Fungal Diseases
Stephen D. White
Dermatophytosis (Ringworm)
Dermatophytosis refers to infections of the keratinized tissues of the skin (stratum corneum layer of epidermis, hair, claws, hoof, and horns) by Microsporum and Trichophyton spp.
Dermatophytosis is relatively common in the horse and in cattle, less common in goats, and rare in sheep.■ Etiology and Pathogenesis The most common dermatophyte species isolated from horses are Trichophyton equinum, Microsporum equinum, Trichophyton mentagrophytes, and Trichophyton verrucosum.1- T. verrucosum infections in humans caused by transmission from horses have been reported.4 In ruminants the majority of dermatophytosis lesions are caused by T. verrucosum and to a lesser extent by T. mentagrophytes.5 Transmission of the disease is usually from animal to animal by direct contact or indirectly through fomites such as grooming instruments, tack, housing, fencing, or feed bunks. The incubation period may range from 1 to 6 weeks.
Several factors may influence the susceptibility of an animal to dermatophyte infection. Age is probably most important, with younger animals more susceptible to infection. The susceptibility of young animals is most likely related to lack of prior exposure or infection and thus no immunity, as well as crowding of young animals and conditions that decrease resistance to infection (e.g., poor nutrition). Environmental factors like warmth and humidity also may play a role. Calves kept indoors or exposed to foggy weather with little or no sunlight have an increased incidence.
Under normal circumstances, dermatophytes only invade fully keratinized, nonliving tissues.1 This results in weakened hair shafts, leading to alopecia.
In many cases, dermatophytosis is theorized to be a selflimiting disease, with the duration of infection ranging from 1 to 4 months.
The spontaneous regression is at least partly related to the development of immunity, of which cell-mediated immunity is the more important. The immunity that develops is probably not complete, and its duration is unknown.■ Clinical Signs The lesions are often circular; usually appear first on the face or in the axillary/girth area; and may spread over the trunk, rump, neck, head, and limbs (Fig. 40.10). Occasionally in the horse, dermatophytoses may be limited to the pastern region. Rarely, dermatophytes may be a cause of coronary band disease in horses. The mane and tail are rarely involved. Cattle and goats are frequently affected around the eyes and face (Fig. 40.11, Color Plate 40.7).
Lesions may be superficial or deep. Superficial infections are much more common and manifest with development of thick crusts or more generally a diffuse moth-eaten appearance with desquamation and alopecia, sometimes in a ring pattern. A small crust may form over the follicle, and the hair is lost. Occasionally the initial lesions may be urticarial, progressing to multifocal, sharply demarcated areas of alopecia and scaling. The degree of pruritus varies but is usually mild or absent. Erythema is usually absent or obscured by pigmented skin.
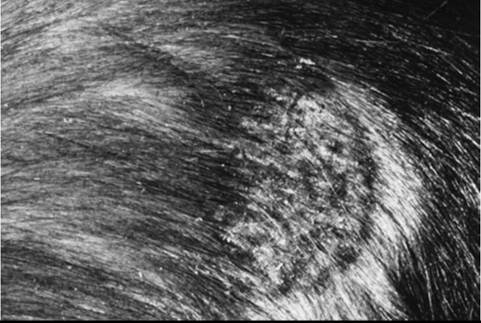
FIG. 40.10 Ringworm lesion (due to Trichophyton spp.) in a horse’s flank area.

FIG. 40.11 Ringworm lesions (due to Trichophyton verrucosum) around a calf’s eye.
The lesions in cattle are usually characterized by excessive crusting, taking on an almost wartlike appearance.
Dermatophytosis must be considered in the differential diagnosis of any dermatoses characterized by multifocal alopecia or scaling and crusting. For a solitary lesion in horses, the occult sarcoid is the primary differential diagnosis. The two most important differential diagnoses of more extensive lesions are dermatophilosis and pemphigus foliaceus.
■ Diagnosis Direct microscopic examination of infected hairs is of value, but in general the most common and reliable method of diagnosing dermatophytosis is fungal culture (see Chapter 11). Broken hairs at the periphery of lesions are most satisfactory for this purpose. Large crusts should be avoided. The use of specialized indicator media is preferred. On occasion, dermatophytosis is diagnosed histopathologically. Interestingly, Trichophyton spp. occasionally may cause acantholysis, mimicking pemphigus foliaceus on histopathology.6 As with other infectious diseases, the role of PCR is being investigated for diagnostic accuracy.7
■ Therapy Although 50% captan (2 tablespoons powder in 1 gallon water) has been recommended in the past and is certainly safe for tack, its effectiveness on the animal has been questioned. Lime sulfur (LymDyp [IVX Animal Health, St. Joseph, Mo.], LymDyp DVM [Bayer, Shawnee Mission, Kan.], LimePlus dip [Dechra, Overland Park, Kan.]), 1 cup to 1 gallon of water, and bleach 1 : 10 with water are both effective but messy, odiferous, and staining. Shampoos containing miconazole, ketoconazole, and/or 3% to 4% chlorhexidine may be effective. In Europe and Canada an enilconazole rinse (Imaveral [Merial, Baie d’Urfe, Canada]) approved for horses and cattle is highly effective.
Systemic treatment is occasionally needed. The efficacy and proper dose of griseofulvin in horses has not been thoroughly researched, but we have advocated and used a dosage of 100 mg/kg PO daily for 7 to 10 days on a small number of horses. Griseofulvin is a teratogen and should not be used in pregnant mares. Alternatively, 20% sodium iodide (NaI) may be given IV (250 mL/500-kg horse once or twice every 7 days) but is also contraindicated in pregnant mares because it may cause abortion.2
Vaccinating cattle against T verrucosum has long been successful in Eastern Europe and Scandinavia. Effective control of ringworm in cattle has been achieved in regions implementing systematic vaccination.8 Vaccination against T.
equinum in horses may reduce the incidence of new infections and protect a high percentage (>80%) of vaccinates from infection. These data are based on results with an inactivated vaccine containing both conidia and mycelial elements.9 In cattle, newer vaccines consisting of recombinant protein and deoxyribonucleic acid (DNA) derived from heat shock protein 60 of T. mentagrophytes have shown success experimentally.10 Such vaccines are not yet available in the United States.Malassezia Dermatitis
The exact species of the yeast Malassezia growing on large animals’ skin is just beginning to be investigated.11 In one study of horses and livestock, the Malassezia spp. isolated were identified as Malassezia furfur, Malassezia slooffiae, Malassezia obtusa, Malassezia globosa, and Malassezia restricta.n We have examined several mares with a Malassezia infection between their mammary glands that was intensely pruritic. The mares rubbed their tails and ventral abdomens. Physical examination showed a dry, greasy-to-the-touch exudate. Cytology of the exudate showed numerous yeast organisms, which were identified on culture as Malassezia spp. Treatment with a topical 2% miconazole/chlorhexidine shampoo was curative. We are aware of other similar cases. However, healthy nonpruritic mares may also have large numbers of yeasts in the intramammary area.13
Sporotrichosis
Sporotrichosis is caused by the yeast Sporothrix schenckii, which is most common in vegetation. The yeast becomes pathogenic in animals because of its dimorphic ability to convert from a yeastlike form at tissue temperatures between 35° and 37° C (95° and 98.6° F) to a mycelial phase (with branching, septate hyphae) at environmental or laboratory temperatures of 25° to 30° C (77° to 86° F).14 The disease has been reported in many species of domestic animals.
The initial lesions are nodules, which frequently ulcerate, and the disease may progress to a lymphatic-cording disease.
Rarely, the fungus will eventually spread to the lungs. In a retrospective study from UCD-SVM, equines were the second most common species affected, after cats.15 Diagnosis is made by demonstrating the organism on histopathology, immuno- fluorescent antibody testing on affected tissues, impression smears, and culture.15,16 This is a zoonosis, so care should be taken when handling suspected samples.Successful therapy with a number of different systemic iodine preparations (NaI, KI) has been reported. Organic iodides have proved to have superior efficacy to inorganic iodides in treating equine sporotrichosis, with ethylenediamine dihydroiodide (organic iodide powder [Neogen Corp., Lexington, Ky.] or EDDI 20 Gr. Dextrose base [Vedco, St. Joseph, Mo.]) being a commonly used preparation. This product is in the form of a feed additive and can be mixed with a small amount of grain and administered at 1 to 2 mg/kg of the active ingredient once to twice daily for the first week, then 0.5 to 1 mg/kg once daily for the remainder of the treatment. In general, lesions will begin to regress during the first month of treatment, and therapy should be continued for at least 1 month beyond complete resolution of all cutaneous nodules and healing of any ulcerated lesions. Prematurely discontinuing therapy will invariably result in an unnecessary relapse of the disease. During treatment, the horse should be closely observed for any evidence of iodide toxicity (iodism), which includes excess scaling and alopecia, a serous ocular or nasal discharge, excess salivation, anorexia, depression, coughing, nervousness, or cardiovascular abnormalities. Should any of these signs develop, the treatment should be discontinued for 1 week, then resumed at three quarters the dosage at which the iodism was noted. In most cases the treatment is subsequently well tolerated.17 Although both itraconazole and terbinafine have been shown to be effective in vitro against the organism isolated from a horse, there is an absence of clinical reports of their use.18 Successful management of an infected donkey with both KI and fluconazole has been reported.15
Histoplasmosis
Histoplasma capsulatum var.
farciminosum (“farcy,” the cause of equine epizootic lymphangitis in East Africa) infection has been reported in donkeys, where it can have considerable economic impact.19 Cutaneous lesions resemble those seen in sporotrichosis. Treatment has not been well established but may be similar to the treatments for S. schenckii.Phaeohyphomycosis
Phaeohyphomycosis is caused by a number of ubiquitous fungi that are either saprophytes or plant pathogens. These include Alternaria, Drechslera, Cladophialophora, Cladosporium, Phialophora, and Stemphylium spp. The correct terminology currently depends on the histologic appearance of the organism, as follows20:
• Chromomycosis: any pigmented fungi
• Chromoblastomycosis: pigmented fungi, primarily yeast
• Phaeohyphomycosis: pigmented fungi, both hyphal elements and yeast
• Hyalohyphomycosis: nonpigmented fungi, mainly hyphal elements
Cutaneous lesions arise from either trauma to the skin or disseminated disease. Animals with disseminated disease probably have a deficient immune system. Similar to the other deep mycoses, these lesions present as expanding nodules and draining tracts. Diagnosis is by biopsy or occasionally cytology. Histopathology shows foamy or epithelioid macrophages, and special stains will show the organisms. Veterinarians and their staff should be careful in handling material from infected animals, because the inadvertent inoculation of these organisms can cause human infections.
Treatment has generally included surgical excision or amputation if practical. Potassium iodide, as for sporotrichosis, and (if the owners can afford it) fluconazole per os at 5 mg/ kg may be effective.
Zygomycosis
Similar to phaeohyphomycosis, zygomycosis is caused by a number of related fungal species that are ubiquitous saprophytes. GI and respiratory tract involvement is possible. Cutaneous lesions are thought to be caused by wound penetration. The disease typically occurs in tropical and subtropical areas. The two orders of Zygomycetes that cause disease are Mucorales, including the genera Rhizopus and Mucor, and Entomophthorales, including the genera Conidiobolus and Basidiobolus. Most cutaneous reports are in horses, although ruminants may have other organ systems affected.
The skin disease is ulcerative, nodular, and generally found on the trunk and neck. Generally, only one large nodule is present. Diagnosis is by histopathology and culture; a serum agar immunoprecipitation test has been useful in diagnosing conidiobolomycosis. Surgical removal, if possible, is preferred for treatment. Medical options include the iodides (not effective against the order Mucorales) and possibly the azoles or amphotericin B.1
Pythiosis
Pythium insidiosum is considered to be the causative agent of swamp cancer, also known as Florida horse leech, bursattee, and kunker. This organism is termed a protista and is found in tropical and subtropical areas worldwide, although its range may be expanding; it recently has been reported in a horse in northern California.21 The pythiosis lesion occurs most often on the limbs, abdomen, neck, and lips and consists of dense granulation tissue containing masses of yellow-gray necrotic tissue, which sometimes are calcified and often are present as cores in fistulae and are removable intact. Such masses are known as leeches or kunkers. The granuloma ulcerates and extends peripherally and may reach a very large size in a short time. The overlying and adjacent skin is destroyed by both the inflammatory reaction and the self-mutilation by the horse. Important differential diagnoses are systemic fungal infections, habronemiasis (“summer sore”), and neoplasia. Although most reports in large animals are in horses, cattle, sheep, and goats may also be affected.22-24
Histopathologic examination of affected tissue reveals pyo- granulomatous inflammation directly surrounding the organism. Isolation of organisms from the lesions is necessary for further identification and study, but histologic demonstration of the protozoa within tissues reacting to its presence is critical in establishing the causal relationship in an individual lesion. In obtaining culture, the kunkers are preferred to the actual tissue. For samples that cannot be processed immediately, acceptable handling techniques include storage at room temperature for up to 3 days, refrigeration for up to 5 days, shipping on cold packs, and storage in antibiotic solution, each combined with subsequent inoculation on selective media.25 Recent advances in enzyme-linked immunosorbent assay (ELISA) or molecular techniques offer better potential for organism detection and identification.26 Wide surgical excision combined with or without immunotherapy has been effective in some cases.26-28