Urolithiasis and Obstructive Disease
Montague N. Saulez
While the prevalence of obstructive disorders affecting the equine urinary tract is low, morbidity is high and the consequences thereof can be permanent and fatal.
Obstructions may occur throughout the urinary tract and clinical symptoms are dependent on the location and degree of obstruction. Partial obstructions may not initially be recognized and can lead to intermittent dysuria, stranguria, hematuria, incontinence, and variable signs of pain. Horses with complete obstruction exhibit severe abdominal pain (colic) leading to bladder or urethral rupture followed by depression and metabolic deterioration. Unfortunately, reoccurrence is frequent irrespective of treatment modality followed or the elimination of potential risk factors.Renal and Ureteral Calculi
Following renal tissue damage, calcium carbonate and calcium oxalate crystals can tightly adhere to the renal parenchyma, forming a nidus that allows repeated crystal precipitation and enlargement of the calculus.1 Underlying renal disease should always be suspected in horses with nephrolithiasis.2,3 It is thought that in horses, a risk factor for nephrolithiasis is prolonged use of nonsteroidal antiinflammatory drugs (NSAIDs), which can cause renal medullary necrosis (Fig. 34.1), thereby increasing the risk of nephrolith formation in the renal pelvis and terminal recess.
Clinical symptoms are dependent on the degree of luminal obstruction and include anorexia, dullness, and weight loss. This may progress to severe colic, hematuria, and stranguria. Bilateral nephrolithiasis may lead to chronic renal failure (CRF).2,3 Horses can also remain clinically asymptomatic with the presence of renal calculi incidentally discovered at necropsy4 (Fig. 34.8, A and Fig. 34.8, B). Diagnosis of renal or ureteral calculi is made by rectal examination revealing an enlarged kidney, ureter, or bladder.
Ureters are not normally palpable but can be detected if enlarged, and the entire ureter should be carefully palpated as calculi may easily be missed. Transabdominal or transrectal ultrasonography should be used to confirm the presence and location of ureteral calculi, which most commonly occur near the entrance to the bladder (Fig. 34.9). In horses affected by a nephrolith and/or ureterolith, typical ultrasonographic findings include hydronephrosis, hydroureter, and a hyperechoic structure with acoustic shadowing in either/both the renal pelvis or ureter.5-8 Horses affected by hydronephrosis typically have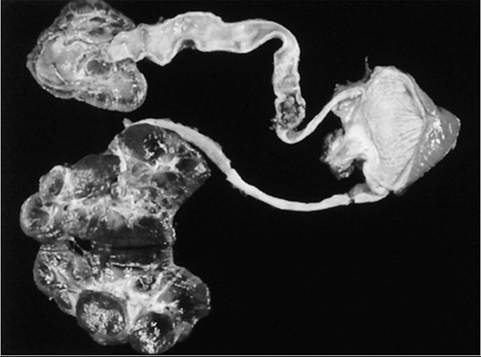
FIG. 34.9 Urinary tract removed from a 5-year-old Standardbred with chronic renal failure caused by intermittent or persistent obstruction by renal and ureteral stones. Note the location of the ureteral obstruction near the bladder. This is the most common site for the obstruction to occur. (Courtesy Thomas J. Divers.)
marked distention of the renal pelvis, thinning of the renal cortex, as well as fibrosis within the kidneys. Serum biochemistry analysis may reveal azotemia in horses with bilateral disease and subsequent CRF, but not in those affected by unilateral disease. Further examination of the urine may reveal isosthenuria, pigmenturia, and microscopic hematuria. Culture of the urine and calculus/calculi is worthwhile, especially in the presence of pyuria, bacteriuria, and in horses with systemic indications of infection (e.g., pyrexia, alterations in the complete blood count and inflammatory markers). Calculi should also be analyzed, and the mineral composition determined.
Nephrectomy should be considered in horses affected solely by unilateral nephrolithiasis without the presence of renal azotemia and concurrent damage to the contralateral kidney.9,10 The advantages of a nephrectomy include prevention of calculus reoccurrence and elimination of any unilateral upper UTI.
A nephrostomy or ureterotomy can be performed to manage ureteroliths.11,12 Transendoscopic laser or electrohydraulic lithotripsy may be considered for noninvasive fragmentation of ureteral stones; however, this technique is time-consuming and often causes tissue trauma.
FIG. 34.10 A large cystic calculus composed of calcium carbonate crystals retrieved from a 17-year-old mare through manual distention of the urethra. Note the easily recognizable spiculated surface that caused chronic cystitis.
The mare had urinary incontinence with perineal and hindlimb scalding (see Fig. 34.5).
Cystic Calculi
Cystolithiasis is most commonly observed in geldings.13 Typically, cystic calculi present as single, large, spiculated stones composed of CaCO3 crystals (Fig. 34.10).1 Less often, calculi consisting of both CaCO3 and CaPO4 crystals may be found; these tend to be smooth and are resistant to fragmentation.13,14 Although the precise etiology is unknown, contributing factors may include neurologic disease causing bladder dysfunction, renal injury, incomplete bladder emptying, underlying cystitis, anatomic defects, bladder trauma or surgery, and neoplasia. Although equine urine is normally supersaturated with CaCO3 crystals, in the healthy horse, the secretion of mucus produced by glands in the renal pelvis and proximal ureter serves as a lubricant to prevent crystal adherence to the uroepithelium.
Clinical symptoms in horses affected by cystic calculi include intermittent hematuria, stranguria, polyuria, dysuria, oliguria, and incontinence. If chronic, then weight loss; urine scalding of the ventral abdomen, preputium, perineum, and hind limbs (see Fig. 34.5); and intermittent colic may occur. The presence of cystic calculi can be confirmed by palpation of the bladder per rectum following bladder catheterization to remove urine.
Advanced diagnostics such as US and cystoscopy should be employed. Due to the possibility of calculi present in multiple locations, US of the entire urinary tract should be performed.1 Cystoscopy allows improved planning for extraction of the calculus or calculi (size vs. shape and quantity), determines the degree of luminal obstruction and mucosal damage, and allows for visualization of urine production from both ureteral openings. Due to urine volume, mucoprotein secretion, and normal sediment, the bladder may require lavage and suction before a complete cystoscopic examination can be performed. It is important to be able to differentiate between sediment and the presence of calculi in the bladder. Sabulous urolithiasis is the accumulation of urine sediment in the ventral aspect of the bladder and often occurs with a concurrent encrusted cystitis and infection (Fig. 34.11).15-17 In turn, over time, sabulous urolithiasis itself leads to a degree of bladder paralysis (myogenic dysfunction), thereby creating a vicious cycle of incomplete voiding, which further predisposes the patient to urolithiasis. Long-standing sabulous cystitis with inherent bladder paralysis may lead to sabulous urolithiasis in the form of an inspissated sphere.16 Care must be taken to avoid confusing inspissated sabulous urolithiasis with the presence of discrete cystoliths.
FIG. 34.11 Encrusted cystitis and sabulous urolithiasis due to infection with Corynebacterium matruchotii in a 17-year-old Quarter Horse ? Thoroughbred gelding. Note the accumulation of crystalloid sludge and ulceration of the bladder mucosa. (Reprinted with permission from the Journal of American Veterinary Medical Association.)
Hematology and serum biochemistry are usually normal with cystolithiasis, but elevation of inflammatory markers should raise suspicion for concurrent upper UTI, and azotemia should prompt careful investigation for concurrent upper urinary tract disease and CRF.
In addition, cytology and culture of an aseptically collected urine sample and culture of a bladder mucosal biopsy may expand the minimum database and help initiate appropriate antimicrobial therapy.Using sedation and caudal epidural anesthesia, small fragmented calculi may be manually removed using a perineal urethrotomy in male horses.13 Care must be taken to avoid further soft tissue trauma and damage to the pelvic urethra, bladder, and rectum. Larger calculi may need to be removed by laparocystotomy through a paramedian, ventral midline incision or with laparoscopic guidance under general anesthetic.18-20 It is the author's (MNS) opinion that the most superior surgical technique is laparocystotomy under general anesthetic, as this allows complete removal of the calculus without fragmentation, thereby reducing the chance of reoccurrence and urethral obstruction, as well as postoperative cystitis and urethritis. Most recently, successful laparoscopic removal of cystic calculi has been described in standing sedated horses, which has the advantage of avoiding general anesthe- sia.21,22 Gokel's cystotomy, using a perirectal incision, can also be used to remove intact, cystic calculi in the standing horse.23 In mares, following caudal epidural anesthesia and manual distention of the urethra, calculi may be easily retrieved intact. Laser (Ho:YAG or pulsed dye laser) or shock wave lithotripsy in the standing horse is also an attractive, noninvasive treatment option for fragmenting large stones.24 Electrohydraulic lithotripsy can be used transendoscopically or via a perineal urethrotomy to fragment large calculi using electrical energy; however, this technique is time-consuming and results in many fragments, which can cause obstruction.25 It is important to submit retrieved stones for analysis and mineral composition. Management of sabulous cystitis has been described in five horses for up to 3 years with medication in combination with bladder catheterization and lavage.17
Unfortunately, calculi may frequently reoccur regardless of treatment modality.
Horses with perineal urethrostomy tend to have greater incidence of reoccurrence than horses with cystotomy most likely due to remaining fragments of calculi. As the precise etiopathogenesis is unknown, preventative measures are difficult to prescribe. Recommendations include urinary acidification with ammonium chloride (50 to 200 mg/kg q24h PO) or ammonium sulfate (200 to 300 mg/kg q24h PO) and changing from a diet of legumes to grass hay to help decrease urinary calcium excretion.26,27 Lastly, the addition of 25 to 50 g NaCl in the feed daily may help promote diuresis by stimulating increased water intake.Urethral Obstruction
Urethral obstruction is typically caused by urethroliths located over the ischial arch where the urethra is narrowest. These stones may move further distally and cause luminal obstruction (see Fig. 34.12, A and B). Mares seldom develop urethral obstruction due to a much shorter, nontortuous, and more distensible urethra. Patency of the urethra may also be affected by neoplasia, congenital disorders, edema, inflammation, and trauma. Should complete urethral obstruction persist, bladder rupture is likely to develop and can be confirmed by abdominal ultrasonography and paracentesis of urine in the abdomen.
Urethral obstruction is best diagnosed by careful urethroscopy. Therapeutic urethroscopy may be used for direct retrieval of stones, thereby minimizing potential trauma, mucosal irritation, and stricture formation. Retrieval of urethroliths that are large and immovable may be performed by a perineal urethrostomy or a distal urethrotomy. However, this may lead to urethral stricture formation and urine fistulization. Urethroscopic lithotripsy can be considered if instrumentation is available. Radial extracorporeal shockwave therapy may be also considered for urethrolith fragmentation in the male horse.28 In horses with urothelial tumors, ureteroscopy will allow improved visualization and treatment by resection using a Nd:Yag laser. Larger obstructive tumors such as squamous cell carcinoma affecting both the penis and prepuce may be treated by surgical resection with topical application of 5-fluorouracil.
More on the topic Urolithiasis and Obstructive Disease:
- Smith Bradford P., Van Metre David C., Pusterla Nicola (eds.). Large Animal Internal Medicine. Part 2. 6th edition. — Elsevier,2020. — 2279 p., 2020
- Overview of Conditions Affecting the Caprine UrinarySystem
- REFERENCES
- Crystalluria
- Urinary Tract Infections
- Dysuria, Stranguria, and Incontinence
- Weight Loss
- Surgery of the Male Reproductive Tract