Idiopathic Renal Hematuria
Harold C. Schott II • Alexandra J. Burton
Idiopathic renal hematuria (IRH) is a syndrome characterized by sudden onset of gross, often life-threatening hematuria.1 Hemorrhage arises from one or both kidneys and is manifested by passage of large blood clots in urine.
Endoscopic examination of the urethra and bladder usually reveals no abnormalities of these structures, but blood clots may be seen exiting one or both ureteral orifices. Although a definitive cause of renal hemorrhage may be established in some horses (e.g., renal adenocarcinoma, arteriovenous or arterioureteral fistula, renal pseudoaneurysm), the disorder is termed idiopathic when a primary disease process cannot be found.2-5 Both genders, a wide age range, and several breeds of horses (including donkeys and a mule) have been affected. However, more than 50% of animals with IRH have been Arabians.Use of the term idiopathic renal hematuria to describe this syndrome of horses was adopted from its use in human patients and dogs with severe renal hemorrhage.6-10 Benign essential hematuria and benign primary hematuria are other terms that have been used to describe less severe hematuria that is not associated with trauma or other obvious causes of hematuria.6-10 In humans and dogs, hematuria is more often a unilateral than a bilateral problem, similar to what has been observed in the few affected horses. The pathophysiology remains poorly understood, but macroscopic hematuria has been associated with immune-mediated glomerular damage (e.g., acute postinfectious
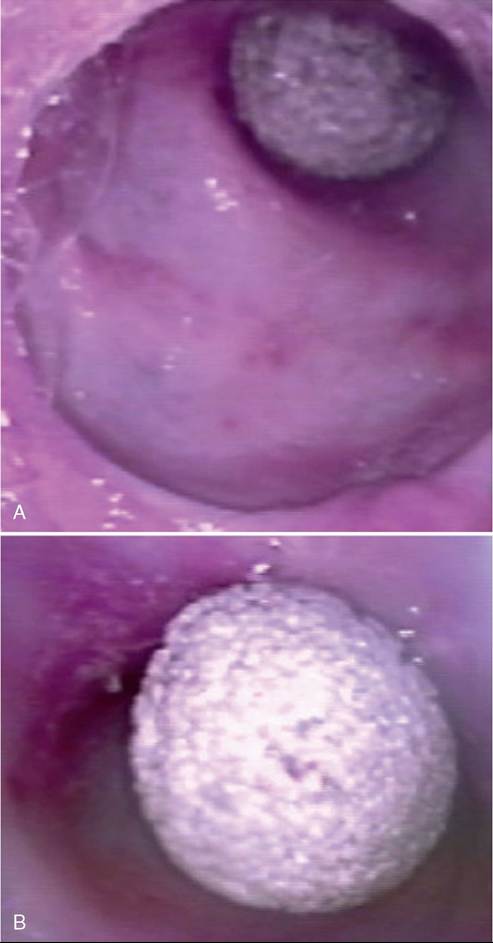
FIG. 34.12 A, Urethroscopic image of a calculus causing intermittent hematuria and stranguria in a 12-year-old gelding. The spiculated calculus caused severe mucosal irritation and damage.
B, Urethroscopic image of an impacted stone in a 15-year-old gelding with intermittent colic and hematuria.glomerulonephritis [GN], membranoproliferative GN, IgA nephropathy, or Berger disease), thin basement membrane nephropathy, and the loin pain-hematuria syndrome in human patients. One of the authors (AJB) has seen a case of IRH in a donkey in conjunction with simultaneous onset of severe laminitis. The donkey recovered over the course of 6 weeks with extensive supportive care.
Hematuria and pigmenturia can accompany several systemic diseases in horses.11 However, patients affected with IRH appear to have spontaneous severe hematuria, in the absence of any other signs of disease. Although one report suggested that severe renal hemorrhage was caused by pyelonephritis, supportive data were lacking.12 In cases managed by the author (HCS), neither UTI nor urolithiasis were detected, and the magnitude of hematuria often resulted in the need for repeated blood transfusions. As with hemorrhage associated with guttural pouch mycosis, the syndrome may produce episodic hemorrhage. Initially, hemorrhage is noted by finding a large amount of clotted blood in stall bedding or in the pasture. However, other client complaints (e.g., depression, anorexia, weight loss) are typically absent. Examination may reveal dried blood at the end of the penis or in the sheath of males or on the vulvar lips and between the hindlimbs of mares. In both genders, neoplasia of the external genitalia or urinary tract is an important differential diagnosis, and in mares, varicosities in the area of the vestibulovaginal sphincter also must be considered, especially in multiparous mares. When blood is not detected in the sheath or vulvar areas, further evaluation may be unrewarding because the renal bleeding may cease spontaneously. In the absence of positive urine culture results, bleeding has anecdotally been attributed to cystitis and pyelonephritis, because hemorrhage stops during a course of antimicrobial therapy.
More likely, spontaneous resolution has occurred. The magnitude of hematuria is considerably greater with IRH than most UTIs, pyuria is absent, and urine culture results are negative. In the author's (HCS) experience, one or two initial episodes of hemorrhage are followed by a more severe hemorrhagic crisis within months to 2 years after observation of the initial bleeding episode. Signs of colic have been notably absent in the history of affected horses.Diagnosis
A diagnosis of IRH is made by exclusion of systemic disease, other causes of hematuria, and alterations in hemostasis. Physical examination may reveal tachycardia, tachypnea, and pale membranes, consistent with acute blood loss. Rectal palpation may reveal an enlarged, irregular bladder resulting from the presence of blood clots. Azotemia is uncommon. Endoscopic examination is important to document that hematuria is originating from the upper urinary tract and to determine whether hemorrhage is unilateral or bilateral (Fig. 34.13). Repeated examinations may be required to answer the latter question. Ultrasonographic imaging is necessary to rule out nephrolithiasis or ureterolithiasis and may occasionally reveal
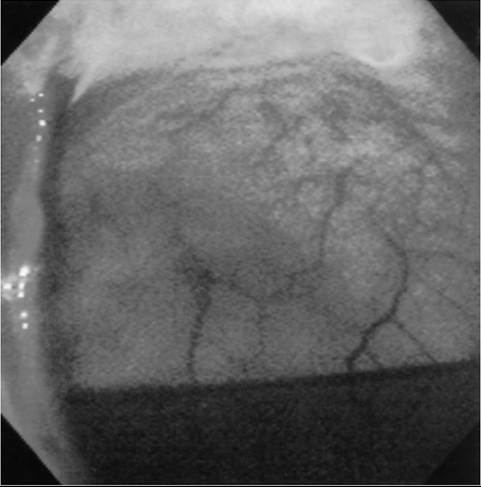
FIG. 34.13 Cystoscopic image of a 19-year-old Arabian mare with idiopathic renal hematuria. A large blood clot can be seen exiting the left ureter, whereas the right ureteral opening appears normal.
a distended vascular space or renal vascular anomaly as the cause of hematuria. Renal scintigraphy can be a useful technique in affected horses, providing semiquantitative information about renal function when a nephrectomy is being considered. Renal biopsy and immunofluorescence (IF) staining may assist in documenting immune-mediated glomerular injury, but the significance of such results is not well understood at this time.
Treatment
Treatment for IRH consists of supportive care for acute blood loss, including blood transfusions. Medications intended to promote hemostasis (e.g., α-aminocaproic acid, formalin) have also been administered, but their efficacy has not been validated. Because the condition may be self-limiting in some patients, supportive care is warranted. With severe and recurrent hematuria of unilateral renal origin, a nephrectomy may be indicated, but owners should be warned of the risk of hematuria developing in the contralateral kidney. In the author's (HCS) experience, risk of contralateral renal bleeding appears to be greater in the Arabian breed. Recently, topical sclerotherapy of the renal pelvis using 5% povidone iodine ± silver nitrate via ureteral stents has been reported as a treatment for IRH in dogs.13,14 This therapy shows some promise, as it was successful in the short term, but longer-term follow-up and a larger case cohort are needed to fully evaluate this technique.13,14