Equine Proliferative Enteropathy
Nicola Pusterla
Equine proliferative enteropathy (EPE) is a disease of foals caused by the obligate intracellular organism L. intracellularis. It affects mainly weanling foals and occasionally young adult horses and is characterized by fever, lethargy, peripheral edema, diarrhea, colic, and weight loss.
The diagnosis of EPE may be challenging and relies on the presence of hypoproteinemia resulting from hypoalbuminemia, thickening of segments of the small intestinal wall observed on abdominal ultrasonography, positive serologic findings, and molecular detection of L. intracellularis in feces. The disease occurs almost worldwide and has been reported in the United States, Canada, Europe, South Africa, Australia, Brazil, and Japan.38-42EPIDEMIOLOGY. In pig populations, the chronic form of the disease is maintained by subclinically affected pigs or is established environmentally in some sites, allowing transmission of L. intracellularis to serial flows of pigs.43 Mice and rats have been shown to be important reservoirs of L. intracellularis on pig farms; prevalences of animals with positive PCR assay results vary substantially between farms (4% to 83%).44,45 Rodents appear to be suitable reservoir hosts because of their susceptibility to L. intracellularis, their close contact with domestic animals, and their high reproductive rate, and they maintain L. intracellularis across generations. The source of infection has not been determined for horses. Exposure to pig feces has been speculated as a potential source of infection for horses since cases of EPE were first reported. However, in most cases of EPE, no history or evidence of direct or indirect exposure to pigs or pig feces has been reported. Moreover, multilocus variable-number tandem repeat profiles of pig and equine isolates differ greatly. One experimental study demonstrated host specificity for L.
intracellularis isolates cultured from pig or horse intestines.46 The study showed that clinical signs, longer periods of shedding, and stronger serologic immune responses were observed in animals infected with species-specific isolates. Previous studies showed that a variety of wild and domestic animals (including dogs, cats, rabbits, opossums, skunks, mice, and coyotes) can shed L. intracellularis on farms with diagnosed EPE cases.47,48Fecal-oral transmission of L. intracellularis has been documented in naive foals housed with foals clinically infected with an equine isolate of L. intracellularis.4 One study showed that feces from rabbits experimentally infected with an equine isolate of L. intracellularis served as infectious material for weanling foals.50 Although infected rabbits and foals remained asymptomatic, infection was supported by fecal shedding of L. intracellularis and detection of specific antibodies to L. intracel- lularis. Although the natural infectious dose for foals has not been determined, pigs receiving as low as 105 L. intracellularis organisms have been shown to develop infection.51
In piglets, large group size, weaning, transportation, diet change, and mixing have been associated with clinical disease. Predisposing situations such as the stress of weaning, overcrowding, decline in L. intracellularis-specific colostral antibodies, endoparasitism, and introduction of new animals have been suggested as factors in the development of EPE in foals.38 In pigs, infection and fecal shedding of L. intracellularis may persist for as long as 12 weeks.51 This is in sharp contrast to experimentally infected foals, which show onset and duration of fecal shedding ranging from 10 to 14 days and 17 to 27 days, respectively.49 Previous work has shown that L. intracellularis is likely to survive in environmental conditions for 1 to 2 weeks at 5° C to 15°C.52
PATHOPHYSIOLOGY.
The mechanism of enteritis after infection with L. intracellularis involves invasion of the proliferating crypt cells in the ileum, causing excessive mitotic division and severe hyperplasia.53,54 The hyperplastic mucosa becomes grossly thickened and develops a corrugated appearance. As would be expected, this thickening of the mucosa, along with the proliferation of immature crypt cells rather than mature villous cells, leads to a limited brush border development and a decreased absorptive capacity, which results in the weight loss and hypoproteinemia characteristic of these cases. The organism can divide within the infected cells and migrate up to the mucosal layers as the cells proliferate and advance. The differential diagnosis in these cases mainly includes R. equi enteritis, which can also cause ulceration in the areas of Peyer patches throughout the small intestine, cecum, and colon.CLINICAL AND LABORATORY FINDINGS. EPE manifests in characteristic signalment, seasonality, clinical signs, and blood work abnormalities. The disease is generally manifested in foals younger than 1 year of age and, in North America, often between August and February.39 Although the disease is common in weanling foals 4 to 7 months of age, cases of EPE have been seen in young adult horses.42 Lethargy, anorexia, fever (>38.5°C), peripheral edema (ventrum, sheath, throatlatch, and distal limbs), weight loss, colic, and diarrhea are among the most common clinical findings in affected foals. Early clinical signs are generally unspecific and include mild depression, partial anorexia, and fever. Although diarrhea is common in affected foals and the character can vary from cow pie to watery, some affected foals produce normal feces. Fatal necrotizing enteritis associated with L. intracellularis has been reported in foals that developed acute onset of clinical signs, followed by rapid clinical deterioration and death caused by endotoxemia, bacteremia, or disseminated intravascular coagulation.55
Foals with EPE may also have concurrent disorders such as respiratory tract infections, gastric ulcerations, and intestinal parasitism.
Signs of EPE may resemble those of more common gastrointestinal disorders such as parasitism, bacterial infections (Clostridium spp., Salmonella spp., R. equi, N. risticii), rotavirus, coronavirus, ulcerations, sand accumulation, intestinal obstruction, and intoxication with plants, chemicals, and pharmacologic agents such as NSAIDs or antimicrobials. As in pigs, the disease can be subclinical in foals and be manifested by a self-limiting and transient decrease in total serum protein concentration, coupled with decreased daily weight gain, in comparison with unaffected foals.49 It remains to be determined whether growth retardation or unthriftiness are associated with subclinical infection.The most consistent laboratory finding of clinical EPE is hypoproteinemia resulting from hypoalbuminemia. Total protein concentration is generally less than 5.0 g/dL, and albumin concentration is usually less than 2.0 g/dL. In one case report, hypoalbuminemia was the only consistent clinicopathologic abnormality of 57 affected foals; albumin concentrations ranged from 0.9 to 3.3 g/dL (normal reference range, 2.7 to 4.2 g/ dL).39 The exact mechanisms by which hypoalbuminemia develops in affected foals have not been investigated. It appears that decreased feed intake, coupled with malabsorption and protein-losing enteropathy resulting from the proliferative nature of the disease, may explain why albumin levels are low.56 Affected foals may also demonstrate nonspecific blood abnormalities such as anemia or hemoconcentration, leukocytosis or neutropenia, hyperfibrinogenemia, increased activity of muscle enzymes, and electrolyte abnormalities (hypocalcemia, hypochloremia, and hyponatremia). Urine analysis to rule out protein-losing nephropathy and cytologic evaluation of abdominal fluid to rule out protein lost to a third space yields generally unremarkable results.
DIAGNOSTIC WORKUP. A presumptive diagnosis of EPE is generally based on age of the affected animal, clinical signs, hypoproteinemia/hypoalbuminemia, presence of thickened loops of small intestine on ultrasonographic evaluation, and absence of other causes of enteropathy and protein losses.
Abdominal ultrasonography, although not very sensitive, may show segments of thickened small intestine and excessive abdominal fluid. In these cases, abdominocentesis yields a noninflammatory transudate. An antemortem diagnosis is generally confirmed through PCR detection of L. intracellularis in feces or rectal swab or serologic findings.It is essential to perform both molecular and serologic diagnostic testing because these modalities have high analytical specificity but variable sensitivity, depending on the situation. Negative PCR results can be expected if the fecal samples are collected from foals that have received prior antimicrobial treatment or those in an advanced disease stage, when L. intracellularis organisms are no longer expected in the feces. Negative serologic results can be expected in the early stage of the disease, when humoral immune responses are not yet strong enough to be detectable by serology. Moreover, differences in sensitivity among different PCR and serologic assays can lead to divergent results. Among PCR assays, the use of a real-time platform has been shown to yield the best sensitivity and to reduce the likelihood of crossover or carryover contamination (i.e., false-positive results).57-59 Several serologic assays, including indirect fluorescent antibody test, ELISA, and immunoperoxidase monolayer assay, have been validated and established for pigs.60-62 A comparative study with equine serum samples has shown that various serologic assays yield accurate results; however, the immunoperoxidase monolayer assay is the most specific in determining the presence of anti-L. intracellularis antibodies in adult horses with EPE.63
PATHOLOGIC FINDINGS. Lesions are most frequently found in the distal jejunum and ileum, although diffuse thickening of the small intestine may occur.53 A classical finding is pronounced mucosal thickening with varying severity of ulceration and transmural edema. The affected bowel appears to be stiff, and the mucosal surface has a corrugated appearance.
Mucosal pleocytosis is a common feature, but in different cases the predominating inflammatory cell type differs. A lymphocytic or plasmacytic cellular infiltration may be present. Crypt proliferation is accompanied by crypt elongation and epithelial hyperplasia. The villi are blunted and may become fused. Silver staining with Warthin-Starry stain reveals elongated, curved bacilli in the apical zone of the crypt epithelial cells.TREATMENT. It is important to treat affected animals early, before lesions become advanced and result in marked weight loss and critically low serum protein values. Treatment of EPE in horses involves the use of antimicrobials such as macrolides, alone or in combination with rifampin, chloramphenicol, oxytetracycline, doxycycline, or minocycline, administered for 2 to 3 weeks. The choice of antimicrobial in the treatment of EPE should account for the risk of inducing disturbance of the gastrointestinal flora and renal toxicity. This is especially a concern in treating older foals with severe hypoalbuminemia. Supportive therapy with crystalloid fluids is necessary to correct dehydration, electrolyte imbalances, and azotemia secondary to fluid losses from profuse diarrhea. Colloidal support with plasma or hetastarch can help correct the edema and decreased colloid oncotic pressure. NSAIDs should be used with caution in foals showing signs of dehydration.
The prognosis in these cases is generally good with early and correct diagnosis of the problem. Therapy can be prolonged and should be continued until the diarrhea and hypoproteinemia have resolved and there is no longer evidence of thickened small intestine on ultrasonography.
Concurrent medical conditions should also be addressed. Clinical improvement after treatment is rapid; however, it may take weeks for the hypoproteinemia to resolve. Spontaneous recovery of clinically infected foals has not been documented, and up to 93% of treated foals survive the disease.39 In general, nonsurvivors develop complications associated with gastrointestinal translocation, gastrointestinal perforation, or kidney failure.55 Frazer reported that clinically affected and successfully treated foals sold for an average of 68% of the average price of unaffected foals by the same stallion.39 However, their monetary earnings from racing were not significantly different from those of other horses.64
MONITORING AND PREVENTION. Early recognition of clinical cases and separating affected animals from the rest of the susceptible foals until full recovery or cessation of fecal shedding appears to be a logical biosecurity measure to prevent spread and environmental contamination. The monitoring of a herd with endemic EPE status includes the regular physical evaluation of resident foals and the monthly or bimonthly assessment of total protein concentration and monthly serologic status. Monitoring for exposure to L. intracellularis and hypoproteinemia/ hypoalbuminemia should begin at least 4 weeks before the historical first detection of clinical cases.
Because of the lack of epidemiologic data regarding potential natural reservoir hosts, as well as the lack of information pertaining to the biological processes of L. intracellularis, management changes should not be made on endemic farms. Moreover, maintaining good pest control and preventing nonequine domestic and wild animals from obtaining access to feed and feeding areas may potentially minimize the risk of disease spread.
Prevention strategies have been best described in pigs with in-feed antimicrobials and a commercially available L. intracel- lularis vaccine.65-67 Detectable humoral and cellular responses can be measured in foals administered an avirulent live L. intracellularis vaccine.68,69 The L. intracellularis vaccine has been shown to be safe and its administration well tolerated by the foals. A field efficacy trial performed on EPE-endemic farms in central Kentucky in 2008 showed that vaccinated foals maintained higher daily weight gains and higher total protein concentrations than did a nonvaccinated, naturally seroconverted group.70 Under experimental conditions, weanling foals vaccinated intrarectally with an avirulent live vaccine against L. intracellularis were protected against clinical and subclinical EPE after challenge exposure with a virulent L. intracellularis isolate of equine origin.71 This was determined by lack of clinical disease, absence of hypoproteinemia and ultrasonographic abnormalities compatible with EPE, and a significant reduction in L. intracellularis fecal shedding in vaccinated foals in comparison with nonvaccinated foals. Moreover, average daily weight gains from the vaccinated foals over the entire study period were similar to those of the control foals and significantly higher than those of the nonvaccinated foals, which highlights the benefit of the vaccine in the prevention of subclinical disease. The extralabel use of the L. intracellularis vaccine should be considered on EPE-naive and endemic farms in an attempt to reduce or prevent EPE. Timing of vaccine administration should again be synchronized with historical disease occurrence. Moreover, routine monitoring for clinical signs and hypoproteinemia/hypoalbuminemia is still recommended even when vaccine prophylaxis is used.
■ Rhodococcus equi Enteritis R. equi most frequently causes a severe pyogranulomatous pneumonia in foals 2 to 3 months of age. Extrapulmonary disorders have been associated with R. equi infection in foals, and the presence of these disorders is associated with an increase in mortality. Extrapulmonary disorders of the gastrointestinal system may occur in as much as 50% of cases. Diarrhea is reported to occur in up to 33% of R. equi cases. In one study of 150 affected foals, enterocolitis and typhlitis were reported in 31, intraabdominal abscesses in 25, abdominal lymphadenitis in 25, and septic peritonitis 11.72
PATHOPHYSIOLOGY. Intestinal infection with R. equi can occur through either fecal-oral transmission or swallowing of infected sputum. The organism invades and reproduces within the macrophages, causing a pyogranulomatous disease. In a survey of normal foals on two different farms, R. equi was shed in the feces of 16 of 17 and 19 of 26 foals, respectively.73 Only 2 foals developed clinical signs of intestinal disease, and the shedding of bacteria in the feces increased threefold to fourfold during those times. Such foals, as well as adults, are probably the source of repeated contamination on endemic farms. The organism’s ability to cause disease is based on the presence of virulence factors, particularly virulence-associated protein A (VapA), which has been most commonly associated with disease in pneumonic foals.
CLINICAL AND LABORATORY FINDINGS. Foals diagnosed with R. equi enteritis typically manifest the signs of pneumonia first, although foals in which the enteric form is the major pathologic process have been reported.74 With the enteric form of the disease, diarrhea, weight loss, and colic are present. Many affected foals are febrile, anorexic, and depressed. Typical clinicopathologic findings include leukocytosis with neutrophilia and severe hyperfibrinogenemia. Ultrasonography of the abdomen may reveal pyogranulomatous abscesses in the lymph nodes.
A diagnosis of R. equi enteritis can be presumed in pneumonic foals showing signs of gastrointestinal disease for which cultures of transtracheal wash fluid yield positive results for R. equi. R. equi can also be cultured from the feces, small intestinal luminal contents, or, occasionally, the peritoneal fluid of affected animals. A PCR based on the vapA gene has been developed and can be used as an adjunct diagnostic tool in these cases.75
PATHOLOGIC FINDINGS. The most common small intestinal lesion is multifocal ulcerative enteritis in the area of the Peyer patches of the ileum. Other parts of the small intestine may be affected, with lesions present throughout the entire small intestine.75 These lesions frequently extend into the cecum and colon as well. A suppurative exudate is also present, along with pyogranulomatous inflammation of the mesenteric lymph nodes. Co-infection with L. intracellularis has also been reported to occur.76
TREATMENT. Treatment of R. equi enteritis is similar to treatment of R. equi pneumonia. Erythromycin estolate (25 mg/ kg PO q6-8h) or erythromycin phosphate (37.5 mg/kg PO q12h) combined with rifampin (5 to 7.5 mg/kg PO q12h) has been the traditional treatment for these foals, and it is still effective but requires a longer duration of treatment and is difficult for owners to administer because of the frequency of the treatments. Alternative treatments include azithromycin (10 mg/kg PO q24h for 5 days, followed by q48h) and clarithromycin (7.5 mg/kg PO q12h), with or without rifampin. To prevent relapses, it is very important to continue treatment until the hematologic abnormalities and radiographic or ultrasonographic examinations have returned to normal.
COMPLICATIONS. Complications associated with R. equi enteritis include septic peritonitis and the development of intestinal adhesions. These may lead to death of affected animals or chronic abdominal problems in those that survive. Therapy is often prolonged in these cases, and owners should be warned that foals with extrapulmonary disorders associated with R. equi pneumonia have a more guarded prognosis.72
■ Enteric Pythiosis Pythium spp. are protistal organisms that belong to a group of phycomycotic organisms that also includes Conidiobolus and Basidiobolus spp. They are a frequent cause of severely pruritic cutaneous granulomas in horses along the Gulf Coast and southern United States. Much less frequently, the disease can cause granulomatous lesions in the small intestine.
PATHOPHYSIOLOGY. Pythium spp. are presumed to be transmitted via contact with contaminated water. Once ingested, the organisms are thought to penetrate the intestinal mucosa through an existing lesion because necrotic tissue is considered chemotactic.77 Pythium spp. may be able to penetrate healthy tissue, however, because some cases in dogs have been reported to have mesenteric lymph node involvement without any mucosal lesions.78
CLINICAL AND LABORATORY FINDINGS. Four reports of equine enteric pythiosis can be found in the literature.79-82 In all cases, masses occurred in the middle to distal sections of the jejunum. One horse died suddenly, one was euthanized during surgery, and two were successfully treated with a jejunal resection. Organic iodide therapy was instituted in one horse postoperatively for 30 days. In three cases, clinical signs of intestinal disease had been present for several months before diagnosis. Chronic colic, weight loss, inappetence, and ill thrift have all been reported and could be related to the intestinal lesion. None of the reported animals had skin lesions. Hematologic evaluation was nondiagnostic in the three cases in which it was performed.
On gross examination, lesions appear caseous with discrete yellow foci (“kunkers”), and the intestinal wall is thickened because of a pyogranulomatous inflammation. On microscopic examination, a diffuse, mixed inflammatory infiltrate, along with granulation tissue, is found in the submucosa, tunica muscularis, and mesenteric attachments. Culture of the organism from these lesions is difficult; however, an indirect immunoperoxidase technique to stain for Pythium-positive hyphae is available in some laboratories.81 Serologic testing for Pythium in canine and equine cases is available; however, it has been validated only for cutaneous disease in horses.
TREATMENT. Treatment of phycomycetes is often difficult. They are not true fungi; therefore they are resistant to many antifungal drugs. Systemic amphotericin B is only rarely effective in treating the cutaneous disorder. Organic iodides are inexpensive and safe when administered orally, but the mechanism of action as antimicrobial drugs is not understood, and the efficacy of this compound to treat this disease has not been proven. A vaccine can be formulated against the organism, and this has been shown to shrink the lesions in horses with cutaneous disease. Its efficacy against enteric disease is unknown at this time. In addition, premortem or presurgical diagnosis of the disease is extremely difficult, and so surgical resection with biopsy are the most effective treatment.
■ Inflammatory Bowel Disease Several intestinal disorders characterized by inflammatory cell infiltration have been placed under the umbrella of IBD, including granulomatous enteritis, multisystemic eosinophilic epitheliotropic enterocolitis, eosinophilic enterocolitis, lymphocytic-plasmacytic enteritis, and basophilic enterocolitis.83-89 IBD in humans is typically characterized by a neutrophilic inflammation, but neutrophils are only the effector cell in a highly complex disease process.90 The syndromes described for equine inflammatory intestinal disorders therefore appear to differ from those of human IBD; because of the different types of cellular infiltrates found in affected horses, these disorders presumably reflect different pathophysiologic mechanisms. Thus use of the term inflammatory bowel disease is not intended to imply either a similarity to the condition described in human beings or similarity among the various syndromes described in horses.
CLINICAL AND LABORATORY FINDINGS. Horses with IBD typically have progressive weight loss despite a good appetite and have intermittent abdominal discomfort. If the disease predominates in the small intestine, diarrhea may not be a feature. In some cases, associated dermatitis is present.91 Affected horses often present with peripheral edema secondary to hypoproteinemia from enteric protein losses. Ultrasonographic examination may reveal thickened walls of the small intestine (>5 mm in diameter).
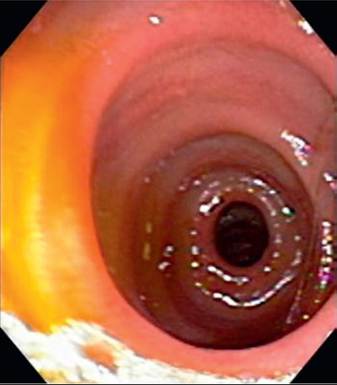
FIG. 32.63 Endoscopic view of the duodenum in a horse with lymphocytic-plasmacytic enteritis. Note the heterogeneous appearance of the duodenal mucosa.
Clinicopathologic abnormalities may include anemia, hypo- albuminemia, hypoproteinemia, and malabsorption of glucose and D-xylose. The results of a glucose tolerance test were abnormal in 70% of cases in one report.92 Hypoalbuminemia in the absence of proteinuria or severe liver dysfunction is consistent with protein-losing enteropathy. Some horses may have a relative gammopathy. Serum electrolyte concentrations and total CO2 levels are usually normal. Subclinical disseminated intravascular coagulation with thrombocytopenia and increased fibrinogen degradation products have been identified in horses with chronic enteritis.86,93 Serum antibodies to gluten have been detected in horses with IBD, as well as in those on a gluten-rich diet.94 This suggests a potential pathogenic role of gluten in at least some cases of equine IBD, and dietary changes may play an important role in treatment.
In most affected horses, cellular infiltration can be found to varying degrees throughout the intestinal tract. Therefore rectal mucosal biopsy may be useful for identifying cases of IBD in horses.95 If the proximal duodenum is involved, endoscopic biopsies can be used for diagnosis (Fig. 32.63). A definitive diagnosis often requires biopsy of the small intestine, large intestine, or both. With appropriate instruments, this can be done through laparoscopy, although an exploration via a ventral midline approach enables a more thorough evaluation of the abdomen.
Histopathologic evaluation of biopsy specimens can be used to differentiate among the various IBDs reported in horses, according to the respective criteria.87 A diagnosis of granulomatous enteritis is made when aggregates of macrophages and epithelioid cells are found in the mucosa, submucosa, or both, along with villous atrophy. In lymphocytic-plasmacytic enterocolitis, lymphocytes and plasmacytes are present in the lamina propria, and villous atrophy usually occurs. For multisystemic eosinophilic epitheliotropic disease, eosinophils, lymphocytes, and macrophages are found in the mucosa and submucosa. In rare cases, basophils have also been reported.
IBD syndrome, termed idiopathic focal eosinophilic enteritis (IFEE), involves focal areas of eosinophilic inflammatory infiltrates within the small intestine.89,96-100 Affected horses typically are examined not because of chronic weight loss or diarrhea, but rather because of acute colic. Hypoproteinemia and malabsorption are not characteristic. The lesions are intramural masses or circumferential mural bands. Eosinophils with or without lymphocytes are seen infiltrating all layers of the intestine, with varying degrees of fibrosis.100 Further characterization of the inflammatory lesions indicate that IFEE probably represents a focally exacerbated inflammatory reaction in horses with diffuse eosinophilic enteritis.99 No underlying cause of the disease has been found, although food allergy, parasitism, and Pythium spp. have all been suggested.100 The incidence, or at least the diagnosis, of this disease appears to be increasing.
TREATMENT AND PROGNOSIS. Because the specific diseases included in the general category of IBD are quite different, a generalized treatment recommendation cannot be made, although corticosteroids are considered the mainstay of medical management. In one study, a lack of response to initial steroid therapy (prednisolone) was associated with a poorer prognosis for long-term survival, as was a lower peak xylose concentration.101 The horses in this study were also treated with coadministration of anthelmintic drugs (fenbendazole) and reported a 3-year survival rate of 65%. The high survival rate may also be a result of case selection and case definition. Reported cases of eosinophilic, lymphocytic, and basophilic enteritis have classically failed to respond to treatment. If treatment is attempted, immunosuppressive doses of dexamethasone, up to 0.2 mg/kg IM or IV once daily, are recommended. Successful remission of granulomatous enteritis was reported in one patient that was treated with dexamethasone.102 Cases of IFEE should be differentiated from other types of IBD with regard to treatment and prognosis. These cases frequently respond to surgical decompression without resection if circumferential mural bands are the only lesion present.100 In cases of intramural masses, surgical resection of the lesions usually resolves the problem.98 Other treatments attempted include anthelmintic drugs with larvicidal activity, hydroxyurea, metronidazole, clioquinol (iodochlorhydroxyquin), and sulfasalazine.103
■ Neoplasia Primary and secondary neoplasia involving the alimentary tract of horses is relatively uncommon, but several cases have been reported.104 Typical signs associated with, but not diagnostic for, small intestinal neoplasia include colic and weight loss. In most horses with focal intestinal neoplasia, the problem becomes apparent only when lumen obstruction develops. Lymphosarcoma can be disseminated throughout a large portion of intestine, eventually resulting in a malabsorption and weight loss syndrome. Alimentary lymphoma is the most common intestinal neoplasia, and the small intestine is the most commonly affected intestinal segment.105 Lymphosarcoma affects horses of all ages, although many of those with the alimentary form are older. The diagnosis of enteric lymphosarcoma is occasionally based on cytologic examination of fluid obtained by abdominocentesis, although multiple samples may be required before a positive sample is obtained.106 In other cases, intestinal biopsy is necessary to diagnose the neoplastic disorder. Ultrasonography may reveal thickening and decreased echogenicity of the small or large intestinal wall or of both.107 The prognosis is best if the tumor is discrete and can be removed surgically. A combination chemotherapy protocol of cytarabine (170 mg/ m2 IM), cyclophosphamide (142 mg/m2 IV), and prednisolone (86 mg/m2 PO q48h) has been reported to be effective in the treatment of mixed-cell thoracic lymphoma.108 In other cases, corticosteroid therapy may induce clinical remission for several months, although it is not curative.
Other neoplasms affecting the small intestine are unusual; they typically arise from the wall of the bowel and include 109 110 111
adenocarcinoma,109 leiomyosarcoma,110 and neurofibroma.111 These tumors often result in intestinal obstruction and signs of abdominal discomfort. Discrete tumors may be surgically removed.
Paraneoplastic syndromes may be the first sign of neoplastic processes in a horse. Pemphigus, hypoglycemia, hypercalcemia, erythrocytosis, and neuropathies have all been associated with tumors in horses.112 Paraneoplastic processes may also lead to intestinal tract dysfunction in horses with extraintestinal tumors. Amyloid deposition secondary to multiple myeloma in a horse has been described.113
■ Small Intestinal Fibrosis Small intestinal fibrosis is a rare syndrome that causes weight loss, chronic colic, and progressive debility in horses and ponies. Clusters of affected animals have been reported in Colorado114,115 and Missouri.116 The pathophysiologic origin of the fibrosis is not known, although ingestion of toxins (Convolvulus arvensis or common bindweed), inhibitors of 11β-hydroxysteroid dehydrogenase, and compounds with mineralocorticoid activity has been suggested.
Rectal palpation typically reveals thickening of the small intestinal wall, which may be confirmed by ultrasonography.115 Gross examination may reveal that the overall length of the intestine is shortened by as much as 50%.114,115 The histologic lesions include arteriosclerosis, capillary endothelial hypertrophy, extensive fibrosis of the submucosa, and hypertrophy of the muscularis mucosae and tunica muscularis.114 The prognosis with the disease is determined by the length of the intestine that is involved. Surgical resection may be attempted.
■ Lymphangiectasia and Chyloabdomen There are few reports of lymphangiectasia and chyloabdomen in the literature. Lymphangiectasia is dilation of the lymphatic channels of the small or large intestine (Fig. 32.64), usually caused by an abscess117 or neoplasia. There are reports of chyloabdomen resulting from congenital lymphatic defects in a neonatal foal, intraabdominal abscesses in a foal, and abdominal adhesions in a miniature horse.117-119 Typically, thickening of the intestinal wall and leakage of chyle into the peritoneal cavity result from obstruction or rupture of the lymphatic channels. Signs include abdominal discomfort, diarrhea, and chronic weight loss. Diagnosis is made on the basis of abdominal fluid analysis and ultrasonography. Chylous abdominal fluid appears milky and may contain a high percentage of lymphocytes. Ultrasonograms may reveal segments of thickened small intestine. Diagnosis is confirmed at surgery or postmortem examination, and treatment, if possible, is usually surgical, although in the author's experience, medical resolution of the effusion has been achieved.
More on the topic Equine Proliferative Enteropathy:
- Equine Proliferative Enteropathy
- REFERENCES
- Molecular Testing for Infectious Diseases in Horses
- REFERENCES
- Hypoproteinemia
- Smith Bradford P., Van Metre David C., Pusterla Nicola (eds.). Large Animal Internal Medicine. Part 1. 6th edition. — Elsevier,2020. — 2279 p., 2020
- Mechanisms of Decreased Growth and Decreased Weight Gain
- Diarrhea
- INDEX