Ectopic Ureter
Thomas J. Divers • Stephanie A. Brault • Alexandra J. Burton
Although rare, ectopic ureter is the most frequently reported developmental anomaly of the equine urinary tract and there are many case reports and series.1-13 This abnormality is the result of an error in embryologic development causing one or both ureters to empty into the urethra, uterus, or vagina instead of attaching normally to the dorsal wall of the urinary bladder.1 Of the cases reported, almost all have been fillies, and the primary complaints were urinary incontinence and perineal dermatitis (urine scalding).1-13 However, this gender distribution may reflect easier recognition of partial urinary incontinence in females rather than a true gender predilection.
In the male, intermittent urine dripping from the end of the penis is less easily recognized; further, urine entering the pelvic urethra may pass retrograde into the bladder.Diagnosis
Ectopic ureter should be suspected in young horses with incontinence observed shortly after birth. Renal function is usually normal, but the affected ureter may be extremely dilated. In young foals (e.g., tract neoplasia in both studies were older than 20 years of age.1,2 This assumption is further supported by another recent study comparing idiopathic hemorrhagic cystitis with bladder neoplasia: The median age of horses with bladder tumors was 24 years (range 16 to 30 years of age).3
Primary kidney neoplasms include renal cell carcinoma (Fig. 34.6, A), adenoma, and nephroblastoma, with carcinoma and then adenoma being the most common.1,4-14 Renal cell carcinoma (or adenocarcinoma) and adenoma occur more frequently in older horses, older than 10 years of age and most often older than 20 years old. Nephroblastomas may be detected in young horses.15 Lymphosarcoma (Fig.
34.6, B), hemangiosarcoma, multiple myeloma, and melanoma may also involve the kidneys and, on rare occasions, the bladder.13 Squamous cell carcinoma is the most common bladder tumor, but horses may also develop transitional cell carcinoma, adenocarcinoma, and undifferentiated carcinomas of the bladder.3,4,19 Fibromatous bladder polyps may occur in younger horses and a poorly differentiated aggressive leiomyosarcoma of the urogenital tract with extensive bladder involvement has been described in a 2-year-old filly.4,19,20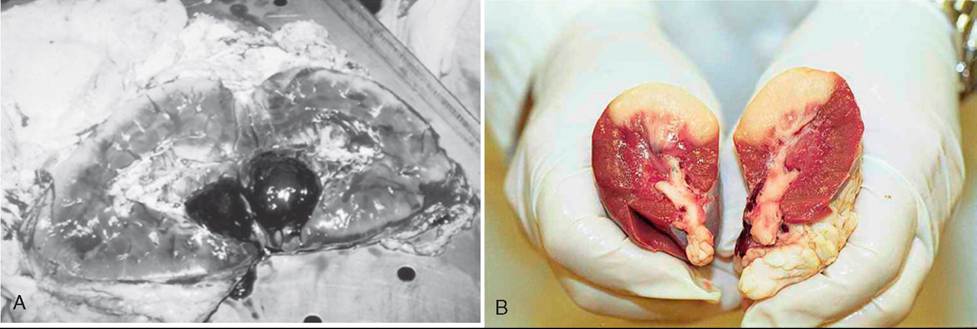
FIG. 34.6 A, Cut section of the left kidney from a 25-year-old horse with chronic weight loss, hematuria, and severe anemia. The kidney appeared normal except for a small 4 ? 5 cm carcinoma with surrounding hemorrhage. B, Cut section of an equine kidney with metastatic lymphoma infiltration (pale tissue). (A, Courtesy Thomas J. Divers. B, Courtesy Montague N. Saulez.)
Clinical Signs and Diagnosis
Clinical signs in horses with renal neoplasia include hematuria, weight loss, and recurrent colic. Sudden death may occur if the neoplasm hemorrhages into the abdomen or thorax. Renal tumors may result in marked enlargement of the kidneys such that both left and right kidneys may be found on rectal palpation. In other cases, tumors may be circumscribed lesions within a kidney that disrupt the renal architecture but cannot be felt during rectal palpation. Ultrasonography may be invaluable for detecting such tumors, however, if very small, renal tumors may still be difficult to detect. Affected horses are usually not azotemic, but anemia may be detected when gross hematuria is observed. Although neoplastic cells are unlikely to be found in urine, cytologic examination of urine sediment is still warranted. Renal biopsy has been found to be associated with a low rate of serious complications and provided a histopathologic diagnosis in agreement with necropsy in 72% of cases.21 Although horses with a diagnosis of renal neoplasia had a greater risk of complications than those with any other histopathologic diagnosis, only 4/151 horses in the study had neoplasia.21 Nephroblastoma usually remains limited to the kidney; renal cell carcinomas typically metastasize.
The liver and lungs are the most common sites of metastasis, but tumors can also spread to unusual sites, leading to variable adjunct clinical signs such as lameness or an ulcerated mass on the premaxilla.7"10,14 Multiple myeloma involving the kidney resulted in hypercalcemia and a high serum parathyroid hormone-related protein concentration.17 Hypoglycemia was the chief clinical sign in a 6-year-old horse with renal cell carcinoma producing insulin-like growth factors.12Bladder tumors most commonly present with hematuria, weight loss, pollakiuria, and stranguria. A mass can usually be palpated on rectal examination, but it should not be confused with a cystolith or accumulation of sabulous concretions in the ventral aspect of the bladder.3 There may be mild to moderate anemia and sometimes hypoproteinemia (hypoalbuminemia). Other than hematuria and associated proteinuria, urinalysis results are often unremarkable, but with bladder tumors, cytologic examination of urine sediment is more likely to reveal neoplastic cells than with renal tumors.18,19 A diagnosis of bladder neoplasia may be confirmed by cystoscopic examination (Fig. 34.7) and biopsy. A recently described new syndrome of idiopathic hemorrhagic cystitis in horses closely resembles bladder neoplasia in clinical pathologic presentation.3 Unfortunately, biopsy and histopathology were not helpful in discriminating between bladder neoplasia and idiopathic hemorrhagic cystitis in this study.3
Treatment
The treatment of choice for unilateral renal neoplasia is nephrectomy.7,13 Unfortunately, most cases of renal cell carcinoma have metastasized by the time the diagnosis is made, and surgical intervention is of little benefit to horses with disseminated disease. In addition, many horses with renal neoplasia will be aged. Thus, careful evaluation for metastatic disease, assessment of comorbidities (e.g., PPID, poor dentition), and consideration of age should be undertaken before contemplating a nephrectomy.
Survival following diagnosis of renal carcinoma ± nephrectomy has been reported to be very poor (median 11 days, range 0 to 365 days).7 However, of interest, there is one report of a renal tubular cell carcinoma (confirmed by renal biopsy) considered too large to be operable, in a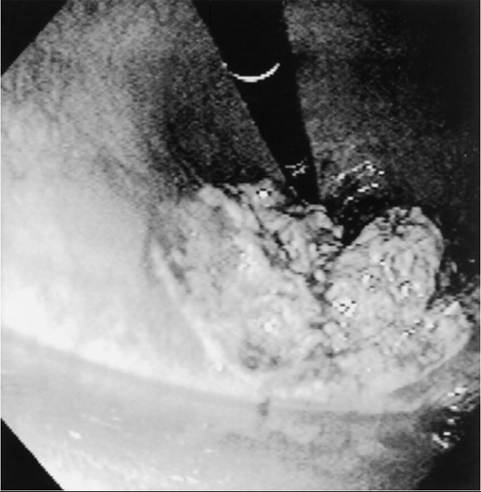
FIG. 34.7 Cystoscopic image of a squamous cell carcinoma of the bladder causing intermittent hematuria in a 14-year-old warmblood mare. The endoscope has been passed beyond the tumor and retroflexed to provide a view directed caudally; a pool of urine is in the foreground, and the tumor can be seen in the ventral aspect of the bladder neck.
15-year-old mare. No treatment was implemented, and the mare was reported to still be stable and in foal 1 year later.22 Treatment of confirmed bladder tumors includes surgical excision, and/or topical chemotherapy using either 5-fluorouracil or triethylenethiophosphoramide and systemic doxorubicin has also been used but prognosis is guarded to poor.19,20 Again, as affected horses are likely to be aged (often >20 years old), careful consideration of comorbidities and quality of life is important before under taking treatment.
EQUINE IDIOPATHIC HEMORRHAGIC CYSTITIS. Idiopathic hemorrhagic cystitis in horses is a newly described syndrome in horses presenting with stranguria and hematuria.3 In a case series of 11 horses from California with this condition, pyuria was present but not bacteria, and no bacterial growth on urine culture (aside from one horse, which was deemed a contaminant).3 Other than bacterial cystitis, which is often precipitated by urolithiasis and/or bladder dysfunction, sterile ulcerative cystitis in horses has been described in two horses in association with long-term phenylbutazone administration.23 Of note, idiopathic hemorrhagic cystitis was almost indistinguishable from bladder neoplasia in terms of clinicopathologic presentation, even by histopathology following mucosal bladder biopsy.3 However, horses with idiopathic hemorrhagic cystitis made rapid (within approximately 8 weeks), full recoveries, with antimicrobial ± nonsteroidal antiinflammatory treatment.
Horses with idiopathic hemorrhagic cystitis were significantly younger (median age = 16, range, 9 to 30 years) compared with those with neoplasia (median age = 24, range, 16 to 30 years), and much more likely to be male—10/11 horses were male, whereas all horses with neoplasia (n = 7) were mares.3 Finally, although gross cystoscopic findings were not different, horses with bladder neoplasia were more likely to have a mass visible on transrectal US.3 Thus, in a horse with clinicopathologic signs that could be attributable to either neoplasia or idiopathic cystitis, it may be worth treating conservatively as described earlier and waiting a few weeks to see if the signs and lesions resolve, rather than immediately employing chemotherapy or euthanizing the patient.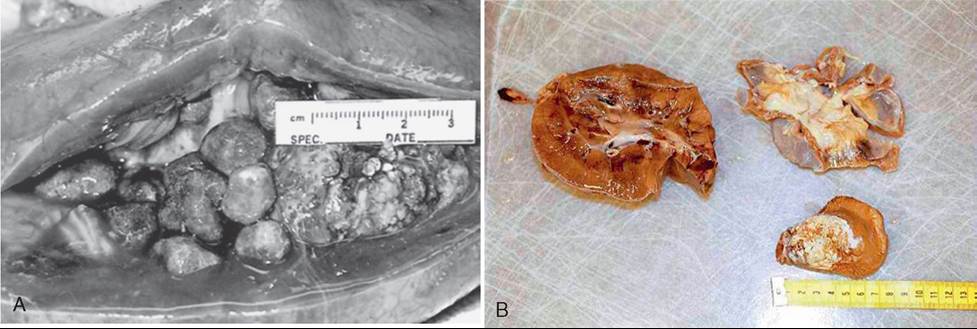
FIG. 34.8 A, Multiple nephroliths in the left kidney of a 12-year-old Thoroughbred that presented with a complaint of intermittent hematuria. The right kidney appeared normal on ultrasound examination, and renal function was normal. B, A single nephrolith in the kidney of a 10-year-old mare discovered incidentally at necropsy. (A, Courtesy Thomas J. Divers.)