Ocular Trauma
Kristina R. Vygantas
Causes of Trauma
Because the eye is anatomically prominent in horses and food animals, it is prone to blunt and sharp trauma, which can range in severity from a mild abrasion caused by a conjunctival foreign body to a severe corneal laceration with globe rupture and orbital bone fracture.
Ocular injuries may result from a variety of causes, including foreign materials such as soil, sand, or stones, which may be thrown into the eye during running or by the wind; trauma from disciplinary action; scratches by vegetable matter such as hay, weed stems, tree limbs, or thorns; exposure to chemical irritants; and sudden, violent head movements during training, working, or grooming. Other sources of ocular injury include stanchions, stall or trailer latches, hooks, protruding nails, bucket handles, fencing materials, and other animals, particularly horned ruminants.Recumbent neonates and animals with CNS disease or severe illnesses that cause depressed mentation often suffer eye injuries from abrasion by debris or bedding materials, such as sand, straw, hay, or wood shavings. These injuries may be prevented by protecting the eye from trauma through the use of a padded hood or soft mats under the head or through sedation to prevent thrashing. It is also important to keep the cornea well lubricated in dehydrated animals and/or those with reduced blinking frequency. Following ocular trauma, opportunistic or pathogenic organisms may become established in the wound bed and may cause superficial or deep corneal infections. Ocular flora native to the conjunctiva include potential pathogens that may cause severe infections.1
Ocular Examination in Cases of Head Trauma
The goals of examination are to determine the degree of ocular trauma and to offer a prognosis for recovery of vision and preservation of the eye.
The history should elicit information as to the cause and duration of the injury, previous ocular and systemic disease or therapy, and a description of any recent sedation, anesthesia, or therapy.Blunt or sharp facial trauma frequently results in damage to the orbit and globe, including fractures or soft tissue injuries of the orbit, corneal abrasions and edema, corneal or scleral rupture, hyphema, traumatic uveitis, lens luxation, traumatic cataract, vitreal hemorrhage, retinal tear or detachment, or proptosis. Therefore the integrity of the orbit and globe and presence of vision should be determined when evaluating a patient with facial trauma.
Ophthalmic examination can be performed only after adequate restraint of the head (see the Ophthalmic Examination Procedures, Restraint section earlier). Intravenous (IV) sedation, sensory and motor nerve blocks, topical anesthesia, and the use of a halter, twitch (in horses), or nose tongs (in cattle) often are necessary for adequate examination of the traumatized eye.
Trauma to the Orbit as well as oblique projections. CT and MRI are available at many referral centers. Detail of the bony and soft tissue structures is greatly enhanced by the cross-sectional views acquired by CT, as are the structures of the calvarium, sinuses, and teeth. MRI is also beneficial in delineating soft tissue abnormalities within the orbit and sinuses.4-6 In a recent case report on a periorbital wooden foreign body in a horse, MRI was required to identify the embedded material.6
Immediate evaluation for orbital fractures should include careful examination of the globe. In cases with substantial swelling, ice packs applied to the fracture site may reduce swelling. Systemic antiinflammatory therapy (e.g., flunixin meglumine, ketoprofen, phenylbutazone) may also be given. Systemic antibiotics should be used if sinus involvement is suspected. If the fracture fragments are only minimally displaced, surgical intervention may not be required.
Surgical repair should be considered if fragment displacement or entrapment of extraocular muscles has occurred or could occur.3,7 Trauma sufficient to cause fractures may also result in neurologic dysfunction and immobility of the eyelids.If eyelid movement is impaired, the globe must be adequately protected and lubricated until neurologic function returns. If the globe is only minimally exposed, a sterile ophthalmic lubricant may be used at least three or four times daily. In more severe cases, a nictitating membrane flap or temporary partial tarsorrhaphy may be required. If neurologic dysfunction is permanent and results in significant exposure conjunctivitis or keratitis, partial or complete permanent tarsorrhaphy should be performed.3 Enucleation with or without placement of an orbital prosthesis may be required for severely affected eyes.
Rupture of the sclera and/or cornea is another potential consequence of blunt trauma to the orbit and globe. A recent study found that eyelid and conjunctival swelling are the most consistent clinical signs of scleral rupture in horses.8 Other clinical features of this condition are hyphema, subconjunctival hemorrhage, uveal prolapse, and a collapsed anterior chamber (Color Plate 39.15). Ultrasonographic findings include poorly defined scleral margins and echoic or hyperechoic material in the anterior and posterior chambers and in the vitreous.7 Trauma severe enough to cause corneal or scleral rupture is typically associated with significant intraocular damage such as retinal detachment, uveal avulsion and prolapse, and expulsive hemorrhage. Prognosis for vision and globe salvage is usually poor.
Traumatic puncture wounds of the eyelids and conjunctiva may result in orbital cellulitis and exophthalmos in food animals and horses. Pyrexia and leukocytosis may be present. If a retrobulbar abscess occurs, temporomandibular movement causes extreme pain; the animal may have the eyes partially closed, be off feed, and stand with the neck extended.
The client may observe a relatively sudden onset of exophthalmos, eyelid swelling, severe chemosis, and exposure keratitis.3,9 With time, the cellulitis may organize into a discrete abscess that can be located by palpation or ultrasound. Fine-needle aspiration may be performed to obtain specimens for culture and susceptibility (C&S) and cytology to guide antimicrobial therapy. Therapy should consist of systemic and topical antibiotics and a systemic antiinflammatory medication. Ophthalmic ointments and lubricants should be used on the exposed cornea and conjunctiva to prevent desiccation. In many cases, the wound or abscess should be debrided or drained to facilitate healing, especially if a well-organized abscess is present.Although traumatic proptosis is uncommon, it may occur in horses and food animals. The prognosis for return of vision is guarded to poor, depending on the extent of damage to the optic nerve and retina. If the globe is ruptured and/or the extraocular muscles are avulsed, the eye should be enucleated. If the extent of the damage cannot be evaluated initially, the globe should be repositioned, a temporary tarsorrhaphy performed, and the globe reevaluated after 7 to 10 days of therapy. Treatment should include topical broad-spectrum antibiotics, topical atropine, and systemic antiinflammatories and antibiotics. With severe fractures or serious ocular damage, consultation with or referral to an appropriate specialist is advised.
Trauma to the Eyelid
Eyelid trauma is frequently accompanied by injuries to other ocular structures. Careful ocular examination should be part of the evaluation of animals with eyelid trauma. Injuries may range from swelling (blepharedema) or orbital cellulitis to extensive lacerations and avulsion. Blepharedema may be accompanied by hemorrhage and usually resolves quickly without therapy; however, recovery may be hastened by the use of ice packs and systemically administered ketoprofen or flunixin meglumine.
Horses are particularly prone to eyelid lacerations because of the prominence of the eye and their tendency toward sudden head movements when startled. Lacerations may be categorized into those without eyelid margin involvement, those with eyelid margin involvement, and avulsions of part or all of an eyelid. For all types of eyelid injury, several basic principles should be followed. Lacerations should be treated promptly to avoid distortion from excessive swelling, infection, scarring, and loss of function. Lacerated or displaced tissue should not be excised. It is impossible to replace the mucocutaneous junction of the eyelid margin. If eyelid margin is sacrificed, the risk of scar formation and secondary corneal damage is high. The laceration should be thoroughly and carefully flushed with sterile saline and explored to remove all foreign material. In acute trauma, cold compresses may assist in decreasing swelling. When suturing an eyelid laceration, it is essential to preserve the eyelid margin; therefore eyelid lacerations should be repaired with minimal debridement. The vascular nature of the eyelid allows for minimal debridement even if the tissue is severely damaged. In cases of avulsion of part or all of the eyelid, a variety of blepharoplastic procedures may be performed to help restore functional eyelid margin.10-12 For a more detailed description of the principles of surgical repair of the eyelids, an ophthalmic surgical textbook is recommended.10,11
Postoperative care of all eyelid lacerations should include standard wound hygiene, application of fly repellent and topical ophthalmic antibiotics, and prevention of self-trauma. In contaminated wounds, systemic antibiotic therapy is indicated for 5 to 7 days. Tetanus prophylaxis should be administered.
Improper repair of eyelid lacerations can lead to abnormal function and secondary problems, including chronic epiphora and associated dermatitis, exposure keratitis, ulcerative keratitis, cicatricial entropion or ectropion, conjunctivitis, and pigmentary keratitis.
Trauma to the Nictitating Membrane
Lacerations involving the nictitating membrane (third eyelid) should be repaired to avoid irritation and damage to the cornea. This appears to be more important in horses than in ruminants. The margin should be realigned as precisely as possible, and the lacerated conjunctiva should be repaired with absorbable small suture material such as 5-0 to 7-0 polyglactin (Vicryl [Ethicon, Somerville, N.J.]). Topical ophthalmic antibiotics should be used 3 to 6 times daily for 7 to 10 days. The entire nictitating membrane should be excised only if it is irreparably damaged.
Trauma to the Conjunctiva palpation, the anterior chamber is shallow or flat, or hyphema or subconjunctival hemorrhage is present.8
Chemosis and subconjunctival hemorrhage frequently resolve without therapy. However, if the chemosis is severe enough to cause exposure and desiccation, sterile ophthalmic lubricants or antibiotic ointments are indicated to prevent secondary irritation. Conjunctival lacerations rarely require closure unless they are extensive. Subconjunctival hemorrhage sustained during parturition is common in foals and calves and requires no therapy, although topical ocular lubricants or antibiotic ointments are often prescribed.
Trauma to the Cornea
Corneal injuries in horses and food animals include blunt compressive trauma, foreign body penetration, ulcerative keratitis, and lacerations. Corneal perforation often results in iris (or iris and ciliary body) prolapse. Therapy is dictated by the type and extent of corneal injury, the complications encountered, the intended use and economic value of the animal, and other financial considerations.
Blunt Trauma to the Cornea
Blunt trauma to the globe from lead shanks, whips, and other objects can result in corneal endothelial injury and subsequent edema. Signs of traumatic uveitis also may accompany such an injury. The corneal edema that results from blunt trauma to the globe may be focal, linear, or diffuse. Therapy for blunt trauma includes a topical hypertonic (5%) saline solution or ointment two to four times a day to decrease corneal edema. Flunixin meglumine or phenylbutazone at antiinflammatory dosages may also be used if uveitis is present. A linear keratopathy characterized by a nonedematous, deep, striate, refractile opacity in the cornea may represent a focal thinning or break in the Descemet's membrane in these cases. This type of lesion must be distinguished from Haab's striae, which are linear breaks in the Descemet's membrane that result from elevated IOP in glaucoma.
Corneal Foreign Bodies
Plant matter embedded in the epithelium or superficial stroma is the most frequently encountered corneal foreign body. Foreign bodies usually are easily removed with hydropulsion, a moistened cotton-tipped applicator, or ophthalmic forceps. Sedation, motor or sensory nerve blocks, and topical anesthesia facilitate removal. Culture and sensitivity tests and cytologic examination of corneal samples are recommended to guide antimicrobial therapy. Fluorescein staining helps evaluate the extent of corneal ulceration. While awaiting laboratory results, medical therapy should include a broad-spectrum topical ophthalmic antibiotic (e.g., bacitracin-neomycin-polymyxin three to six times daily) and atropine as needed. In horses, treatment with a topical antifungal agent (e.g., miconazole three to four times daily) may also be warranted. The prognosis is guarded until the cornea heals; the eye should be reevaluated in 24 to 48 hours.
Complications of corneal foreign bodies include bacterial and fungal infection, corneal perforation, and severe corneal scars that may restrict vision. Subpalpebral lavage systems are used in severe injuries when frequent prolonged therapy is needed or when treating intractable animals (see the Infectious Ocular Diseases, Keratitis section later).13 Originally, the placement of the subpalpebral catheter was described in the middle tolateral fornix of the upper eyelid, although many practitioners place the lavage system in the medial aspect of the inferior eyelid, allowing the third eyelid to protect the cornea from trauma from the lavage catheter itself.14
Corneal Ulcers
Corneal ulcers in horses are usually initiated by trauma and should be considered contaminated by bacteria or fungi until proven otherwise. Trauma may play a lesser role in food animals, in which primary infectious etiologies are more common (see the Infectious Bovine Keratoconjunctivitis [IBK] section later). The conjunctival fornices, third eyelid, and eyelids should be carefully examined for foreign material. Diagnosis is based on cytologic examination, culture and sensitivity testing of corneal samples, and fluorescein staining of the cornea. Material for bacterial and fungal culture is collected from the ulcer with sterile rayon-tipped swabs. Cotton swabs are less satisfactory because cotton exhibits some antimicrobial properties. The eyelid margins and skin should be avoided, and better culture results are obtained if the swab is moistened with a sterile solution (sterile water or saline) before specimen collection. The most reliable results are obtained if the swabs are placed in a transport medium at the time of collection (Port-A-Cul [Becton Dickinson, Sparks, Md.]). Immediately after collection, the swab is replaced in the tube or inoculated onto standard bacterial and fungal agar plates, or blood agar and thioglycolate broth.
Corneal scrapings for microscopic examination are collected with the use of topical anesthesia. The eyelids are retracted, and the margin of the corneal ulcer is gently rubbed with a small brush, a cytology spatula, or the blunt handle end of a Bard-Parker scalpel blade until a small amount of cellular material is collected. This material is transferred to clean glass slides, spread over a 1-cm area, and allowed to air-dry. Slides may be stained in-house with Diff-Quik and/or Gram stain to assess the presence and type of microorganisms and inflammatory cells.
Therapy of corneal ulcers is based on the removal of the cause if it is still present, control or prevention of infection with topical antimicrobials, use of topical atropine for relief of painful ciliary body spasm and prevention of synechia, and, in horses, systemic use of nonsteroidal antiinflammatory drugs (NSAIDs) such as flunixin meglumine or phenylbutazone. The initial choice of topical antibiotic should be based on the results of cytologic evaluation and modified later if necessary, according to the results of culture and sensitivity testing. If gram-positive organisms are demonstrated on corneal cytology, several surveys of bacterial susceptibility suggest that topical chloramphenicol or fluoroquinolones are a good first choice of therapy.15 If gram-negative organisms are seen, initial empirical therapy should include a topical aminoglycoside or fluoroquinolone antibiotic,15 but since the ocular flora is primarily gram-positive, use of broad-spectrum combinations such as bacitracin- neomycin-polymixin B should be considered. Susceptibility testing ideally should be performed for every infected ulcer given the increasing resistance seen for bacterial pathogens. If cytology demonstrates fungal hyphae, initial therapy with a topical antifungal agent should be instituted immediately. In a recent study of fungal isolates from equine ulcerative keratomycosis cases, voriconazole was shown to be the most effective antifungal drug for initial therapy.16 Subpalpebral lavage systems greatly facilitate the delivery of topical medication to the equine eye.13,14
Surgical intervention should be considered in cases of deep corneal ulceration and especially when Descemet's membrane is exposed. Surgical procedures most often used for corneal ulceration include conjunctival pedicle flap and keratoplastic procedures. Ophthalmic tissue adhesives and soft contact lenses may also be used as nonsurgical therapy for deep corneal ulcers. Perforating ulcers with iris prolapse and mixed bacterial and fungal keratitis or ulcers present for more than 2 weeks usually have a poor visual outcome.17
Corneal Lacerations
Corneal lacerations may be caused by sharp, protruding objects or projectiles. They can occur with or without scleral laceration and, if they are partial thickness, may be treated as corneal ulcers. By contrast, perforating corneal lacerations must be repaired surgically. Preoperative preparation includes tetanus prophylaxis (horses and goats), systemic antibiotics, and sample collection for corneal culture and sensitivity. Ocular ultrasonography is useful in determining the integrity of intraocular structures. However, care must be exercised during ocular examination, ultrasonography, and surgery and anesthesia (especially induction and recovery) because extrusion of the intraocular contents may occur if excessive pressure is exerted on the globe or if the eyelids are forced open. In some cases, complete examination of the globe should be delayed until the animal is anesthetized.
General anesthesia, adequate magnification, proper instrumentation, appropriate suture material and needles, and adequate postoperative care are necessary for successful repair of a corneal laceration. Postoperative therapy must include topical antibiotics and mydriatics or cycloplegics, along with systemic antiinflammatory agents. The prognosis for recovery of vision and preservation of the globe generally is guarded. Complications that may occur after repair of corneal lacerations include phthisis bulbi, corneal fibrosis, synechia formation, blindness, retinal detachment, cataract formation, uveitis, endophthalmitis, bacterial or mycotic keratitis, and wound dehiscence with subsequent iris prolapse.
The prognosis after surgical repair of corneal or corneoscleral lacerations is best when the animal is presented immediately with a small wound in which the cornea or sclera is sealed and the anterior chamber has reformed. Minimal hyphema, clear intraocular media, a clearly visible fundus, and laceration length of less than 15 mm are additional findings that indicate a favorable prognosis.17 In horses the success rate when only the cornea is involved is about 70% for recovery of vision and 90% for a cosmetically acceptable globe.18 With corneoscleral lacerations, the prognosis is much worse. In our experience, the success rate in such cases is 20% for recovery of vision and 70% for a cosmetically acceptable globe. Most phthisical globes are not considered cosmetically acceptable. Therefore enucleation should be considered initially with severe corneoscleral lacerations because the prognosis is poor for return of vision and guarded for preservation of the globe. Several surgical procedures have been described in horses to provide a cosmetic appearance to the globe and orbit, including placement of an
,
19 20 intraocular silicone prosthesis.19,20
Trauma to the Uveal Tract rarely, oral corticosteroids. Care must be taken to avoid secondary complications from systemic corticosteroids.
Trauma-induced hyphema usually has a good prognosis if the blood has clotted and fills less than half the anterior chamber. Stall rest, topical 1% atropine, topical corticosteroids, and systemic antiinflammatory therapy should be instituted to control the associated uveitis. If a penetrating wound is suspected, topical and systemic antibiotic therapy should be included with periodic fluorescein staining. Surgical intervention to remove large blood clots is rarely indicated because it may result in additional bleeding or may worsen the uveitis. Dilute tissue plasminogen activator (tPA; Activase [Genentech, South San Francisco, Calif.]), 25 to 50 μg, may be injected into the anterior chamber to disrupt or lyse intraocular hemorrhage and fibrin and to aid in resolution of synechiae. For maximum effectiveness, tPA should be used within 24 to 72 hours of clot formation, although clot lysis by tPA may still occur up to several weeks after the traumatic incident.21,22
Chronic uveitis after ocular trauma may be associated with lens damage or the introduction of infectious or foreign agents into the eye and carries a poor prognosis. If the lens is ruptured, its surgical removal is advocated. Ocular perforation is a frequent cause of panophthalmitis in food animals and horses. Although therapy consists of systemic and topical antibiotics, as well as tetanus prophylaxis in susceptible species, panophthalmitis usually necessitates eventual enucleation.
Trauma to the Lens
Blunt or sharp trauma to the eye may damage the lens by causing lens opacity (cataract), by rupturing the lens capsule, or less often by causing a shift in position (subluxation or luxation). Release of lens protein into the eye after lens capsule rupture may induce severe granulomatous uveitis. In such cases the eye should be treated vigorously for lens-induced uveitis with topical atropine and topical and systemic antiinflammatory drugs. If the globe has been penetrated, topical and systemic antibiotics are indicated. The prognosis for preservation of vision is poor. Lens removal may be required to control the inflammatory response.
Cataracts (lens opacities) associated with ocular trauma may occur acutely or develop weeks after the initial injury. The opacity may be focal and not appreciably affect vision, or it may be complete and cause a visual deficit. If the remainder of the eye is normal, surgical removal of the cataractous lens may improve vision.23,24 In a recent retrospective study of surgical cataract removal in horses, the highest success rate was noted in the removal of traumatic cataract, as compared with cataracts of other known etiology.24
Trauma Involving the Vitreous
Trauma to the eye may result in hemorrhage into the vitreous or release of inflammatory products that cause vitreal degeneration. Either circumstance can result in vitreal syneresis (liquefaction), formation of vitreal traction bands, and subsequent retinal detachment. Symptomatic treatment of inflammation is generally adequate, but vitrectomy may be beneficial in the management of vitreal traction bands to prevent subsequent retinal detachment.25
Trauma to the Retina
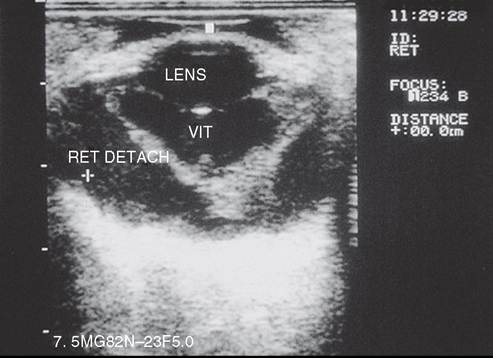
FIG. 39.8 Ocular ultrasound of a horse eye after blunt trauma to the globe. Note the characteristic V-shaped retinal detachment.
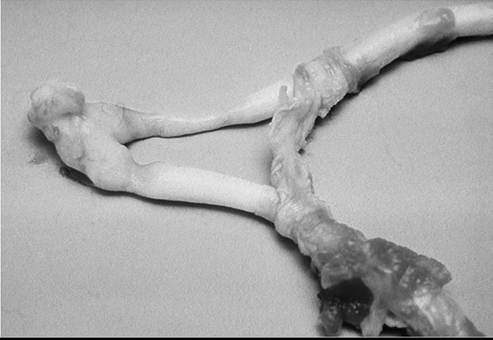
FIG. 39.9 Optic nerves and chiasm of a foal that was blind as a result of head trauma. Note the constrictions of the optic nerves caused by necrosis and degeneration. (Courtesy Dr. C.L. Martin.)
retinal tears, lacerations, or detachments in food animals and horses may be feasible in selected cases.
Trauma to the Optic Nerve
The pathogenesis of damage to the optic nerve is not well understood. Shearing forces at the optic foramen from displacement of the brain after severe head trauma (Fig. 39.9), direct contusion or avulsion of the optic nerve, or loss of blood supply to the nerve and subarachnoid hemorrhage probably all have roles in optic nerve injury.27 Early examination may reveal only a dilated pupil that may be partially or completely unresponsive to light. Later, changes may include optic nerve atrophy (Fig. 39.10) and peripapillary retinal pigmentation changes. Therapy with systemic antiinflammatory drugs may be of benefit, but severe damage is usually irreversible.
Traumatic optic nerve atrophy is usually characterized by sudden onset of unilateral or bilateral blindness, dilated fixed pupils, and a lack of menace response. In horses the traumatic episode is frequently characterized by damage to the poll from rearing over backward and striking the back of the head, from rearing up and hitting a ceiling beam, or from blunt trauma (blows) to the side or front of the face. The animal usually stands without loss of consciousness, and the injury is not
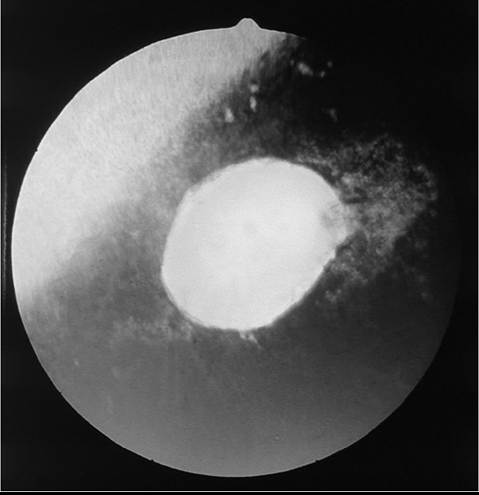
FIG. 39.10 Appearance of optic nerve 3 months after head trauma in a horse. Note the pale optic disk and peripapillary retinal degeneration. (Courtesy Dr. C.L. Martin.)
of the affected area with copious amounts (500 to 2000 mL) of sterile saline solution. Tap water may be used by the owner until veterinary assistance is available. It may be necessary to sedate the animal. No attempt should be made to neutralize the substance because this may cause precipitation within the cornea. The damage should then be evaluated with the aid of local nerve blocks.
Treatment should include appropriate topical antimicrobials, atropine, and a collagenase inhibitor such as autologous serum or possibly 5% to 10% acetylcysteine (Roxane Laboratories Inc., Columbus, Ohio), which inhibits collagenases and metalloproteinases by binding calcium. Hourly application of serum or acetylcysteine may be needed. Systemic antiinflammatory drugs should be used to control secondary uveitis. Therapeutic soft contact lenses have been used to protect the corneal stroma in patients with extensive corneal ulcerations.
Thermal Injury
Facial burns secondary to barn or stable fires may damage the eyelids, conjunctiva, and corneas. Therapy for minor burns to the eyelids is directed toward keeping the injured area moist with antibiotic dressings and protecting the cornea if eyelid dysfunction occurs. Treatment for injury to the conjunctiva or cornea should include topical antibiotic and systemic antiinflammatory drugs in horses. Full-thickness eyelid burns may require grafting procedures to protect the cornea and minimize scarring. Third eyelid or conjunctival flaps may be required to protect the cornea until eyelid function returns.
considered serious by the owner at the time. Initially, blindness with a normal-appearing ocular fundus is observed.
Within 3 to 4 weeks after the trauma, examination of the fundus reveals a pale optic disk (see Fig. 39.10). Later, loss of peripapillary retinal vessels is usually evident. The optic disk often appears depressed, with increased prominence of the lamina cribrosa. Confirmation of optic nerve or optic tract lesions causing blindness may be made by the absence of a direct PLR with a normal electroretinogram. In some cases, the pathologic lesion is a rupture of the nerve axons from stretching forces produced by movement of the brain.27 Chiasmal hemorrhage and fractures of the basisphenoid bone may be observed at necropsy. Therapy with systemic corticosteroids (dexamethasone, 2.5 to 5 mg IV or IM) and IV dimethyl sulfoxide (DMSO) has generally not been suc- cessful,27 although the lack of response to medical therapy appears related to the severity of the injury.
A segmental optic nerve atrophy involving one to three quadrants of the optic disk occurs in horses. The appearance is characterized by pallor, loss of normal vasculature, and increased prominence of the lamina cribrosa in the affected quadrants. The etiology is unknown, but traumatic injury is suspected in most cases. Response to medical therapy is poor.
Chemical Injury