Bacterial Diseases
Stephen D. White
Dermatophilosis (Streptothricosis, Rain Scald, Lumpy Wool, Strawberry Foot Rot)
■ Definition and Etiology Dermatophilosis is caused by an actinomycete bacterium, Dermatopbilus congolensis.
The organism is a gram-positive, non-acid-fast, branching, filamentous, aerobic bacteria that divides longitudinally and then transversely to form parallel rows of coccoid zoospores. Dermatophilosis affects horses, cattle, sheep, and goats, as well as a wide range of other mammals.1-4Three conditions must be present for Dermatopbilus to manifest: a carrier animal, moisture, and skin abrasions. Chronically affected animals are the primary source of infection, but they become a serious source of infection only when their lesions are moistened, which results in release of zoospores, the infective stage of the organism. Mechanical transmission of the disease occurs by both biting and nonbiting flies, ticks, and possibly fomites. Because normal healthy skin is impervious to infection with D. congolensis, some predisposing factor that results in decreased resistance of the skin, especially prolonged skin wetting by rain, is necessary for infection to occur. The organism has been isolated from the environment of affected animals. Distribution is worldwide, but frequency of occurrence of dermatophilosis varies with geographic location; areas with increased rainfall are predisposed. There is no apparent age, breed, or gender predilection.
■ Clinical Signs Dermatophilosis is usually seen during the fall and winter months, with the dorsal surface of the animal most often affected (Fig. 40.7, Color Plates 40.4 and 40.5). In horses, this association with the wetter months of the year has led to the term rain scald. Occasionally the lesions involve the lower extremities when animals are kept in wet pastures (“dew poisoning”) or if horses are left in the stall while the stall is cleaned with high-pressure water hoses.
In the early stages of disease, the lesions can be felt more easily than they can be seen. Thick crusts can be palpated under the hair coat. Removing the crusts and attached hair exposes a pink, moist skin surface, with both the removed hair and the exposed skin assuming a paintbrush shape. The undersurface of the crusts is usually concave, with the roots of the hairs protruding. In cattle and goats the older term cutaneous streptothricosis is sometimes still used. In sheep the condition is referred to as “lumpy wool” or “mycotic dermatitis” when wooled areas are affected and as “strawberry foot rot” when distal extremities are involved.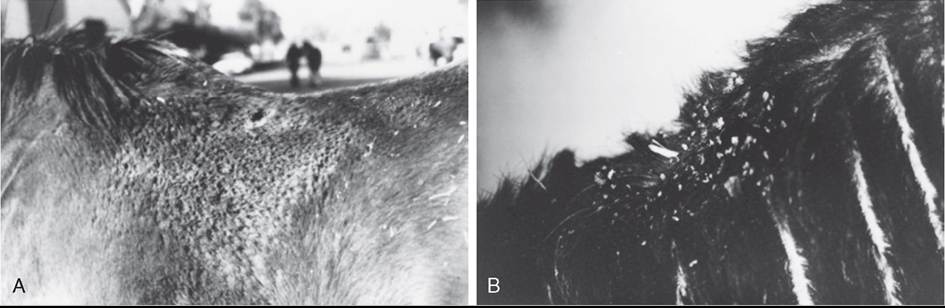
FIG. 40.7 Dermatophilosis (Dermatopbilus congolensis). A, Horse with suppurative crusts and matted hair on the back. B, Scaling and crusting over withers and neck of a bovine.
Body areas predisposed to infection include those that are most susceptible to maceration and trauma. The distal extremities, muzzle, and entire length of the dorsum are frequently the initial sites of infection. Nonpigmented skin is also reported to be more susceptible to infection. Horses develop lesions in areas rubbed by tack, and cattle often have involvement of the udder and scrotum. Goat kids may have a tendency to develop lesions on the pinnae and under the surface of the tail. Sheep may develop a form of dermatophilosis that begins as an encrusted proliferative dermatitis at the coronet region; removal of the external crusts reveals a pink-red granulation bed that resembles the surface of a strawberry. Lesions can extend from the hoof to the hock; with loss of the crusts, ulceration occurs. Under appropriate conditions, dermatophilosis can become generalized.
■ Diagnosis Diagnosis is made by demonstrating the “railroad-track” cocci on impression smears. A portion of one of the crusts should be minced and mixed with a few drops of sterile water on a glass slide, Gram stained, and examined microscopically.
Alternatively, bacterial culture or histopathology may be used for diagnosis, particularly in chronic cases. A thick crust composed of alternating layers of parakeratotic stratum corneum, dried serum, and degenerating neutrophils is the most characteristic change. A superficial folliculitis may be a prominent feature of the disease.1 In Gram-stained sections, the branching filamentous organisms can be observed in the crusts and follicles. A recent report showed the efficacy of using real-time quantitative polymerase chain reaction (RT-qPCR) in the diagnosis of this organism.5■ Therapy The animal should be removed from the wet environment if possible. Careful removal of possibly painful crusts, washing with iodophors or lime sulfur, and administration of antibiotics (for horses, 22,000 units/kg procaine penicillin G IM twice daily or 30 mg/kg trimethoprim-sulfamethoxizole PO twice daily) for 7 to 10 days.4 Long-acting oxytetracycline given as a single 20-mg/kg IM dose has been reported to be effective for bovine and ovine dermatophilosis. The crusts are important in contagion, so they should be disposed of rather than brushed to the ground. Reduced tick control has been associated with increased incidence of the disease.6
Folliculitis, Furunculosis, and Impetigo
■ Definition and Etiology Bacterial folliculitis (superficial pyoderma) is defined as inflammation of the hair follicles secondary to a bacterial infection. Furunculosis is the term used to describe a follicular infection that breaks through the follicular wall (“boil”). Bacterial infection that causes subcorneal pustules but does not involve hair follicles is called impetigo. Folliculitis and furunculosis are often seen in horses1,4 and goats3 but are an uncommon problem in cattle and sheep. Impetigo is relatively common in cattle and goats.
Bacterial folliculitis is usually caused by a coagulase-positive Staphylococcus species.
Both Staphylococcus aureus and Staphylococcus pseudintermedius (formerly S. intermedius) have been isolated.7,8 In one study in horses, S. aureus accounted for twice as many isolates as S. pseudintermedius; the same study isolated some strains of Staphylococcus hyicus as well.9 Staphylococcus delphini has also been isolated from horses on occasion. Many isolates are resistant to penicillin G.9 Occurrence of pyoderma has been linked to poor nutrition and husbandry in some cases.10■ Clinical Signs Clinical signs of staphylococcal pyoderma are most often crusts, usually in a circular pattern suggestive of dermatophytosis (this may be why equine pyoderma is underdiagnosed), epidermal collarettes (circular skin lesions with an exfoliative border, as seen in dogs with superficial pyoderma), or encrusted papules similar to the miliary dermatitis reaction pattern in cats.7 These infections tend to vary in intensity of pruritus. Histology often shows folliculitis and furunculosis, but bacterial colonies are not always seen. A truncal form of bacterial folliculitis (contagious acne, contagious pustular dermatitis, Canadian horsepox) is often associated with poor grooming and trauma from tack and saddle; warm, wet weather; and heavy work. It is painful and interferes with working and riding. It is usually caused by a coagulase-positive Staphylococcus species but may also be due to Corynebacterium pseudotuberculosis11 (more often a cause of deep pyoderma, as discussed later). In horses, folliculitis often develops in the saddle and lumbar region, particularly in the summer. The affected area may initially be swollen and sensitive, followed by formation of follicular papules and pustules. These may become confluent or rupture, forming plaques and crusts. Deep pyoderma followed by ulceration may develop over large areas of the body, especially the neck, sides of the thorax, inner surface of the thighs, and prepuce.
A pastern bacterial infection (pastern folliculitis) is often seen. Again, the causative agent is usually a coagulase-positive Staphylococcus species. As with most primary pyodermas, the mechanism by which the organism gains its foothold is unknown; it is not necessarily contagion or poor sanitary conditions. The lesions are usually limited to the posterior aspect of the pastern and fetlock regions; one or more limbs may be involved. Initial lesions consist of papules and pustules. If left untreated, they coalesce and may produce large areas of ulceration and suppuration that may be quite painful. The disease is usually not associated with systemic signs, and the general health of the horse is not affected.
A relatively uncommon nodular disease termed botryomycosis mimics actinomycosis or a deep fungal infection but is most often caused by Staphylococcus spp. in the horse. These may require surgical excision as well as long-term antibiotics.
■ Public Health Considerations In a 2000 study, methicillin-resistant coagulase-negative staphylococcal species were cultured from healthy horses in Japan. The authors concluded, “These organisms must be considered a potential threat to horses and veterinarians who care for them.”12 In a 2006 study from the Netherlands, methicillin-resistant coagulase-negative staphylococci were found frequently.13 The organism was usually Staphylococcus sciuri rather than Staphylococcus epidermidis, which was found in the humans in close contact with these horses. No methicillin-resistant S. aureus (MRSA) was found in healthy horses. A more recent article reported S. sciuri from a horse's skin infection.14
There is little public health concern about methicillin- resistant S. pseudintermedius (MRSP) or S. delphini because clustering of equine cases does not appear to be important, and zoonotic disease potential seems to be limited.
In contrast, a single strain of MRSA was isolated from both humans (13%) and horses (4.7%) on horse farms in Canada and New York state.15 In looking at horses admitted to a university teaching hospital (Ontario Veterinary College), MRSA was isolated from 120 (5.3%) of 2283 horses.
Of these 120 horses, 50.8% were positive at admission, and clinical infections due to MRSA were present or developed in 14 animals. Horses colonized at admission were more likely to develop clinical MRSA infection. Administration of ceftiofur or aminoglycosides during hospitalization was the only risk factor associated with nosocomial MRSA colonization. Another strain of MRSA was isolated from a small number of horses at the Veterinary University in Vienna, Austria.16 Of further concern is the finding of nasal carriage of S. aureus in cattle.17 Of most concern is the finding of humans reporting skin lesions after contact with a community MRSA-positive affected foal, despite short-term contact with standard protective barriers. Isolates from the foal were indistinguishable from those affecting humans.18 In another study, MRSA was isolated from 15.6% of veterinarians or technicians in large animal practice, as opposed to from only 4.4% of small animal personnel; large animal practice was the only statistically significant variable associated with colonization of MRSA.19 On two horse farms with endemic MRSA, active screening and strict implementation of infection control protocols resulted in a rapid decrease in the number of colonized horses. Most horses eliminated MRSA without antimicrobial treatment.20■ Therapy The antibiotic usually used for bacterial skin infections in the horse is oral trimethoprim-sulfamethoxazole (TMS [30 mg/kg PO q12h for 2 to 6 weeks, longer for deep infections]).7 Interestingly, dosing intervals for intravenous (IV) administration of TMS in horses may not be appropriate for use in donkeys or mules. Donkeys eliminate the drugs rapidly compared with horses.21 In cases of staphylococcal resistance to TMS, enrofloxacin or doxycycline may be used. Doxycycline is less expensive but associated with a higher incidence of colic. Dosage is usually 10 mg/kg PO q12h. Off-label use of oral enrofloxacin formulations for poultry, ruminants, or swine has been suggested. The formulation for poultry may be used; the dose is 7.5 mg/kg PO once daily. Use of enrofloxacin in young horses (it is called “pigeon fever” in the United States. This type of deep Cory- nebacterium infection may occur where caseous lymphadenitis is common in sheep or goats (although proximity to small ruminants is not a requirement), and it also may be seen seasonally when insect populations and activity are maximal. This may occur in the dry seasons, giving rise to another vernacular name, “dry land distemper”, when the process affects the inguinal region. Insect vectors seem probable, especially stable, horn, and house flies.34 The frequency of this disease is increasing in the United States.35 Draining nodules or abscesses are especially common in the pectoral region and occasionally affect the face, neck (Color Plate 40.6), axilla, groin, and limbs; they begin deep and enlarge, often with much edema, and rupture in 1 to 4 weeks, discharging viscid creamy pus, a major source of contamination. Abscesses most often rupture externally. Diagnosis is by clinical signs, with the infection readily identified by bacterial culture of aspirate samples from abscesses. The synergistic hemolysis inhibition test is useful for diagnosis of internal abscesses but unreliable for external abscesses.36 Recent molecular studies of various strains of C. pseudotuberculosis have not shown definitive relationship between an individual strain and the location of the abscess.3',38
Treatment depends on location. If the abscess is in the axilla and thus painful on movement or prevents locomotion, establishing drainage is important, and antibiotics are indicated.
The antibiotics most commonly used are ceftiofur (2 to 4 mg/kg IM q12-24h), enrofloxacin (7.5 mg/kg PO or IV q24h), procaine penicillin (2θ,θθθ to 50,000 lU/kg/day), rifampin (3 to 5 mg/kg PO q12h), and TMS (30 mg/kg PO q12h).36,39 Interestingly, there have been no changes in the minimum inhibitory concentrations of effective antibiotics over time.40 Treating with TMS and rifampin concurrently can lead to a greater incidence of colitis and is to be avoided. If the decision is made to use antibiotics but drainage cannot be easily established (e.g., axillary abscess, with owner unwilling to allow veterinarian to use trocar and drain), antibiotics must be used for a minimum of 1 month. If the abscess is solitary and not causing pain or fever, antibiotics are usually unnecessary, but bringing the abscess to a head with hot packs or heat-inducing agents (ichthammol) is important. Once an abscess has drained, gentle cleaning with tamed iodines or chlorhexidine is indicated.
Early diagnosis and long-term antimicrobial treatment are important for a successful outcome in horses with internal C. pseudotuberculosis infection. Ultrasonographic imaging is an important technique for identifying specific organs affected, aiding in obtaining samples for a definitive diagnosis, and monitoring response to treatment. Pregnant mares with internal infections are at risk for fetal loss. Preexisting chronic organ disease may be associated with a poor prognosis.41
Digital Dermatitis (Papillomatous Digital Dermatitis, Bovine Digital Dermatitis, Foot Warts, Heel Warts, Hairy Foot Warts, Hairy Heel Warts, Mortellaro's Disease, Strawberry Heel Warts, Verrucous Dermatitis)
John A. Angelos • Muhammad Muzafar Makhdoomi
Digital dermatitis (DD) of cattle is an infectious, contagious, painful dermatitis of the digital skin and is a major cause of lameness in dairy cattle. Economic losses in affected animals are attributable to decreased milk production and reproductive performance, increased costs for treatment and management, and increased culling rates.1-4 Primarily a disease of housed dairy cattle, DD was first described in Italy in the mid-1970s5; however, since the mid-1990s this condition has increased in prevalence throughout the world. It has been reported in many countries, including several in Europe, the United States, Japan, Chile, Canada, Mexico, and New Zealand.6-9 Digital dermatitis has also been found in feedlots and pasture-based dairies. Although it is difficult to assign costs to specific diseases, DD is thought to be of lower cost than sole ulcers or foot rot; however, prevalence of DD can be much higher than that of other lesions, so the total cost can be high.
■ Clinical Signs Roughly 80% of DD lesions occur on the plantar aspect of the hind foot, immediately proximal to the heel bulbs and adjacent to or extending into the interdigital space.8 A 2017 study of dairy cattle in New Zealand reported that approximately 75% of affected cows were infected on one rear limb and 25% were infected on both rear limbs.10 Less commonly, lesions occur on the plantar aspect of a forefoot and the dorsal aspect of any foot.8 Lesions are confined to the digital skin below the level of the dewclaws.8
The gross appearance of lesions and the predilection for hind limbs and skin-hoof wall junctions, especially those bordering the heel bulbs and interdigital space, distinguish this disease from other causes of bovine dermatitis. The clinical appearance of DD has been classified into five stages, advancing from acute to chronic and in some cases to regression and healing.11 The first stage describes small (~1 to 2 cm) focal lesions with a reddened circumscribed area (hence the name “strawberry heel warts”) that are extremely painful and have hairs on the periphery of each lesion that are erect and matted in exudate. The second stage has larger (2 to 6 cm) ulcerated lesions with peripheral hairs that are two to three times longer than surrounding hairs. In the third stage healing lesions have a rough, encrusted surface and are often gray in color. The fourth stage (often referred to as the “hairy” or “papillomatous” stage) consists of chronic proliferative lesions with varying degrees of hyperkeratosis characterized by black papilliform projections that vary in length from 1 mm to 3 cm. If the fifth stage is reached, it is characterized by healing of the lesion.11 Washed surfaces are characteristically extremely painful and either red and granular, or they may appear as white-yellow, gray, brown, or black papillary areas with red, granular areas interspersed. Lesions bleed easily if traumatized. The time required for lesions to progress to a mature (“hairy” or papillomatous) state varies. DD lesions involving the interdigital space often occur in association with a previous interdigital fibroma. Lesions may have a foul odor12,13 attributed to secondary anaerobic bacterial growth in exudate material (most likely Fusobacterium necrophorum and/or Porphyromonas levit).114 Swelling of the pastern and fetlock regions is not typical in uncomplicated cases. Lameness is characteristic on dairies where DD has a high prevalence, but lameness is not consistently related to lesion size or chronicity. As such, animals can appear much lamer than one might expect given the size of the lesion. If affected digits go untreated, those with plantar or palmar lesions may become clubbed when a cow preferentially bears weight on toes while the heels overgrow.
■ Differential Diagnoses Differential diagnoses for an individual case of DD include interdigital necrobacillosis (foot rot; foul in the foot; interdigital phlegmon), interdigital hyperplasia (corns; interdigital fibroma), interdigital dermatitis, and traumatic injury with granulation tissue. For herd problems of lameness localized to the digit, differentials should include DD, interdigital necrobacillosis, interdigital dermatitis, laminitis, excessive sole wear from caustic or abrasive flooring, and improper or no hoof trimming. If signs of polysystemic disease exist, coronitis from viral diseases (e.g., bovine virus diarrhea, vesicular stomatitis, foot-and-mouth disease) should be considered.
■ Epidemiology Digital dermatitis typically spreads rapidly among adult cows, often affecting a majority of adult animals within a year after introduction. Once established in a herd, lameness is more typically seen in first and second lactation cows, commonly after entry into a milking string.15-17 Lesions are typically seen in older cows; however, lameness in older animals is less common compared to younger cows. Bulls and yearling heifers can be affected, but these groups generally comprise a small proportion of clinical cases. Freestall herds tend to be more commonly affected than stanchion (tie stall) housed cattle or pastured cattle. DD is almost exclusively seen in dairy cattle, with no breed predilection. In endemic herds it is unlikely that eradication is possible.
Retrospective epidemiologic studies in the United States identified two significant risk factors in high-prevalence herds: muddy or wet conditions and purchasing replacements from off premises.3,16 Experimental transmission of DD was demonstrated when homogenates of DD lesions were applied to the feet of calves subjected to moisture and low oxygen tension.18 Conditions of moisture and low oxygen tension are present on confinement dairies if manure management and hygiene are inadequate. Other risk factors include use of outside hoof trimmers and not washing hoof-trimming equipment between cows.3
■ Pathogenesis A variety of anaerobic organisms have been associated with DD.6,19-25 Treponema spp. spirochetes have been identified most consistently and form the majority of the colonizing bacterial flora on active lesions; these organisms also can invade the epidermis and dermis.23,25-29 These spirochetes induce a humoral antibody response in cattle with active lesions.30 Although DD lesions can exhibit gross and histologic similarities to viral papillomas, bovine papilloma virus has not
2 8 31
been found in lesions.,8,
Evidence suggests that DD is a multifactorial disease involving environment, microbial, host, and management factors.3,8,15-17,25 Rough flooring; inadequate drainage; fecal and urine accumulation on floors; dirty, wet, or uncomfortable bedding areas; and overcrowding can adversely affect digital skin health and increase the risk of DD. Transmission among cattle and between herds may be facilitated by contact between clinically and subclinically affected cows, fomites such as foot-trimming instruments, and livestock trailers and farm equipment.
Chronic and recurrent cases in otherwise healthy adult cattle are reported; immunity to DD, if it does develop, may be incomplete or temporary. Recurrence is common in individual cows following antimicrobial treatment.11,32 Spontaneous regression of lesions and resolution of lameness, while possible, occurs rarely.
■ Pathologic Findings Histopathologic criteria to establish a diagnosis of DD are8:
• Circumscribed plaque of eroded acanthotic epidermis attended by parakeratotic papillomatous proliferation profusely colonized by spirochete-dominant bacterial flora
• Loss of stratum granulosum
• Invasion of stratum spinosum by spirochetes
• Infiltration of neutrophils, plasma cells, lymphocytes, and eosinophils into the dermis.
If performed, biopsies should be full-thickness 4- or 6-mm punch biopsies, washed off with sterile saline and placed in buffered formalin. Although helpful in confirming a diagnosis, histopathology is not necessary to make a diagnosis because DD lesions typically exhibit a characteristic appearance and occur in specific locations in cattle.
A biopsy study on treatment and recurrence of DD showed that clinical and histopathologic diagnoses were in agreement for active lesions before treatment.32 Histopathology on day 28 post treatment with lincomycin or oxytetracycline, however, demonstrated that more than half of the lesions that appeared clinically resolved still had microscopic evidence of infection.32
■ Treatment and Prevention The most common methods for treating DD involve application of topical antibiotics.8,11,32,33 There are no antibiotics currently labeled for treatment of DD in the United States; therefore adherence to extralabel drug-use regulations and observance of scientifically established withdrawal times is imperative when risk of drug residues exists.
The most commonly used therapy for DD is topical oxytetracycline or lincomycin applied in spray or powder form. To apply it topically as a spray, oxytetracycline or lincomycin is mixed with deionized or distilled water in a 2- to 4-L agricultural sprayer (25 g/L oxytetracycline, 8 g/L lincomycin) and applied directly to the heels of DD-affected cattle daily for 5 to 14 days. For topical powder treatment, 2 grams of oxytetracycline or lincomycin powder are placed on a cotton pad, applied to the affected area with an elastic bandage, and changed daily for 5 to 10 days. Both treatments elicit a rapid response consisting of dramatic lameness regression and reduction in wound size. The recurrence rate is high enough that topical treatments may need to be repeated after 45 to 60 days for more effective control. There have been no reported antibiotic residue violations resulting from topical application of antibiotics.34 Parenteral penicillin and ceftiofur have been reported to be efficacious8 but may require milk withholding. Given the current restrictions on extralabel use of ceftiofur in the United States, practitioners should be mindful of following all label directions related to dose, route, frequency, and duration of therapy.
Footbaths containing a variety of products, including 5% formalin, oxytetracycline (1 to 4 g/L), lincomycin (1 to 4 g/L), copper sulfate (0.25 to 1 g/L), zinc sulfate (20%), or sodium 1231 35 38
hydroxide,’’ can assist in controlling the disease in infected herds; however, low-prevalence herds (Prevalence is most common on dairies with intensive stocking rates and moist, filthy conditions. In tied systems the hind digits are more commonly affected. In freestall systems lesions are observed equally between the front and hind digits. Diffuse epidermal erosion in the interdigital cleft may be seen in early cases. More chronic cases exhibit hyperkeratosis leading to a roughened appearance to interdigital skin and dorsal and palmar commissural skin folds. Chronic cases are frequently accompanied by cracks in the heel (heel horn erosion, “slurry foot,” “slurry heel”), with potential underrunning of the heel horn and subsequent severe lameness.
Some investigators have hypothesized that ID and DD are forms of the same disease complex. Dichelobacter nodosus may be a primary or contributory pathogen36 along with Treponema spp.45 ID and DD share certain histologic characteristics suggesting contribution or involvement by spirochetes (Treponema), and both can be successfully treated and prevented with the same topical antibiotics or footbaths. However, ID can persist on dairies that practice regular foot-bathing. Slatted, rather than solid, floor systems may reduce incidence of the condition. Causative organisms may survive within deep heel cracks, which should be trimmed to reduce accumulation of debris and allow exposure to foot bath solutions.
ID differs from interdigital necrobacillosis (foot rot), in which infection extends into the dermis, leading to fissure formation, infection of deeper structures if left untreated, and cellulitis of the pastern and fetlock regions.
In sheep, ID and virulent foot rot (VFR) are considered two different stages of the same disease complex,46,47 with ID classified as a less severe form.48 The same disease state is also classified as benign foot rot in Australia. Some authors designate the more severe form of disease as VFR in sheep, whereas others classify it simply as foot rot. In the UK, ID and VFR are the main causes of lameness in sheep49 and major animal welfare issues.50 The primary pathogen is D. nodosus, a gramnegative, rod-shaped anaerobic bacterium.51-53 In sheep, ID is characterized by inflammation of the interdigital skin, resulting in lameness and loss of body condition.54 In ID the interdigital skin appears pink and moist and is sensitive to touch, whereas VFR is characterized by underrunning of the hoof horn leading to separation of the hoof from the underlying soft tissue. The underrunning of the hoof horn begins at the junction of the skin fold with the heel that spreads anteriorly to the abaxial wall. This causes separation of the hoof horn from the laminae of the foot.55 It is often accompanied by discharge of a grayish exudate that has a characteristic fetid odor.51 Some authors have suggested a role of the host's acute inflammatory response to D. nodosus infection in leading to the development of clinical signs.56
The occurrence of ID is influenced by local climatic conditions.57 In Australia a mean daily temperature greater than 10° C and a wet pasture are required for transmission of the disease. In the UK the disease can occur throughout the year and can be transmitted between sheep even when daily mean temperatures are greater than 10° C.58 A study reported mini epidemics of ID during the spring in the UK, with increasing temperature and rainfall favoring spread of disease.59,60
In the UK, ID in sheep is treated with topical oxytetracycline spray (25 mg/mL) on the interdigital skin for 3 days. The use of topical antibiotic spray is highly effective at combating the disease61,62 and leads to more than 95% recovery within 3 to 4 days.61,63 Foot-bathing has also been used, but topical therapy is generally considered a more effective method of ID control. VFR can be difficult to treat with antibiotics, and recurrent cases of VFR can occur after 2 weeks of antibiotic treatment. VFR can be effectively controlled and eliminated from sheep flocks by vaccination with a D. nodosus serogroup-specific vaccine.64
Control and elimination programs for ID and VFR in the United Kingdom are based on empirical evidence that D. nodosus cannot survive off the host for more than 7 days.51 Survival off the host (pasture) is dependent on moist conditions, and some authors have reported that D. nodosus does not survive on pasture for more than 2 weeks under warm and damp conditions. Therefore, under these conditions, sheep are not at risk of ID and VFR once pastures have been rested for 14 days. However, a recent study using qPCR reported that viable D. nodosus can survive for at least 40 days in soil microcosms, and the rate of survival is affected by soil type, moisture, and temperature, with lower temperatures (41°F) and clay soil favoring survival of higher loads of D. nodosus.65 This is a step change in our understanding of the ability of D. nodosus to survive off a host. Aggressive treatment of infected sheep and preventing access of healthy sheep to D. nodosus- contaminated pastures for at least 40 days can potentially aid in controlling ID.
More on the topic Bacterial Diseases:
- Bacterial Diseases
- Interdigital Necrobacillosis (Foot Rot) in Cattle
- Smith Mary C., Sherman David M.. Goat Medicine. 3rd edition. — Wiley-Blackwell,2023. — 976 p., 2023
- Peripheral Vestibular Disease of Horses
- Pregnancy Loss
- ANATOMY AND PHYSIOLOGY
- EPIDEMIOLOGY
- Smith Bradford P., Van Metre David C., Pusterla Nicola (eds.). Large Animal Internal Medicine. Part 2. 6th edition. — Elsevier,2020. — 2279 p., 2020
- THERAPEUTICS
- Surveillance