walls. At least in the case of small intestinal ischemia, the mucosal barrier to endotoxin may be further compromised by ischemia-reperfusion injury when full blood flow is restored by luminal decompression or other manipulation. Prophylactic or intraoperative administration of NSAIDs, ROS scavengers, polymixin B, hyperimmune plasma or serum (as described later), or a combination of these before or immediately after correction of a strangulating intestinal lesion may be warranted.
NEUTRALIZATION OF CIRCULATING ENDOTOXIN
Hyperimmune Plasma and Serum. An antiserum (Endoserum; Immvac Inc., Columbia, Mo.) and several hyperimmune plasmas (e.g., Equiplas-J, Plasvacc, Templeton, Calif.) produced by immunization of horses against R-mutant endotoxins are used in horses with suspected endotoxemia (in some cases, this is an off-label use). As is the case with studies in humans and small experimental animals, use of cross-reactive endotoxin antibodies in horses with either experimentally or naturally acquired endotoxemia has yielded conflicting results. Several studies demonstrated impressive reduction of mortality rate or improvement in clinical signs when antiendotoxin serum or plasma was given to horses126-128; in other studies, however, no improvement was demonstrated.129,130 Pretreatment of foals with antiserum was associated in one report with significant worsening of clinical response to IV administered endotoxin in comparison with foals that received no pretreatment.131 These disparate results probably reflect, at least in part, variation in the quality of antisera and experimental conditions; therefore no blanket recommendation can be made as to the clinical use of such products.
As evidence of the potential general value of hyperimmune plasmas, a reduction in mortality was achieved when antiendotoxin plasma raised against the E. coli mutant J5 was given to bacteremic humans (39% for controls versus 22% for those given antiendotoxin plasma) in a masked, well-controlled study at a single hospital.132 In contrast, subsequent large multicenter studies of two different antiendotoxin monoclonals failed to show beneficial effects.133,134 An equine study demonstrated no effect of hyperimmune plasma on clinical parameters or peak plasma TNF-α concentrations in horses undergoing an experimental low-dose endotoxin challenge, although peak plasma TNF-α bioactivity was reduced in horses receiving plasma in comparison with controls.135 This suggests that hyperimmune plasma may contain factors such as soluble TNF-α receptor that could limit the activity of endotoxin-induced inflammatory cytokines. Hyperimmune plasmas (raised against any antigen) also contain colloid, anticoagulant, and increased amounts of substances such as acute-phase proteins, which might have nonspecific beneficial effect in the setting of endotoxemia and sepsis. Therefore the use of 5 to 40 mL of hyperimmune plasma (of any specificity) per kilogram can be justified in treatment of serious endotoxemia or sepsis in horses.
Polymyxin B. Polymyxin B is a broad-spectrum cyclic peptide antibiotic with potent endotoxin-binding activity. Potentially lethal side effects (respiratory paralysis and nephrotoxicity) have precluded use of this agent as a systemic antimicrobial drug; however, polymyxin B retains endotoxinneutralizing capacity at nontoxic dosages. Pretreatment of foals with polymyxin B at a dosage rate of 6000 U/kg significantly suppressed clinical and cytokine responses to intravenous endotoxin without causing toxic side effects.131 Repeated administration to ponies of 15,000 U/kg also produced no sign of toxicity.136 At a dose of 5000 U/kg, polymyxin B provided protection even when given 30 minutes after the start of LPS infusion.137 The results of a pharmacokinetic and pharmacodynamic study of polymyxin B in horses suggested that the drug could safely be given at 6000 U/kg every 8 hours to maintain continuous endotoxin neutralization.138 Lower doses (1000-2000 U/kg) also appear to have anti-TNF-α effects, but for shorter time periods.13',139 Thus in horses with moderate or severe endotoxemia, IV polymyxin B (Polymyxin B sulfate; Bedford Laboratories, Bedford OH) can be given cautiously two or three times daily at a dosage rate of 1000 to 6000 U/ kg. Each treatment should be diluted in saline and infused over at least 15 minutes. However, of importance is that although polymyxin B and the nontoxic polymyxin B-dextran 70 conjugate PMX-622 safely prevented signs of endotoxemia when given before LPS to otherwise healthy horses,137,139,140 the drug has not advanced beyond phase 1 trials in human patients because experimental studies showed that it did not protect mice if given after intraperitoneal administration of endotoxin.141
INHIBITION OF ENDOTOXIN-INDUCED INFLAMMATION AND RELATED SEQUELAE
Nonsteroidal Antiinflammatory Drugs. Through inhibition of COX, NSAIDs reduce the formation of prostanoid metabolites (e.g., thromboxanes and prostaglandins) from arachidonic acid and thereby attenuate much of the adverse effect of endotoxin. Flunixin meglumine, phenylbutazone, ketoprofen, carprofen, meloxicam, firocoxib, and aspirin are examples of this class of drugs used in horses. When flunixin is administered at 0.25 mg/kg every 6 to 8 hours in horses, endotoxin-induced prostanoid production is prevented, and antiendotoxic effects are maximal in experimental situations without obscuring the signs of colic or increasing the risk of toxic side effects of the drug.142 Flunixin, however, does not reduce endotoxin-induced leukopenia. Because there is evidence that aspirin does not prevent endotoxin-induced aggregation of equine platelets,143 there appears to be no rationale for the practice of adding aspirin to the NSAID regimen. Most NSAIDs inhibit constitutive COX-1 activity (in addition to endotoxin-induced COX-2 activity), and so some morbidity is associated with their use. Gastric ulceration, right dorsal colitis, renal papillary necrosis, and possibly impairment of intestinal motility may develop.144,145 Moreover, flunixin meglumine has been shown to slow mucosal healing and increase mucosal permeability by LPS in ischemic-injured equine jejunum,146,147 although similar inhibition of mucosal barrier function does not appear to occur in the equine colon.148 However, concurrent administration of misoprostol (a prostaglandin E1 analogue)149 or
1
a constant-rate infusion of lidocaine150 ameliorated these effects in an equine model, which suggests these drug combinations might be more appropriate than flunixin alone for horses with endotoxemia caused by intestinal ischemia.
In view of this toxic potential of equine NSAID use, it has also been suggested that administration of COX-2-selective drugs may minimize side effects while maintaining efficacy. Three NSAIDs with documented analgesic effect in horses— firocoxib, carprofen, and meloxicam—have been shown to be COX-2-selective.151,152 Etodolac, a COX-2-specific drug in dogs and humans, is not COX-2-selective in horses when used at analgesic doses (23 mg/kg PO once or twice daily).153 Firocoxib and meloxicam do not appear to retard small intestinal mucosal healing or increase LPS permeability in ischemic- injured equine jejunum as flunixin can.146,154 Of importance, however, is that COX-2 activity may also have potentially beneficial effects in horses with sepsis; for instance, COX-2 products (e.g., prostaglandins E2, and I2) mediate epithelial restitution in damaged equine colon144 and are thought to be important in maintaining the antithrombotic phenotype of normal endothelium. NSAIDs in the coxib class, which are potently COX-2 specific, have also been shown to increase the risk of atherosclerotic cardiovascular disease in humans.155 Similar risks for coxibs in horses have not been described, but at present firocoxib and meloxicam are the only drugs in this class labeled for equine use, and neither is yet available globally.
Finally, although various NSAIDs have been shown to effectively prevent the clinical and molecular sequelae of equine endotoxemia in experimental models,83,142,156-163 no study has shown convincingly that NSAIDs actually save lives in human or equine patients with naturally occurring sepsis. A large multicenter, controlled, masked, prospective study of ibuprofen in humans with sepsis syndrome showed no effect of this drug on the development of shock or the acute respiratory distress syndrome, and no improvement in survival.164 Similar studies have not been conducted in horses to date.
Methylxanthine Derivatives. Inflammatory cytokine production by macrophages is suppressed in dose-dependent manner by methylxanthine derivatives. This effect appears to be caused by phosphodiesterase inhibition and consequent elevation of intracellular cyclic adenosine monophosphate. Pentoxifylline, a drug that used widely by humans as a hemorheologic agent, has also been shown to increase RBC deformability in horses.165 Pentoxifylline also inhibits TNF-alpha production in horse blood and in cultured equine macrophages while increasing secretion of prostacyclin.166,167 Studies in other species suggest that pentoxifylline stimulates production of the antiinflammatory cytokine IL-10, suppresses neutrophil activation, and inhibits activation of NF-κB.168 A pharmacokinetic study in horses has indicated that administration at 10 mg/kg PO two times daily provides serum concentrations equivalent to those used therapeutically in humans.169
Finally, intravenous pentoxifylline significantly, albeit only partially, reduced adverse signs in horses given LPS.170 The usefulness of this finding is called into question, however, by the observation that the lethality-sparing effect of pentoxifylline in endotoxemic mice was removed if the drug was given in combination with indomethacin, a potent NSAID.171,172 In this study, the investigators concluded that upregulation of prostacyclin production by pentoxifylline, which was prevented by concurrent indomethacin, reduced mortality in subject mice by preventing endotoxin-induced leukopenia. Of interest is that pentoxifylline alone increased WBC counts in horses, but this effect is prevented by flunixin.167,170 Thus there might be a conceptual and potential beneficial effect of pentoxifylline therapy (10 mg/kg PO bid) in endotoxic horses, although any effect could be partially or wholly neutralized by concurrent NSAID administration (as is commonly done in equine practice).
Corticosteroids. The corticosteroid class of drugs theoretically has many useful actions in combating inflammation in endotoxemia and sepsis. These include reduced production of cytokines, inhibition of TNF-alpha production by macrophages, stabilization of cell membranes, and prevention of neutrophil activation. It is surprising, however, that neutral or negative effects of moderate or high-dose steroid use were found in large, multicenter studies of humans with Gram-negative sepsis,173 probably in relation to immunosuppressive effects at these doses. Corticosteroids also are widely believed to increase susceptibility to laminitis in endotoxemic horses, perhaps by increasing the sensitivity of digital vessels to the constrictive actions of circulating catecholamines or by inducing insulin resistance and hyperglycemia.174 Use of high-dose corticosteroids is currently contraindicated in the treatment of endotoxemia or sepsis in humans and horses.
Some human patients with sepsis appear to respond to low “physiologic” doses of hydrocortisone.174-178 Most such patients have high baseline cortisol concentrations but are thought to be in a state of adrenal insufficiency termed critical illness-related corticosteroid insufficiency (CIRCI), a syndrome that also appears to occur in some septic neonatal foals and some horses with systemic illness and SIRS.41,179-181 Low-dose hydrocortisone is associated with reduced need for vasopressor use and lower mortality rates in humans with septic shock, according to a number of reports,175,176,182-184 but other studies have not demonstrated a beneficial effect.185 At present, low-dose hydrocortisone therapy is recommended for humans with sepsis who meet criteria for CIRCI but not universally for all septic patients.183 The use of low-dose hydrocortisone therapy has not yet been reported in septic equine patients, but a 3.5-day tapering regimen of low-dose hydrocortisone (1.3 mg/kg/day divided q4h IV) administered to healthy neonatal foals was shown to ameliorate LPS-induced inflammatory cytokine production from peripheral blood leukocytes without impairment of neutrophil function in an ex vivo model.186
Anticoagulant Therapy. The use of anticoagulants such as heparin in horses with endotoxemia is somewhat controversial. Heparin prevents microvascular thrombosis principally by promoting the anticoagulant activity of AT-III. Unfortunately, heparin cannot reverse existing thrombosis, and because AT-III is consumed during severe coagulopathy, it may not prevent additional intravascular coagulation in such cases. Fresh and fresh-frozen plasma are good sources of AT-III but also provide clotting factors that could potentiate intravascular coagulation. When given at the recommended intravenous or subcutaneous dose of 40 U/kg tid (fresh plasma) or 150 U/kg bid (fresh-frozen plasma), unfractionated heparin causes intravascular agglutination of equine RBCs.187 Therefore it could be argued that the use of heparin might actually exacerbate intravascular cellular plugging, which is theorized to play a role in some cases of laminitis in equine sepsis. This side effect can be avoided with the use of low-molecular-weight heparin (LMWH), which is nonagglutinating but retains anticoagulant activity, principally via inhibition of factor Xa.188 Two clinical studies have suggested that LMWH may have benefits over unfractionated heparin in the prevention of jugular thrombosis or laminitis in some 189190
equine patients with colic,189,190 but this suggestion is not universally accepted. The use of heparin could be considered in horses with sepsis that have evidence of hypercoagulation syndrome (early evidence of dyshemostasis such as abnormal coagulogram or spontaneous venous thrombosis), or possibly in those that are at high risk for laminitis (e.g., DPJ, colitis, or grain overload). In general, heparin should be given with plasma (10 to 40 mL/kg) at a dose of either 200 to 300 IU/ kg/day for unfractionated heparin (either divided bid-tid IV or SC or as a continuous intravenous infusion) or 50 IU/kg for LMWH (SC sid). Foals at risk for thrombosis may require a higher dose of LMWH, in the range of 100 IU/kg.191
Other anticoagulants that inhibit platelet function, including clopidogrel and aspirin, have also been evaluated in horses and are sometimes recommended in equine sepsis. Both clopidogrel (4 mg/kg PO once for loading dose and then 2 mg/ kg PO q24h) and aspirin (5-10 mg/kg PO q24-48h) appear to be effective anticoagulants in horses by inhibiting platelet activation 192-194; however, aspirin's effects are irreversible, which could be problematic if surgery or invasive diagnostic testing is required during sepsis treatment. Clopidogrel has been evaluated in horses with experimental endotoxemia, and attenuation of LPS-induced tachycardia was noted, but specific LPS-induced platelet hyperreactivity was not seen.194
Scavengers of Reactive Oxygen Species. ROSs are thought to cause corrosive tissue damage during endotoxemia and potentiate the production of inflammatory cytokines through activation of NF-κB. Surgical deflation of distended small intestine is thought to lead to ischemia-reperfusion injury, a process that generates ROSs from epithelial xanthine oxidase. The life-saving and necessary process of fluid resuscitation in horses with septic shock may even lead to whole-body ischemiareperfusion and systemic release of ROSs. Despite these key associations between oxidant stress and sepsis, little effort has been made to intervene therapeutically at this level.
There is some evidence that allopurinol, a hydroxyl radical scavenger and inhibitor of xanthine oxidase activity, has positive clinical effect during sublethal endotoxin infusion in horses.195 A recommended dose for allopurinol is 5 mg/kg IV. Because dimethyl sulfoxide (DMSO) has been shown to be a potent scavenger of hydroxyl radicals with efficacy in rodent sepsis models,196 it has been considered for use in the treatment of equine endotoxemia, although effects in experimental models have been variable. DMSO is typically administered by rapid intravenous infusion (or by nasogastric tube) as a 10% to 20% solution in saline at dose of 0.02 to 1 g/kg every 6 to 12 hours. However, intravenous infusion of DMSO at the low and high ends of this dose range was recently shown to have little to no effect on clinical signs (with the exception of fever at the high dose), on clinicopathologic abnormalities, and on TNF-α production after endotoxin infusion in horses.197 At high concentrations intravascularly, DMSO can cause hemolysis.
Ethyl pyruvate, a stable analog of pyruvate, has been shown to have remarkable protective efficacy in a variety of models of septic and nonseptic shock in rodents and other species; its beneficial actions are ascribed to its antioxidant effects.198 Because this agent is inexpensive and can be given in intravenous crystalloid fluids, it could have potential for the treatment of endotoxemia and sepsis in horses. Reports about equine experimental endotoxemia support this theory, demonstrating beneficial effects on clinical manifestations of endotoxemia (except fever) and suppression of proinflammatory gene expression.199-201 Use of ethyl pyruvate in clinical cases of equine sepsis or endotoxemia is not described to date, and other antioxidants that have shown benefit in rodent sepsis models and are considered for use in some human patients with sepsis (e.g., vitamin C, vitamin E, and A-acetylcysteine) have not been evaluated in equine sepsis.
MISCELLANEOUS TREATMENTS. A number of other treatments for endotoxemia and sepsis have been described in horses and other species, though on the whole, currently available data are less supportive of their use in clinical cases. Naloxone, a narcotic antagonist, at a dose of 0.2 mg/kg, blunted some of the cardiovascular effects of high-dose endotoxin in one study,202 but a dose of 1 mg/kg had no effect in another.203 Of importance, 0.75 mg/kg naloxone caused signs of colic in conscious horses,204 probably by blocking the actions of endogenous β-endorphins at the high affinity μ-receptor. The detergent tyloxapol was remarkably effective in preventing the effects of endotoxin in anesthetized horses.205 The mechanism of antiendotoxic action of tyloxapol is unknown, but the detergent has been shown to have wide-ranging effects on cells and proteins, some of which may preclude its use in clinical cases. For example, the detergent has been shown to inhibit cellular phagocytosis, clearly an important event in innate immunity and sepsis. Also, this agent induces marked hyperlipidemia (lipid levels up to 100-fold higher than in controls) in horses because of interference with lipoprotein metabolism. Similarly, a phospholipid emulsion effectively prevented adverse effects of subsequent endotoxemia; however, the treatment induced hemolysis sufficient to preclude its use in clinical cases.206 A published report207 on the use of the sulfonyl analog of the spin trap molecule alpha-phenyl-A7-tert- butylnitrone suggests that this agent was effective in reducing clinical signs in horses given endotoxin. However, a cautionary note was the observation that in some rodents given the same agent at high doses, the endotoxin-induced mortality rate was actually higher.
Platelet-activating factor inhibitors have been effective anti-endotoxic agents in some species but have not yet shown much positive clinical effect in horses or humans.208 In dogs and other experimental animals, inhibitors of nitric oxide production such as jV3-monomethyl arginine reverse endotoxin- induced (or more probably TNF-alpha-induced) hypotension;209 however, nitric oxide synthase inhibitors generally have no protective effect in sepsis models. Furthermore, nitric oxide production may not be increased in horses with endotoxemia.210 The antifibrotic pyridine compound pirfenidone (5-methyl- 1-phenyl-2-[1H]-pyridone) had no effect on endotoxin-induced clinical signs, leukopenia, or TNF-α production in horses.211 Hyperbaric oxygen therapy also did not appear to have any protective effect on clinical or cytokine changes in experimental endotoxemia in horses.212
Constant-rate infusion of ketamine has been theorized to have beneficial effects in equine endotoxemia after it was shown in vitro to suppress the production of inflammatory mediators by LPS-stimulated equine peritoneal macrophages.213 Constantrate infusion of ketamine at 1.5 mg/kg/h for 320 minutes achieves blood concentrations compatible with this inflammatory effect and has been shown to be safe and nonsedating in horses. However, pretreatment with ketamine had no effect on clinical signs, leukopenia, or inflammatory cytokine in horses after endotoxin infusion.214 The putative antiinflammatory actions of ketamine appear to be mediated by the actions of adenosine on the adenosine A2A receptor215; because the equine adenosine A2A receptor was cloned and characterized pharmacologically, it itself may prove a potential direct target for antiinflammatory drugs in the future.
FUTURE TREATMENT CONSIDERATIONS. In summary, current research in horses, humans, and experimental animals suggests that a single therapeutic agent with universal benefit in endotoxemia and sepsis will be very hard (or impossible) to find. Most antiinflammatory approaches that show promise in experimental endotoxemia, even if they are aimed at the initiating steps of the inflammatory cascade (e.g., NF-κB activation), do not work consistently in severe sepsis models (e.g., cecal-ligation puncture) or in phase III clinical trials with human patients. A substantial proportion of the morbidity and mortality associated with sepsis may result as much from immunosuppression in the later stages of sepsis as from the cytokine storm in early sepsis. Immunosuppressed patients could be injured further by antiinflammatory therapy, which potentially explains some of the discrepancy between specific therapeutic efficacy in experimental sepsis and that in clinical sepsis. This emphasizes the need for accurate recognition of—and possibly tiered treatment protocols for—the various stages of sepsis. Plasma biomarkers such as adrenomedullin, procalcitonin, C-reactive protein, or high-mobility group box 1 levels have been used to diagnose sepsis, define sepsis 216217 categories, and provide prognostic information in humans,216,217 but a universally reliable biomarker or combination of markers has yet to be identified. Similar markers need to be integrated more fully into equine sepsis diagnosis, staging and management, although several of the aforementioned human biomarkers (e.g., C-reactive protein) do not appear to be useful in equine sepsis diagnosis.115
Some different treatment approaches have the potential to be both effective and affordable. There is some indication that IFN-γ, a cytokine that is pivotal in both innate and acquired immunity, may be beneficial for combatting immunosuppression in bacterial sepsis.218 Il-7, IL-15, and IL-17 may also prevent or modulate immunosuppression in sepsis by preventing leukocyte apoptosis and supporting both innate and adaptive immune function.51,219 There also remains enthusiasm in human critical care for antioxidant strategies aimed at effective means to suppress or scavenge ROSs.51,86,87 In this regard, the remarkable effects of ethyl pyruvate in multiple models of inflammation, which probably mediates through its antioxidant actions, offer considerable promise. So-called “metabolic resuscitation” with a combination of low-dose hydrocortisone, vitamin C, and thiamine appeared to have a beneficial effect on survival in one human study220 and, if truly effective, might be both beneficial and cost-effective in the treatment of equine sepsis. Inhibition of complement activation with anti-C5a antibody show promise in some sepsis models and is currently in clinical trials in humans.51,221 Finally, two of the most exciting possibilities in the distant future are the use of genotyping to target sepsis diagnosis and treatment and the potential use of even gene therapy to transiently transfect host cells in a targeted way 222223 with genes supporting immune and bactericidal function.222,223
Medical Disorders of the Small Intestine and 32.11). A similar temporal and geographic association was reported in two cases of ulcerative duodenitis in yearlings.5 These findings seem inconsistent with a purely peptic insult as the cause for the ulcerative duodenitis. In one report of seven foals with ulcerative duodenitis,6 lesions typically extended into a large area of the proximal duodenum and were characterized by mucosal necrosis, and areas of affected and more normalappearing mucosa were often sharply demarcated. In the foals of that report, no common microbial organism other than E. coli was identified, and a cause for the ulcerative duodenitis was not determined. In most foals with duodenal disease, the lesions were not focal ulcers but rather appeared as more generalized inflammation. The origin of duodenal disease in foals is probably multifactorial and may involve a combination of breakdown of duodenal mucosal defenses, interaction of gastrointestinal peptides, and possible pathogenic agents.7
CLINICAL SIGNS. The signs of ulcerative duodenitis have been classically described like those of gastric ulcer signs but more severe,8 and in many cases, duodenal and gastric ulcers occur simultaneously. The gastric ulceration is probably secondary to physiologic or anatomic obstruction to gastric emptying, tends to be severe (see Color Plate 32.12), and potentially leads to gastroesophageal reflux, esophagitis and ptyalism. Until the gastric ulceration becomes severe, the primary signs of duodenitis can be nonspecific; they include fever, mild to moderate abdominal discomfort, mild obtundation, and diarrhea.
In general, the sequelae of ulcerative duodenitis are more severe than those of primary gastric ulceration. Complications of ulcerative duodenitis include duodenal perforation with peritonitis or adhesions, duodenal stricture with complete or partial obstruction (Figs. 32.61 and 32.62), ascending cholangitis and hepatitis, and ascending pancreatitis.
DIAGNOSIS. Duodenoscopy is the most specific means of diagnosis. An endoscope with at least a 200-cm working length is used in foals up to 6 months of age, and in older foals, a longer endoscope is needed to examine the duodenal mucosa. Because of the size of the stomach and the anatomic configuration of the duodenum in foals, it is usually not possible to advance the endoscope past the duodenal ampulla. Therefore a diagnosis is most readily made when lesions are diffuse or located within the ampulla. Excessive enterogastric reflux of bile through the pylorus is consistent with duodenal dysfunction. Ulceration at the pylorus or pyloric antrum may accompany ulcerative duodenitis and thus provide an indication of potential duodenal involvement.
FIG. 32.61 Proximal duodenum of a 10-month-old horse with a history of chronic poor appetite and condition. The pylorus (P) is at the left. There are two strictures in the duodenum: S1 is orad from the major duodenal papilla, and S2 is aborad from the duodenal papilla. The segment of the duodenum between the strictures is dilated. (Courtesy Dr. MJ. Murray.)
The peritoneal fluid may show signs of inflammation, infection, hemorrhage, or a combination of these, depending on severity of disease. CBC often reveals peripheral blood leukocytosis and hyperfibrinogenemia. Serum chemistry studies may reveal elevations in liver enzymes, particularly biliary system-associated enzymes (γ-glutamyltransferase [GGT], ALP) and serum bile acids. With severe ulcerative duodenitis, survey radiographs of the cranial abdomen may reveal accumulation of fluid within the stomach and gas ascending the biliary ducts.9 If barium contrast medium is placed into the stomach, complete emptying is usually delayed (>2 hours), and an irregular mucosal border may be noted in the descending duodenum. In most cases, however, radiography would not contribute to a diagnosis of duodenal ulcer per se, although duodenal stricture may be noted. If the descending duodenum is to be imaged, the volume of contrast medium placed in the stomach should not exceed 0.5 to 1 L in a foal and 1 to 2 L in a weanling or yearling; otherwise, the proximal descending duodenum will be obscured by contrast medium within the stomach.
TREATMENT. The effectiveness of treatment of ulcerative duodenitis depends on the extent and severity of ulceration and the presence or absence of complications. Treatment objectives are to decrease duodenal inflammation, treat secondary gastric and esophageal ulceration, promote gastric emptying, and treat related problems such as peritonitis. If ulcerative duodenitis is confirmed or even suspected on the basis of clinical signs, treatment should be aggressive.
Inflammation may be an important part in the perpetuation of disease. In acute cases of ulcerative duodenitis, there usually is a pronounced lymphocytic infiltration of the mucosa. In more chronic cases, there is a mixture of neutrophils, macrophages, fibroblasts, and fibrinonecrotic exudate. Definitive antiinflammatory therapy has not been described for these cases, and the use of corticosteroids or NSAIDs is controversial because they may worsen gastric ulcer disease through inhibition of protective prostaglandin synthesis.
Suppression of gastric acid secretion is still an important objective in the treatment of ulcerative duodenitis in foals because most affected foals have gastric ulcers. Initially, acid suppression should be accomplished via parenteral administration of H2
FIG. 32.62 Duodenal stricture (S1) in the horse described for Fig. 32.68.
The diameter of the duodenal lumen at the stricture is only 3 mm. (Courtesy Dr. MJ. Murray.)
antagonists (cimetidine, 7 mg/kg IV q6h, or ranitidine, 1.5 mg/kg IV q8h) or proton pump inhibitors (pantoprazole, 1.5 mg/kg IV q24h). Oral medications are unlikely to be adequately delivered to, or absorbed from, the small intestine in the first days of treatment. Gastric emptying can be enhanced with bethanechol (0.02 mg/kg SC q6-8h or, when the foal can consume orally, 0.35 mg/kg PO q8h). In foals that have severe duodenal disease or that have required surgery, bethanechol has been given for up to 3 months. Once the foal can accept oral medication, it should be treated with the proton pump inhibitor omeprazole at a dose of 4 mg/kg orally once daily in the paste formulation. In the 24 hours after the first dose, acid suppression is incomplete, and maximal suppression of acid secretion is achieved between days 1 and 5.10 Therefore a common practice is to combine an H2 antagonist IV for the initial 2 days of treatment with omeprazole in foals with duodenitis.
Misoprostol is a synthetic prostaglandin E1 analog that has been used successfully in treating ulcerative duodenitis in humans. Doses of 2 to 5 ng'/kg q8-12h can be used in horses, although side effects may include abdominal pain and diarrhea. Sucralfate promotes duodenal mucosal healing in humans.11 The dose of sucralfate that is effective in humans with ulcerative duodenitis ranges from 1 to 2 g two to four times daily. Foals treated for ulcerative duodenitis that do not have impaired gastric emptying should be administered 2 to 4 g of sucralfate three times daily. Sucralfate, however, should not be used as the sole therapeutic agent for ulcerative duodenitis.
Foals with duodenitis must usually be prevented from nursing or eating for 1 to 3 days. During this time, parenteral feeding should be considered. Depending on the age of the foal, administration of parenteral nutrition should provide 40 to 60 kcal/kg/day.
If medical therapy is ineffective or if sequelae of ulcerative duodenitis cause complications, surgical intervention may be required. Gastroenterostomy has been reported to be effective in some cases through bypassing the affected portion of duodenum and allowing for an alternative route for gastric emptying.9 However, short-term survival and long-term quality of life and use are often unsatisfactory. Patients that have a successful surgical outcome require long-term aftercare and usually require long-term maintenance acid suppression and treatment with a prokinetic drug until gastric emptying is normalized. Therefore an owner should be prepared to make a significant time and financial commitment before surgery is considered.
■ Duodenitis-Proximal Jejunitis DPJ, also known as anterior enteritis or proximal enteritis, is a clinical syndrome characterized by inflammation and edema of the duodenum and proximal jejunum, excessive fluid and electrolyte secretion into the small intestine, and, consequently, large volumes of enterogastric reflux. The syndrome of DPJ was first described in 198212 and was more fully characterized in 1987.13 A subsequent report14 described clinical and clinicopathologic parameters in horses with DPJ that differed somewhat from cases in the 1982 report, which suggests that either the cases were of similar etiopathogenesis but of different severity or that the cases were of different etiopathogeneses whose only similarity was the segment of bowel affected. A diagnosis of DPJ is often applied when affected animals exhibit abdominal discomfort, small intestine distention, and excessive enterogastric reflux without obstruction; however, it is unclear whether all of these cases lie along a spectrum of severity of DPJ or whether they are several disease entities that affect the proximal small intestine and that share clinical features. The latter seems more likely.
PATHOPHYSIOLOGY. In horses with DPJ, lesions are consistently found in the duodenum, but the severity and frequency of lesions in the jejunum are variable. Serositis is a consistent finding, characterized by bright red to dark red petechial and ecchymotic hemorrhages on the serosal surface.13 Histologic lesions include hyperemia and edema of the mucosa and submucosa, villous epithelial degeneration, epithelial cell sloughing, neutrophilic pleocytosis, hemorrhages in the muscular layers, and fibrinopurulent exudation on the serosa.
DPJ causes an increase in the volume of duodenogastric reflux, typically 50 to 100 mL/min. This reflux has been considered to result from increased intestinal fluid secretion and decreased motility. Mechanisms of intestinal fluid secretion include passive transmucosal exudation, secondary to mucosal and submucosal inflammation and characterized by a proteinrich fluid secretion, and active fluid secretion, caused by increased cyclic nucleotides and characterized by fluid with a high electrolyte content and low protein content. The components of fluid in the intestines of horses with DPJ have not been characterized, but they probably result from a combination of passive and active secretion. In some horses the hemorrhagic nature of the gastric reflux implies increased capillary permeability of the duodenal mucosa, whereas in other horses the watery nature of the reflux, the presence of serum electrolyte disturbances,15 and the absence of peripheral hypoproteinemia are most consistent with an active secretory process.
Another potential source of the large volume of fluid secreted into the proximal small intestine and flowing back into the stomach is the pancreas. Normally there is periodic orad movement of duodenal contents into the stomach, which has been observed endoscopically and has been documented by collecting gastric contents with and without pyloric obstruction.7 The duodenal contents have a large component of water, sodium, and bicarbonate, as well as bile salts from the liver. These secretions are presumed to originate from the pancreas, as well as the liver, and pathologic features of either of those organs may contribute to the pathophysiologic manifestations in cases of DPJ.
Suppurative cholangiohepatitis has been reported in cases of small intestinal inflammation secondary to DPJ.16,17 The pathophysiologic origins of this observation may be related to an increased luminal pressure in horses with DPJ, which increases the likelihood of intestinal content regurgitation into the bile ducts. It is also possible that horses with DPJ absorb inflammatory mediators or bacterial products from the small intestine via the portal blood flow or systemic circulation.
Although the exact cause of DPJ is not known, several bacteria and toxins have been implicated. C. difficile has been frequently implicated in causing the disease. One prospective study cultured toxigenic species of C. difficile from the reflux of all 10 horses with a diagnosis of DPJ and only 1 of 16 horses with diagnoses of other causes of nasogastric reflux. Of the strains cultured, those in 8 of the 10 horses with DPJ produced both A and B toxins, whereas the those in the remaining 2 produced only toxin B.18 This is significant in that toxin B may cause inhibitory electromechanical disturbances to smooth muscle in the small intestine, which may be a possible cause of ileus in these horses.19 Toxin A has also been shown to promote inflammatory cell infiltration into the smooth muscle layers.20 Influx of neutrophils and release of inflammatory mediators in the intestinal wall activate nitric oxide pathways, which results in inhibition of the enteric nervous system, increases in sympathetic tone, and a subsequent reduction of contractile activity in the gut.21 Experimental intraduodenal inoculation of crude C. difficile toxins in fasting horses resulted in clinical signs of DPJ in 33% of cases; however, all cases had histopathologic changes consistent with DPJ.22 C. difficile can also be cultured from the proximal intestinal tract in horses without evidence of gastrointestinal disease, however, and these strains can produce both toxin A and B.23 C. perfringens and Salmonella spp. have also infrequently been associated with DPJ, but the significance of these pathogens remains unknown.
Feeding practices may be associated with the development of DPJ. In one study, horses with DPJ were fed significantly more concentrate and were significantly more likely to have grazed on pasture than were horses with other types of colic or horses with lameness.24 This may indicate that these horses are exposed to some type of toxin or infectious agent through different types of feed. Fusarium moniliforme has been cultured from the feed of horses with naturally occurring DPJ. Under experimental conditions, F. moniliforme producing fumonisin B1 mycotoxins also caused lesions consistent with DPJ in two horses.25 Neurologic lesions were present in those horses, however, and both died with lesions consistent with equine leukoencephalomalacia. Cantharidin toxins can also cause reddening of the mucosa in the small intestine, as well as excessive gastric reflux,26 and may be a cause of DPJ in some cases. It is possible that this one syndrome has multiple initiating causes and that no one causative agent will ever be definitively identified.
CLINICAL SIGNS AND DIFFERENTIAL DIAGNOSIS. The differential diagnosis for DPJ includes simple or strangulating small intestinal obstructions. Differentiation can be extremely difficult in some cases and may delay surgical intervention in cases of small intestinal obstruction, to the detriment of the patient. The criteria used to discriminate between DPJ and obstructive lesions include degree of pain after reflux, presence of fever, and changes in hematologic parameters and abdominal fluid.
Horses with DPJ have a history of acute-onset moderate to severe abdominal pain, often followed by varying degrees of depression. Nasogastric intubation yields a large volume of enterogastric reflux, which is frequently orange-brown in color, with a fetid odor. Rectal palpation reveals multiple loops of mild to moderately distended small intestine. The initial volume of reflux may range from as little as 4 to 5 L to as much as 32 L. The duration of the reflux may be as short as 24 to 48 hours, but it usually lasts 3 to 7 days. Many affected horses are febrile (rectal temperature higher than 38° C [101° F]) and dehydrated and have injected mucous membranes, prolonged capillary refill time, diminished intestinal sounds, tachycardia (>60 beats/min), and tachypnea.12-15,27,28 Horses with DPJ also tend to have a higher incidence of gastric ulceration than do horses with abdominal pain secondary to other causes.29 Although abdominal pain usually abates after gastric decompression, most affected horses remain depressed, which perhaps is the most consistent and characteristic clinical sign of the disease. If the fluid that accumulates in the proximal intestinal tract is not removed periodically, signs of abdominal pain recur.
Assessments of the degree of small intestine distention and the thickness of the intestinal wall can be useful indicators. Many horses with DPJ have generalized distention of small intestine, but when palpated rectally, the intestine does not feel taut. In many cases of small intestinal obstruction, the bowel is tightly distended on palpation, but this is not universally true. Ultrasonography can be used, both transrectal and transabdominal, to determine the diameter of the small intestine, evaluate contractions, and measure the thickness of the wall of the intestine. With acute obstruction, several segments of small intestine that are 6 to 10 cm in diameter, have no contraction, and have a wall diameter of 3 to 5 mm are visible. With DPJ, small intestinal diameter may be less, and the thickness of the intestinal wall may exceed 6 mm.
Culture of the reflux for Clostridium and Salmonella spp. can be attempted. This can be difficult, however, given the special conditions required for anaerobic cultures, as well as the intermittent shedding of Salmonella spp. into the gastrointestinal tract of normal horses. Also, the large volume of reflux in these cases may dilute the bacterial population to the point at which isolating low numbers of bacteria is difficult.
Clinicopathologic FINDINGS. Clinical laboratory findings include increased PCV and total plasma proteins (hemoconcentration). Abdominocentesis often reveals an elevated total protein concentration in peritoneal fluid and a mild to moderate increase in the peritoneal WBC count (>5000 cells/J.L).27 The peritoneal fluid is usually yellow and turbid, but in severe cases, diapedesis of RBCs occurs, which results in a serosan- guineous color. In abdominal fluid, a total protein concentration above 3.5 g/dL is associated with a poorer prognosis.27 The WBC count in the peripheral blood may be normal, increased, or decreased.13,14 In addition, hypocalcemia, hyponatremia, hypochloremia, hypokalemia, and acid-base alterations have been reported in horses with DPJ.15 An elevated anion gap may be present, secondary to either decreased calcium and magnesium concentrations or increased lactate or albumin concentrations.27 Increases in the anion gap to 15 mEq/L or higher have also been associated with a poor prognosis. Horses with enteritis have been found to have higher plasma D-dimer concentrations and more severe coagulopathies on admission than do horses with other types of colic.30
Activity of liver enzymes, particularly GGT, may be elevated in horses with DPJ, and such elevation may be a useful way to help differentiate between DPJ and strangulating lesions of the small intestine.16,17 According to a retrospective study of a large series of DPJ cases to determine the prevalence of hepatic damage in horses with small intestinal inflammation, horses with DPJ had significantly higher hepatic enzyme activities than did the control group of horses with small intestinal strangulating obstruction (SISO).17 More than 50% of horses with DPJ had biochemical evidence of hepatic disease (high GGT, aspartate aminotransferase, or ALP activity). In addition, horses with DPJ had a 12.1-fold higher risk of having high GGT activity and a 1.8-fold higher risk of having high aspartate aminotransferase activity than did horses with SISO. Aspartate aminotransferase activity in horses with proximal enteritis ranged from 133 to 2994 IU/L (reference range, 215.8 to 365 IU/L), GGT levels ranged from 7 to 117 IU/L (reference range, 6.2 to 19.1 IU/L), and ALP levels ranged from 86 to 1103 IU/L (reference range, 69.4 to 293.7 IU/L). Bile acid concentrations were rarely abnormal, which indicates that hepatic failure was uncommon. Histopathologic evidence of liver disease was a common biopsy and necropsy feature in the horses with proximal enteritis. Centrilobular necrosis and inflammation were noted in some cases.
TREATMENT. Because the causative agent or agents of DPJ are unknown, treatment remains empirical and consists of aggressive supportive therapy. The continuous production of enterogastric reflux necessitates gastric decompression every 1 to 2 hours to relieve pain and to prevent gastric rupture. The stomach should be decompressed frequently, regardless of whether the horse is showing signs of abdominal pain, as these signs may be masked by severe depression or the administration of analgesic or antiinflammatory medications. Horses should receive nothing by mouth until small intestinal function has returned, recognized clinically by cessation or reduction of the nasogastric reflux to 1 to 2 L over a 4-hour period and increased frequency of borborygmi. The time necessary for gastric decompression varies with each patient. Repeated rectal examinations after the first day of therapy inconsistently reveal distended loops of small intestine, depending on the frequency of removal of the reflux and the severity of the initial lesion. Ultrasonography may reveal fluid-filled small intestine when the bowel is not discernible by rectal palpation. Loops of small intestine are most frequently visualized in the ventral flank area, near the udder or prepuce; therefore this area should be examined in all cases of suspected small intestine distention.
Intravenous administration of a balanced electrolyte solution is necessary to maintain intravascular fluid volume and cardiovascular performance. In some horses even rapid administration of fluid fails to adequately restore and maintain intravascular volume because of enteric fluid losses that can be as great as 8 L per hour. In addition, the very large volume of isotonic crystalloid fluid that must be given intravenously to keep pace with enteric fluid losses in horses with DPJ may accelerate the flux of fluid from the vasculature into the intestinal lumen because of reduced intravascular oncotic pressure, increased capillary perfusion pressure, and increased capillary permeability in the inflamed intestine. Consequently, the balance between adequate hydration and the volume of enterogastric reflux obtained requires careful and frequent monitoring.
Administration of colloid solutions may be of benefit in preserving intravascular volume without promoting enterogastric reflux. The colloids most frequently used in horses include hyperimmune plasma and hetastarches. Plasma products require a large volume of administration to exert a colloidal effect, which is cost prohibitive in many cases. Smaller doses, however, may have a beneficial effect in horses with DPJ, particularly in animals showing signs of sepsis or endotoxemia. Hetastarches have been shown to significantly increase plasma oncotic pressure in ponies administered 10 mL/kg31 and represent a reasonably priced alternative to plasma. These solutions have been associated with changes in the hemostatic profile in normal ponies at higher doses32 and should be used with caution only in horses already at risk for coagulopathies, particularly with the higher-molecular-weight formulations.
During the initial hours of therapy, even aggressive intravenous fluid administration may result in only moderate clinical improvement. A positive clinical response—as evidenced by improved hydration status, decreased heart rate, decreased enterogastric reflux, improved attitude, and improvement in parameters reflecting kidney function (decreased blood urea nitrogen [BUN] and serum creatinine levels)—is correlated with resolving intestinal inflammation.
NSAIDs should be used judiciously to prevent the masking of the clinical signs of a potential surgical lesion. Flunixin meglumine can be used at a dose of 0.25 to 0.5 mg/kg PO every 6 hours to reduce the untoward effects of arachidonic acid metabolites.
Antimicrobial agents are typically administered to horses with DPJ, although the necessity for antimicrobial treatment in horses with DPJ is uncertain. Because of the association of DPJ with C. difficile, administration of intravenous penicillin G sodium or potassium (22,000 to 44,000 IU/kg IV q6h) is warranted. Metronidazole also has excellent activity against C. difficile; however, administration is difficult because nothing can be administered orally. Rectal administration of metronidazole has been studied33 and can be used in these cases. The dose and frequency of administration should be increased because bioavailability after rectal administration is much less than after oral administration (30% vs. 74%, respectively). Broad-spectrum antimicrobial treatment may be indicated in horses with low WBC counts, but care must be taken in selecting an antimicrobial to avoid potential adverse effects, particularly nephrotoxicosis with aminoglycosides in a dehydrated patient with compromised renal function.
Horses with DPJ may have to be kept from eating for several days and are often in a hypermetabolic state; therefore they rapidly develop a negative energy and nitrogen balance. In these horses, parenteral nutritional support should be considered. Parenterally administered solutions containing glucose, balanced amino acid solutions, lipid emulsions, balanced electrolyte and trace minerals, and vitamins have been administered to adult horses with a variety of intestinal disorders, including DPJ. Part of a horse's nutritional requirements (8000 to 12,000 kcal/day) can be provided with glucose-amino acid solutions that are of moderate cost. The rationale for this treatment is that through provision of nutritional support to an anorexic, severely ill horse, the healing process is facilitated, complications are minimized, and the duration of hospitalization may be shortened. Thus the overall cost of providing nutritional supplementation, enteral or parenteral, to horses with DPJ may well be offset by quicker recoveries and diminished requirements for other costly treatments.
Prokinetic agents may also be useful in cases of DPJ. Of the available prokinetics, lidocaine is used most frequently.34 A slow intravenous loading dose of 1.3 mg/kg in a bolus, followed by a continuous infusion of 0.05 mg/kg/min, has been shown to shorten the time of reflux and shorten the hospital stay of horses with DPJ.35 It may do this by decreasing sympathetic tone, acting as an analgesic agent, affecting ion channels, or decreasing granulocyte infiltration in the intestinal wall. Its use should be reserved for horses in which a surgical lesion has been ruled out because it can effectively mask intestinal or foot pain. Horses should be refluxed frequently during the infusion and checked for other signs of complications, such as laminitis, routinely. Metoclopramide, erythromycin lactobionate, and cisapride are also used in cases of DPJ.34 The efficacy of prokinetics in this disease is debated, mainly because the intestine must be healthy in order for the drugs to exert an effect. A more in-depth discussion of prokinetic agents can be found in the Gastrointestinal Ileus section.
Medical therapy is sufficient in most cases of DPJ; however, surgical exploration is sometimes necessary for definitive diagnosis; if horses show uncontrolled pain, have prolonged nasogastric reflux (>7 days), or have excessive fluid losses that cannot be corrected with conventional fluid therapy; or if clinical and laboratory findings are strongly suggestive of an intestinal obstruction. Retrospective comparisons of medical and surgical therapy of DPJ showed that in surgical cases, survival rates were significantly decreased and the nasogastric reflux lasted longer and continued in larger total volume. The horses in surgical cases were also more likely to develop complications such as diarrhea and showed a higher rate of incisional infection than did horses that underwent surgery for other types of colic.36
COMPLICATIONS. Complications of DPJ include septic peritonitis, cholangiohepatitis, myocardial and renal infarction, aspiration pneumonia, adhesions of the proximal small intestine, and laminitis. In severe cases of DPJ, a segment of the small intestine may become infarcted, which necessitates surgical removal. The prognosis for surviving the initial intestinal insult is good in cases of DPJ. Death and function losses from this disease are more commonly related to the secondary complications such as laminitis and intraabdominal adhesions. In one report, laminitis occurred in 28% of horses with DPJ, and associated factors were high body weight and hemorrhagic gastric reflux.37 Laminitis prophylaxis is routinely incorporated into the medical therapy and can include cryotherapy, NSAIDs, topical glyceryl trinitrate, and DMSO (200 mg/kg given as a 10% solution in normal saline). In one study, horses that received heparin as a prophylactic treatment for laminitis were less likely to develop clinical laminitis than were horses that 37
did not receive heparin.3
■