Hypersensitivity Disorders
Stephen D. White
Atopic Dermatitis
■ Definition and Etiology Atopic dermatitis can be defined as an abnormal immunologic response to environmental allergens like pollens, barn dust, and molds.
It is increasingly being recognized as a cause of pruritus in horses. The disease may be seasonal or nonseasonal, depending on the allergens involved. Age, breed, and gender predilections have not been extensively reported. A familial predisposition may be present.1The presumed etiology is a type I (immediate) hypersensitivity response mediated by IgE. Evidence indicates that atopic horses do produce allergen-specific IgE2,3; the IgE is presumed to be directed against specific allergens. When that allergen is bound to two or more IgE antibodies on the surface of a mast cell, the mast cell releases granules containing various substances that cause erythema, vascular leaking, and pruritus.
■ Clinical Signs Pruritus, often affecting the face, distal legs, or trunk, is the most common clinical sign. Alopecia, erythema, urticaria, and papules may all be present. Urticarial lesions may be severe but nonpruritic. In one study of 54 horses with atopic dermatitis, 28 horses had urticaria, 8 had pruritus, and 18 had both.3 Horses may have a secondary pyoderma typified by excess scaling, small epidermal collarettes, or encrusted papules (miliary dermatitis). Diagnosis of atopic dermatitis is based on clinical signs and exclusion of other diagnoses, especially parasite (Culicoides) allergy.
■ Diagnosis Diagnosis is based on clinical signs and exclusion of other pruritic skin disease. Confirmation to formulate allergen-specific immunotherapy (ASIT [hyposensitization]) is based on either intradermal testing (IDT) or serum allergy tests. IDT involves a series of intradermal injections of aqueous allergen extracts along with a positive (histamine) and negative (saline) control.
Injections are usually performed over the lateral cervical or thoracic region, and the sites are then observed for 30 minutes to 24 to 48 hours for evidence of wheal formation. A positive reaction does not necessarily mean that the horse's clinical signs are caused by the reacting allergen, but rather that the horse has antibodies to the allergen that, on intradermal exposure, cause wheals to form. False-negative IDT reactions may occur, the most important cause of which is the use of corticosteroids, antihistamines, or phenothiazine tranquilizers before testing, especially within the previous 14 days.4Horses with atopic dermatitis generally have a higher incidence of positive reactions than healthy horses, but the diagnosis (as in other species) cannot be solely made based on the IDT or serologic test alone. Such tests should be interpreted by considering the history of the disease. For example, a horse with seasonal signs is more likely to have an allergic response to seasonal allergens (pollens in summer, barn dust in winter). This interpretation will help the clinician determine which allergens might be relevant in hyposensitization, should the owners choose that treatment.2,3,5-7
IDT and available serologic tests look for allergen-specific IgE in the animal's blood,8 but the latter's use on horses and other domestic species is not without controversy. One study showed no statistical difference in the efficacy of hyposensitization between horses tested with IDT and those tested with serology.3 Preferentially, IDT and/or serologic testing are performed on horses with atopic dermatitis that have owners interested in pursuing hyposensitization. It should be remembered that, in regard to food allergy, neither serologic testing nor IDT likely has any relation to reality. Clinical research is ongoing to determine the most important allergens, their testing dilutions, and effective control substances.9,10
■ Therapy Corticosteroid treatment is usually effective in the control of pruritus or urticaria due to atopic dermatitis.
The usual oral medication used is prednisolone (1 mg/kg PO q24h), although dexamethasone (0.05 mg/kg PO q24h) can also be used. The injectable dexamethasone solution may be used orally, although the clinician should remember that the bioavailability is 60% to 70% of the injectable route.Corticosteroids in horses may cause various adverse effects, including steroid hepatopathy, laminitis, and iatrogenic hyper- adrenocorticism. Therefore other modalities of treatment may be used, such as the antihistamine hydroxyzine pamoate (200 to 400 mg/500 kg PO q12h) or cetirizine (0.2 mg/kg PO q12h); doxepin, a tricyclic antidepressant with antihistaminic effects (300 to 600 mg/500 kg PO q12h); or diethylcarbamazine syrup (6 to 12 mg/kg PO q24h). Hydroxyzine, cetirizine; and doxepin may cause either drowsiness or nervousness, although these adverse effects are uncommon. Cetirizine is expensive; because it is the active metabolite of hydroxyzine, if the latter is ineffective in an individual horse, cetirizine probably will be as well. Pyrilamine maleate, though often used in the horse, in fact has poor oral bioavailability.11 Some clinicians have noted improvement when an essential fatty acid (EFA) product is added to the feed. Platinum Performance (Platinum Performance Inc., Buellton, Calif. [Dr. W. Rosenkrantz, personal communication, 2004]) has been used successfully in some atopic horses as an adjunctive treatment.
In general, hyposensitization injections for any manifestation of atopic dermatitis in the horse should be evaluated for efficacy for at least 12 months. The veterinarian should maintain consistent communication with the client to monitor the progress of treatment and encourage the owner to continue with the injections for the full year. Although most horses will need to be maintained on injections for life, if hyposensitization is successful, perhaps as many as 25% may be able to discontinue the treatment without recurrence.3 Experience at the University of California, Davis, School of Veterinary Medicine (UCD-SVM) shows that about 65% to 70% of atopic horses improve with hyposensitization3,12; other researchers have reported even better results but in a noncontrolled study.13
Urticaria
■ Definition and Etiology Urticaria is characterized by transient focal swellings in the skin or mucous membranes called wheals, which represent localized areas of dermal edema.
Angioedema is essentially identical but involves the subcutaneous tissues. The swelling of angioedema is diffuse, often involving the entire face and neck of the animal.Urticaria is more frequently recognized in the horse than in ruminants. Allergic urticaria is usually caused by atopic dermatitis (environmental allergens like pollens),1,6,7,14 drug eruptions (especially from antibiotics15 and nonsteroidal antiinflammatory drugs [NSAIDs]), contact allergies, and food allergies (rarely).16 Physical urticarias are less common and involve a nonimmunologic pathogenesis. The three most important categories are mechanically induced, such as dermatographism, essentially a “pressure” urticaria; cold urticaria; and exercise-induced urticaria. Miscellaneous diseases that can cause urticaria include dermatophytosis (initial lesions),17 pemphigus foliaceus, “stress” (sometimes seen in racehorses immediately before a race), and vasculitis (Box 40.1). Urticaria is a recognized manifestation of milk allergy in cattle.18
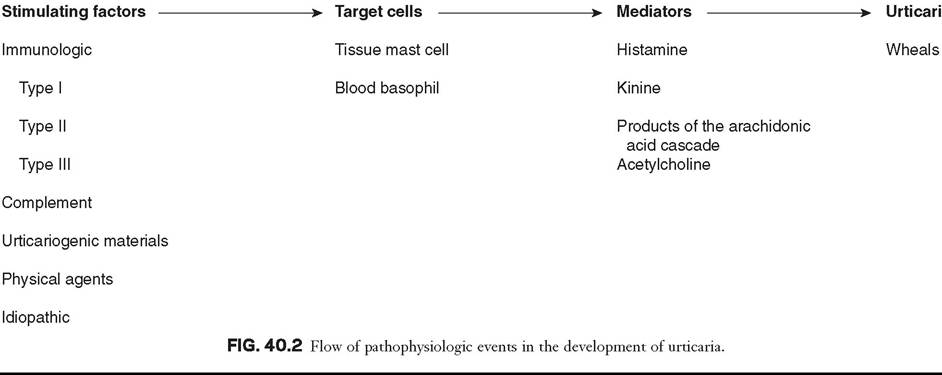
■ Pathophysiology The wheals result from vasodilation and transudation of fluid from capillaries and small blood vessels. Both immunologic and nonimmunologic factors can trigger release of mediators from mast cells and blood basophils that will ultimately produce the characteristic wheals (Fig. 40.2). The most frequently cited immunologic mechanism of urticaria is type I hypersensitivity (IgE). Non-IgE-dependent, immune-mediated urticaria may be induced by either type II (cytotoxic, involving antibody and complement) or type III (immune complex) hypersensitivity reactions. Complement- activated urticaria may involve either immunologic or nonimmunologic mechanisms and may occur through either the classic or the alternative pathway. Urticariogenic materials can induce wheal formation without involving immunologic mechanisms by being ingested, injected, or contacting the animal. Physical agents, including mechanical injury, thermal changes, and solar radiation, may induce urticaria.
An example of mechanically induced urticaria is dermatographism (whealing after blunt scratch injury to the skin). Local or generalized exposure to heat or cold may induce urticarial lesions in certain individuals.■ Clinical Signs and Differential Diagnosis Wheals range from 1 to 10 cm (0.4 to 4 inches) in diameter and tend to involve the cervical and craniolateral thorax (Fig. 40.3). The animal may or may not be pruritic. Alopecia is not usually a feature of urticaria. The most important factor in distinguishing urticaria from other nodular diseases is that the individual lesions pit with pressure. This is easily demonstrated in the
■ BOX 40.1
Possible Causes of Urticaria in Horses and Ruminants
Allergic Urticaria
Inhalants
Pollens, animal danders, mold spores, feather down, aerosols, smoke, dust, and volatile chemicals
Injectants
Drugs, diagnostic agents, vaccines, insect stings, serums, and blood
Ingestants
Drugs, various food items, beverages, and occult additive materials found in foods
Infections
Foci of bacteria, fungal, viral, and parasitic infections
Contactants
Animal products, plant materials, cosmetics, plastic, and other chemicals
Drugs
Penicillin, aspirin, quinine, sulfonamides, insulin, and many others
Milk Proteins
Milk retention (cattle)
Urticaria Caused by Urticariogenic Materials
Drugs
Cocaine, morphine, codeine, atropine, quinine, thiamin, pilocarpine, polymyxin B, D-tubocurarine, dextran, dehydrocholate sodium (Decholin), and other drugs
Foods
Certain citrus fruits, strawberries, and certain fish
Toxins
Cobra venoms, jellyfish toxin, and certain plant and insect toxins
Physical Urticaria
Dermographic (induced by blunt-scratch injury)
Heat
Cold
Light
Miscellaneous Urticaria
Erythema multiforme
Pemphigus foliaceus
Infections
Collagen vascular disease
Neoplasia
Psychogenic
early stages of wheal formation, when the lesions consist primarily of dermal edema.
In the later stages, when there is cellular infiltration into the dermis, the pitting is less apparent.■ Diagnosis Urticaria is usually a clinical diagnosis; the diagnostic dilemma is to determine the cause of the urticarial eruption. A skin biopsy not only will lend support to the clinical diagnosis of urticaria but also may show evidence of pemphigus foliaceus, dermatophytosis, or vasculitis. Initiation of ectoparasite control, IDT or serologic tests for atopic dermatitis, fungal culture, skin biopsy, and feed trials may all be used to determine the underlying disease.14
■ Therapy Avoiding the allergen or initiating factor or treating the underlying disease is the best therapy. When this is not possible or when the allergens cannot be identified, medical therapy should be used, as described in the Atopic Dermatitis section.
Milk Allergy
The principal cutaneous manifestation of milk allergy is urticaria and is usually seen in cows during the drying-off period. Increased intramammary pressure presumably causes milk proteins to gain access to the circulation, where they induce a type I hypersensitivity reaction.19 The disorder is believed to be hereditary and familial, with cattle of the Channel Island breeds demonstrating increased susceptibility.
The urticarial reaction can be localized or generalized. Other clinical signs that may be noted include muscle tremors, respiratory distress, restlessness, ataxia, dullness, and even maniacal behavior. Diagnosis is made by observing an edematous swelling at the site of an intradermal injection of the cow's milk or the milk protein casein diluted 1 : 1000, in combination with the appropriate clinical signs.19,20
Treatment involves the use of antihistamines early in the disease. Prevention requires avoiding milk retention. An affected cow is likely to suffer recurrences of milk allergy, so culling is usually recommended.
Erythema Multiforme
Erythema multiforme (EM) has been recognized clinically in the horse and in one bull (Fig. 40.4). This is an immunologic reaction in the skin, and programmed keratinocyte cell death (apoptosis) is the prominent change seen on biopsy. The keratinocytes may be killed specifically by killer lymphocytes. The many possible etiologic factors include infectious diseases, drugs, systemic disease, and neoplasia. In horses, drugs are probably the most frequent inducers of EM, although in many cases an underlying disease is undiagnosed.21,22 In one bull the EM may have been caused by a pyelonephritis found on necropsy.23 Clinical lesions are characterized by macules, papules, urticarial lesions, or vesicular bullous lesions. Individual lesions may expand peripherally, leading to formation of target-like lesions. Scaling and crusting are usually not a feature of equine EM unless the disease is characterized by erosions or ulcers. Individual lesions can persist for several days, unlike urticarial lesions. Pruritus and pain are variable but not usually seen. Lesions may occur in association with or after an infection or drug administration. The late Dr. A.A. Stannard of UCD-SVM had theorized that reticulated and hyperesthetic leukotrichia may also represent a type of EM in the horse,22 although a recent article demonstrated histologic differences between hyperesthetic leukotrichia and EM.24 One report associated EM in a horse with equid herpesvirus 5.25 Interestingly, a similar disease, toxic epidermal necrolysis, has rarely been reported in cattle.26
Differential diagnoses include urticaria, amyloidosis, and other nodular papular diseases. The diagnosis is made based on history, physical examination, and skin biopsies. Histologic changes are distinctive and often include a lichenoid pattern with keratinocyte apoptosis. Vesicular lesions may be present and can include more confluent areas of keratinocyte destruction with massive spongiosis and subepidermal and intraepidermal edema.
Treatment should be directed toward the underlying cause if one can be found. A drug eruption should be high on the list, and searching the history for recent drug administration is important. Although some cases of EM are self-limiting and may resolve within 1 to 3 months,21 corticosteroid treatment as for pemphigus foliaceus may be tried. In our experience, reticulated leukotrichia does not resolve spontaneously and does not respond to corticosteroids.

FIG. 40.3 Acute urticaria in a horse caused by an adverse drug reaction.

FIG. 40.4 Erythe ma multiforme in a horse.
a
Vasculitis
Vasculitis is a histopathologic term that implies the presence of inflammatory changes in the walls of blood vessels, and it is associated with a broad spectrum of disorders. Cutaneous vasculitis is recognized in horses and is most often seen as a feature of photoaggravated dermatitis, drug reactions, or purpura hemorrhagica.27 Mules and donkeys may also be affected.27 Affected vessels may be limited to the skin or may involve other organs, resulting in systemic disease. The cutaneous lesions are characterized by crusts, scales, edema, purpura, necrosis, and ulceration, most often affecting the legs (Fig. 40.5, Color Plate 40.3).
As a clinical entity, phOtoaggravated vasculitis seems to be more common (if poorly understood) in California and the western United States. Although previously termed leukocytoclastic vasculitis, the most common histologic finding is cell-poor and lymphocytic/histiocytic vasculitis.27 It generally affects mature horses and produces lesions confined to the lower extremities that lack pigment, although pigmented legs may also be affected. Lesions are multiple and well demarcated, with the medial and lateral aspects of the pastern the most common sites. Initially, erythema, exudation, crusting, erosions, and ulcerations develop, followed by edema of the affected limbs. Some lesions may have a “punched-out” appearance. Chronic cases may develop a rough or “warty” surface. Pathogenesis is uncertain; an immune complex etiology has been suggested, and when lesions are restricted to nonpigmented areas this suggests a role for ultraviolet (UV) radiation. Drug reactions may be a potential cause.22 One report also implicated Staphylococcus intermedius.2
It must be emphasized that cutaneous vasculitis can occur anywhere on the body and may become generalized.
The differential diagnosis is photosensitization, particularly that caused by contact. The diagnosis is confirmed by skin biopsy, which demonstrates vasculitis, often with vessel wall necrosis and thrombosis involving the small vessels in the superficial dermis. These changes may be difficult to demonstrate.
Treatment involves corticosteroids at relatively high doses (prednisolone at 1 mg/kg PO q12h or dexamethasone at 0.08 to 0.2 mg/kg PO q24h) for 2 weeks, then tapered over the next 4 to 6 weeks. Reducing UV light exposure is helpful, by bandaging affected legs, stabling inside during daylight hours, or both. In some cases, topical corticosteroids (e.g., betamethasone valerate cream 0.1% or triamcinolone spray 0.015%) may enable the horse to be weaned off systemic corticosteroids. Pentoxifylline (8 to 10 mg/kg PO q12h) may be an effective adjunct treatment. Another alternative (but more expensive) is 0.1% tacrolimus ointment q24h (Protopic [Astellas Pharma US, Northbrook, Ill.]). This disease recurs in approximately 25% of cases.27 These horses are prone to secondary bacterial infections, and a month of antibiotic treatment (usually trimethoprim-sulfamethoxizole) is often indicated if the horse has fever or its legs are extensively swollen.
Cutaneous vasculitis seemingly is rare in ruminants; one report in calves describes lesions on the forelegs and ear tips occurring within a month on one farm. Histology showed a fibrinous-necrotic or leukocytoclastic vasculitis. Glucocorticoid (prednisolone) therapy was effective.29 A recent article describes systemic vasculitis (polyarteritis nodosa) in four flocks of sheep.
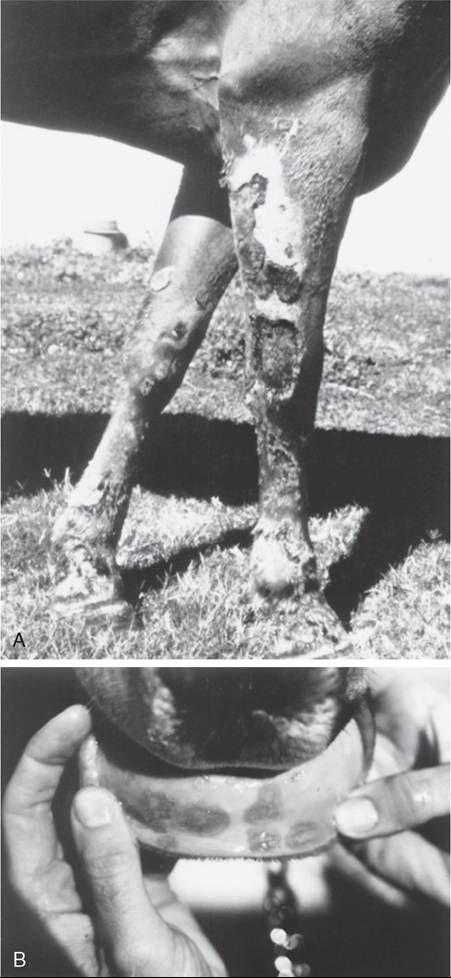
FIG. 40.5 Cutaneous vasculitis in a horse. A, Vasculitis involving forelimbs. B, Vasculitis involving mucous membranes of inner lip.
Clinical and histologic signs involved several organ systems, including the skin.30 Vasculitis and purpura hemorrhagica are discussed in more detail in Chapter 37.
Drug Eruption
A drug eruption is a cutaneous reaction to any agent that enters the circulation by ingestion, injection, inhalation, or percutaneous absorption. Drug eruptions may or may not be associated with systemic signs. Many drug eruptions are thought to be immunologically mediated hypersensitivity reactions, although on occasion they may occur with the initial administration of a drug and therefore without any prior sensitizing

FIG. 40.6 Drug eruption in a horse; note pruritus.
exposure, characteristic of an immunologic reaction. Drug eruptions may also occur after years of repeated asymptomatic exposure to a drug, although this is probably less common than formerly supposed. Any medication can cause a drug eruption, but the compounds most frequently incriminated include antibacterial agents (especially semisynthetic penicillins and the sulfas), phenothiazine tranquilizers, NSAIDs and antipyretics (especially phenylbutazone), local anesthetics, and anticonvulsants. In general, the more recently a drug has been given, the more likely it may be the cause of a skin disease. The clinician should try to determine a temporal association between administration of the drug and the skin disease.
Because drug eruptions can result in a wide variety of cutaneous manifestations, they must be considered in the differential diagnosis of all skin disorders. Certain clinical symptoms are more often associated with drug eruptions. Urticaria and angioedema, diffuse erythema, papular rashes, intense pruritus that responds poorly to corticosteroids (Fig. 40.6), sharply demarcated ulcers secondary to vasculitides, vesicular and bullous eruptions, and photosensitization should arouse clinical suspicion of a drug eruption. Typically, cutaneous lesions are noted 24 to 48 hours after drug administration, although there may be a longer lag interval. The eruption usually subsides within 24 to 48 hours after exposure ceases, although lesions may persist for up to 6 months after the offending agent is eliminated.22
A diagnosis of drug eruption is based on clinical suspicion associated with an incriminating history of drug administration and by ruling out other possible causes. In a suspected case, all medications should be discontinued. If life-saving medications are being administered, a chemically unrelated compound with similar pharmacologic effects should be substituted. Administration of corticosteroids may provide some relief, but drug eruptions respond variably to corticosteroids. Although development of a cutaneous reaction after readministration of the suspected agent would support a diagnosis of drug eruption, readministration is not advisable because it can be fatal as well as unethical. Future exposure to any implicated compounds and chemically related substances should be avoided.
Contact Dermatitis
■ Definition and Etiology Contact dermatitis is recognized in both horses and ruminants and can be subdivided into irritant and allergic contact dermatitis. Irritant contact dermatitis occurs more often and is defined as a cutaneous reaction to an irritating concentration of an offending agent. The substance chemically damages the skin without immunologic mediation. The reaction may occur after a single contact with a strong irritant or after repeated contacts with a milder irritant. Allergic contact dermatitis represents a cutaneous reaction in a sensitized animal to a nonirritating concentration of the offending agent. Tissue damage is immunologically mediated by delayed-type hypersensitivity (type IV), so prior exposure is required to sensitize the skin to the material eliciting the dermatitis.16,18 It may be difficult to differentiate between the two types of contact dermatitis, and it may not be clinically important. In our experience, the vast majority of contact dermatitis cases are iatrogenic, caused by topical products placed on the skin by veterinarians or owners.
■ ClinicalSigns The clinical lesions associated with allergic and irritant contact dermatitis are very similar. Predisposed areas include the muzzle, extremities, and areas contacted by tack. Early lesions include erythema, edema, and vesiculation that progress to erosions, ulcerations, and crusting and ultimately to lichenification and hyperpigmentation. A gravity- induced drip pattern may be evident when the irritant is a liquid.31
■ Diagnosis A detailed history is very important—the bedding, all topical products and blankets, and other potential environmental antigens and irritants should be noted. Certain woods release various irritant oils and have been implicated when incorporated into the bedding.32 Patch testing is possible but usually impractical. Provocative exposure is the most useful test for diagnosis of contact dermatitis, although it does not reliably distinguish between allergic and irritant contact dermatitis. It requires avoiding contact with all suspected agents for 7 to 10 days to permit clearing of the skin lesions. The patient is then reexposed to these agents on an individual basis at 7- to 10-day intervals while being observed for recurrence of the dermatitis. When a positive reaction is observed, challenge with the suspected agent should be repeated to confirm the diagnosis. The process is time consuming, requiring owner patience and cooperation.
■ Therapy An animal with a suspected or confirmed diagnosis of acute or irritant contact dermatitis should be placed in an environment where there is negligible chance of exposure to agents that might have produced the dermatitis. Symptomatic treatment pending spontaneous resolution includes gently washing the affected regions with water. Pentoxifylline at the dose noted earlier for vasculitis may be helpful in horses.