Infectious Ocular Diseases
Caryn E. Plummer
This section describes the major infectious ophthalmic diseases of large animals (Table 39.3). Infectious bovine keratoconjunctivitis (IBK), or “pinkeye,” the most common ocular disease of cattle, will be discussed in another section.
Infectious ocular disease in large animals may be either the result of a pathogen primarily affecting the ocular tissues or an ocular manifestation of a systemic infection, wherein the ocular signs are secondary or concurrent to the systemic illness. As a general rule, surface ocular diseases are often primary in origin, whereas intraocular diseases are either primary or secondary. The first infections described in this section are those with predominantly ocular signs, followed by descriptions of ocular manifestations of systemic disease.There are many potential ophthalmic manifestations of infectious disease in large animals. Few diseases have pathognomonic or classically distinctive signs, so the combination of signalment, ocular clinical signs, systemic clinical signs, and laboratory diagnostics are necessary to confirm a diagnosis. Clinical signs associated with conjunctivitis are nonspecific to the underlying cause and include conjunctival hyperemia and chemosis. Other clinical signs may include follicle formation (often a manifestation of chronicity) and serous to mucopurulent discharge. Differentiation of primary conjunctivitis from secondary conjunctivitis resulting from other diseases (systemic disease or intraocular disease) is very important. A thorough ophthalmic examination will help with this determination.
In cattle and small ruminants, corneal disease may be initiated by an infectious agent, but infectious corneal disease in horses most often occurs secondary to corneal trauma. It can also be a manifestation of primary ocular disease or systemic disease. Signs of keratitis include pain (blepharospasm, photophobia, epiphora), ocular discharge, corneal edema, variable corneal vascularization, loss of stromal integrity (melting or keratomalacia), and secondary anterior uveitis.
■ TABLE 39.3
Major Infectious Ocular Diseases of Large Animals
| Agent | Common Name/Disease | Major Sign(s) | Cattle | Sheep | Goats | Horses |
| Mycoplasma conjunctivae | Pinkeye | Keratoconjunctivitis | ++ | ++ | ||
| Mycoplasma mycoides subsp. | Pinkeye | Keratoconjunctivitis | + | |||
| mycoides | ||||||
| Acholeplasma oculusi (oculi) | Pinkeye | Keratoconjunctivitis | + | + | ||
| Chlamydia psittaci | Pinkeye | Keratoconjunctivitis | ++ | |||
| Branhamella (Neisseria) | Pinkeye | Keratoconjunctivitis | + | + | ||
| Mycoplasma agalactiae | Keratoconjunctivitis | + | + | |||
| Mycoplasma arginini | Keratoconjunctivitis | + | + | |||
| Listeria monocytogenes | Keratoconjunctivitis | + | + | |||
| Bovine herpesvirus type 1 | Keratoconjunctivitis | ++ | + | |||
| (infectious bovine | ||||||
| rhinotracheitis) | ||||||
| Colesiota (Rickettsia) conjunctivae | Pinkeye | Keratoconjunctivitis | + | |||
| Equine viral arteritis | Keratoconjunctivitis | + | ||||
| Equine herpesvirus type 2 | Keratoconjunctivitis | + | ||||
| Mycoplasma bovoculi | Conjunctivitis | + | ||||
| Ureaplasma spp. | Conjunctivitis | + | ||||
| Equine adenovirus | Conjunctivitis | + | ||||
| Moraxella spp. | Conjunctivitis | bgcolor=white>+ | ||||
| Streptococcus equi | Strangles | Conjunctivitis | + | |||
| Moraxella bovis | Pinkeye | Corneal ulcer | ++ | |||
| Equine herpesvirus type 1 | Rhinopneumonitis | Keratitis | + | |||
| Malignant catarrhal fever | Uveitis, keratitis | + | ||||
| Neonatal septicemia | Uveitis | + | + | + | + | |
| Mycobacterium bovis | Tuberculosis | Uveitis | + | |||
| Salmonella spp. | Uveitis | + | ||||
| Borrelia burgdorferi | Lyme disease | Uveitis | + | |||
| Leptospira interrogans | Recurrent uveitis | + | ||||
| Brucella abortus | Recurrent uveitis | + | ||||
| Scrapie | Retinitis | + | ||||
| Histophilus somni (formerly | Infectious thromboembolic | Retinitis | + | |||
| Haemophilus somnus) | meningoencephalitis | |||||
| Bovine viral diarrhea | Retinal dysplasia, cataracts | + | ||||
| Bluetongue | Chorioretinitis, conjunctivitis | + | + | |||
| Toxoplasma gondii | Chorioretinitis | + | ||||
| Rhodococcus (Corynebacterium) equi | Panophthalmitis | + | ||||
| Bovine leukemia virus | Exophthalmos | + | ||||
| Cryptococcus neoformans | Exophthalmos | + |
Uveitis is inflammation of the uveal tract, which includes the iris, ciliary body, and choroid.
Initial clinical signs may include episcleral injection, blepharospasm, photophobia, miosis, aqueous flare, hypopyon, fibrin, hyphema, and corneal edema. Intraocular inflammation can affect the entire eye and may result from direct invasion of the globe by a pathogen or as the result of a systemic inflammatory response. If untreated, uveitis can lead to permanent vision loss, cataract, secondary glaucoma, and phthisis bulbi. Some systemic infections may result in neuro-ophthalmic signs, such as facial nerve paralysis, Horner's syndrome, trigeminal neuropathies, nystagmus, strabismus, or ptosis. Others may cause retrobulbar disease or periorbital swelling.This section addresses viral-, bacterial-, and fungal-mediated ocular disease; parasitic infections are addressed in a separate section. Many viral diseases affect the eye either directly or indirectly. Those that affect the globes may require direct ocular management. Other infections mediate disease primarily through cranial nerve neuropathy, and management is supportive. Any systemic bacterial infection has the potential to affect the eyes. Certain specific bacterial diseases (e.g., tetanus, botulism) may have their own distinctive ophthalmic signs, but most bacterial infections, especially when sepsis has developed, can be associated with nonspecific ocular inflammation. Fortunately, systemic fungal infections are not common in the immunocompetent animal, although ocular surface infections are common, especially in the horse. For more detailed information on the specific ocular conditions mentioned in this chapter, consult an ophthalmology textbook and the recent literature.
Conjunctivitis and Keratoconjunctivitis clinical signs began on day 2 and lasted for 5 weeks.9 Later in the disease, keratitis with corneal neovascularization (Color Plate 39.16) and occasionally anterior uveitis can be seen.1,10 One case of choroiditis and hyalitis has been described.11 Signs can be seen in individuals, as well as in herd or flock outbreaks.
The disease is usually unilateral but can be bilateral. Differential diagnoses include other infectious causes of keratoconjunctivitis, such as Chlamydophila spp. (sheep), Branhamella spp., aerobic bacteria, parasites, and infectious bovine rhinotracheitis (goats), as well as noninfectious causes such as trauma. There may be a slight variation in clinical signs experienced by sheep and goats. Although both will exhibit blepharospasm, conjunctivitis, and keratitis, sheep will occasionally develop a more severe form of the disease associated with mucopurulent conjunctivitis, corneal ulceration, and uveitis with hypopyon (Color Plate 39.17). Goats do not typically ulcerate their corneas, despite the presence of severe and vision-threatening keratitis.■ Clinical Pathology In conjunctival scrapings taken early in the disease, many neutrophils are seen; later, lymphocytes predominate. Plasma cells and necrotic epithelial cells are also observed.12 Organisms can occasionally be found in epithelial cell cytoplasm in coccobacillary or varied forms.11 Pigment granules can be mistaken for organisms.6,12,13
Mycoplasmal organisms can be cultured and identified from conjunctival swabs; serum antibody titers can be measured,14,15 or PCR can be used to identify M. conjunctivae in conjunctival smears.16,17 Egwu and Faull18 describe rising serum and lacrimal antibody titers in sheep topically inoculated with M. conjunctivae. However, Trotter and colleagues2 report low serum titers to M. conjunctivae in normal animals and no rise in titer in animals subconjunctivally inoculated with M. conjunctivae that subsequently developed signs of disease.
■ Epidemiology Mycoplasmal infections apparently are transmitted directly from animal to animal, as evidenced by herd or flock outbreaks. Subclinical carrier states exist, and M. conjunctivae can be cultured from nonclinical animals.19,20 There is some evidence for vector transmission (flies) as well.21 Animals can become reinfected, but if they do, their clinical signs are usually more mild than during the initial infection.
Keratoconjunctivitis can be induced in sheep with topical inoculation of M. conjunctivae.19,11'13 Clinical signs were identical to natural outbreaks and spread to uninoculated sheep. The organism can be cultured from eyes long after clinical signs abate.9 Co-infection with other organisms may occur and result in more severe clinical signs.■ Treatment and Prognosis In most animals, mycoplasmal keratoconjunctivitis associated with M. conjunctivae is transient. Affected animals usually recover spontaneously in 10 days, although some animals seem to have recurring episodes that last for several weeks. In a controlled clinical trial, one dose (20 mg/kg) of long-acting oxytetracycline was given to experimentally inoculated lambs. This treatment seemed to hasten the cessation of clinical signs, although the results were not analyzed statistically.14 The treatment did not, however, eliminate the M. conjunctivae infection and may promote a carrier state. Other drugs recommended for the ocular disease include topical oxytetracycline or oxytetracycline and polymyxin B.1 Subconjunctival oxytetracycline is not currently recommended because it may cause a severe inflammatory reaction. In vitro antibiotic testing of M. conjunctivae shows that flor- fenicol, tylosin, oxytetracycline, streptomycin, and chlortetracycline are suitable for treatment.25,26
■ Prevention and Control Introduction of new animals into a herd or flock has been implicated in starting an outbreak of keratoconjunctivitis. Therefore isolation and, if necessary, treatment of new animals are important before contact with the herd.17-19 Transmission between species has been documented, so housing domestic sheep and goats where they might commingle with wildlife is not recommended.17,18 No other specific recommendations have been made for prevention and control of M. conjunctivae.
Bovine Mycoplasmal Conjunctivitis
Mycoplasma bovoculi and Ureaplasma spp.
have been isolated from cattle with conjunctivitis and IBK. Inoculation of normal calves with Mycoplasma bovoculi or Ureaplasma isolates produced conjunctivitis characterized by serous discharge and conjunctival hyperemia. Experimentally induced conjunctivitis ran a course of more than 1 month. Cases can be confirmed by culture or PCR performed on conjunctival swabs.30 Mycoplasmal infection may predispose the animals to development of IBK from Moraxella bovis31,31 (see the Infectious Bovine Keratoconjunctivitis [IBK] section later). Therefore although treatment of mycoplasmal conjunctivitis may not be warranted, it may be advisable in areas where IBK is endemic. Topical oxytetracycline ointment applied three times daily or intramuscular (IM) injection of long-acting oxytetracycline is recommended.Other mycoplasmal organisms (e.g., M. arginini) can be isolated from cows' conjunctiva but are not thought to cause the disease. Mycoplasma bovis was found using PCR performed on normal conjunctival samples,19 but it was not thought to cause conjunctivitis. Mycoplasma bovigenitalium, Mycoplasma bovirhinis, and Mycoplasma bovoculi were isolated from members of two cattle herds with conjunctivitis and bronchopneumonia.31 However, when viral cultures were performed, bovine herpesvirus type 1 (BHV-1; also called infectious bovine rhinotracheitis [IBR]) was isolated in the same individuals. The mycoplasmal organisms may have contributed to the disease in these herds. In another cattle herd with an outbreak of respiratory disease, keratoconjunctivitis followed, and Mycoplasma bovis, M. bovirhinis, and Mycoplasma bovoculi were isolated in various combinations from affected calves.33
■ Chlamydial Keratoconjunctivitis in Sheep and Goats
Definition and Etiology
Chlamydial agents have been isolated from outbreaks of keratoconjunctivitis in sheep flocks. The agent was originally described as a strain of Chlamydia psittaci.
The agent was called Chlamydophila pecorum for a period of time but is currently designated Chlamydia pecorum, which can also cause abortion (see Chapters 31 and 35) and polyarthritis in lambs.34,35■ Clinical Signs and Differential Diagnoses Early clinical signs consist of epiphora, chemosis, and conjunctival hyperemia. Later in the disease, follicle formation in the conjunctiva becomes prominent. Still later, corneal vascularization may be seen (Color Plate 39.18). Most cases are bilateral and symmetric.36,37 In some flock outbreaks of keratoconjunctivitis, outbreaks of polyarthritis are also noted. Most lambs that develop chlamydial polyarthritis will also develop conjunctivitis.36,37 Differentials include other infectious causes of keratoconjunctivitis, such as Mycoplasma and Branhamella (Neisseria) spp., aerobic bacteria, and parasites, as well as noninfectious causes like trauma.
■ Clinical Pathology Early in the disease, conjunctival smears show numerous neutrophils and some lymphocytes. Later, there are more neutrophils and fewer mononuclear cells. Cytoplasmic chlamydial inclusions are occasionally seen in up to a third of the eyes scraped and can be definitively identified by fluorescent antibody staining.34 Conjunctival epithelial cells are often necrotic. Chlamydial organisms can be cultured from conjunctival scrapings and from blood taken from sheep with polyarthritis and conjunctivitis.36-38 In one study, titers to chlamydial antibodies were found at 1 : 16 or higher in a number of the affected lambs, although titers on normal lambs were not reported.37 PCR can also be used to identify the organism.
■ Epidemiology Chlamydial organisms are apparently transmitted by direct contact, as evidenced by flock outbreaks. Chlamydial organisms caused conjunctivitis in five lambs inoculated topically.38 An uninoculated lamb housed with the five lambs also developed conjunctivitis. Lambs subsequently developed follicular conjunctivitis.38 In another study, chlamydial organisms were injected intraarticularly, intravenously, and intramuscularly and caused polyarthritis and conjunctivitis.39
■ Treatment and Prognosis In uncomplicated cases the disease is self-limiting, and eyes are normal within 2 to 3 weeks.37 The same treatments indicated for M. mycoides subsp. mycoides (systemic oxytetracycline and, when possible, a topical tetracycline ophthalmic preparation) are also effective in treating chlamydial conjunctivitis and polyarthritis of sheep.
Branhamella (Neisseria) ovis Keratoconjunctivitis in Sheep and Goats
Branhamella ovis is a gram-negative diplococcus similar to Moraxella. This agent has been cultured from the eyes of sheep and goats with keratoconjunctivitis and from normal eyes.40-42 B. ovis has also been cultured from cattle with serous conjunctivitis and, rarely, keratitis.43 Clinical signs are usually mild and include epiphora and conjunctival hyperemia. Severity of clinical signs is increased when co-infections with other organisms, such as M. conjunctivae, are present. Conjunctivitis but not keratitis has been experimentally induced in goats44 and lambs,45 and B. ovis could be cultured from the eyes of the lambs for up to 20 days after inoculation. Outbreaks of B. ovis have been successfully treated with parenteral tylosin, topical neomycin-polymyxin B, and a corticosteroid,40 or with subconjunctival penicillin.44
Moraxella Conjunctivitis in Horses
Two reports have described a Moraxella species recovered from several horses in herd outbreaks of conjunctivitis, ocular discharge, and erosions of eyelid epithelium at the canthi.46,47 The organism was similar but not identical to Moraxella bovis, and the disease was reproduced experimentally in horses by instillation of the organism into the conjunctival sac. Huntington and colleagues47 described successful treatment of the lesions with chloramphenicol ointment, whereas Hughes and Pugh46 described the lesions as healing spontaneously.
Keratitis
■ Bacterial Keratitis in Horses
Definition and Etiology
Bacterial keratitis occurs when a traumatic corneal ulcer becomes infected with opportunistic bacteria; no bacteria are known to initiate corneal ulcers in horses. The most devastating clinical manifestations are associated with Pseudomonas aeruginosa and Streptococcus equi subsp. zooepidemicusj9~56 However, any bacteria that have access to the ocular surface may colonize and complicate a corneal wound.52,53,57
■ Clinical Signs and Differential Diagnoses Whether infected or not, corneal ulcers cause signs of pain (blepharospasm, epiphora, photophobia). The conjunctiva is hyperemic, and the ulcerated area of the cornea retains fluorescein stain. Acute superficial ulcers are usually not infected, and the cornea maintains its normal curvature in the ulcerated area. If a superficial ulcer is slow to heal, it should be sampled for microbial C&S, since delayed healing may be a sign of an early or subclinical infection. A deep ulcer (resembling a divot in the corneal stroma) should always be assumed to be infected.
Other signs of corneal infection are rapid progression and white or yellowish infiltrate within the cornea (signifying influx of neutrophils and bacterial colonization within the corneal stroma). An ulcer that is rapidly becoming wider or deeper or begins to melt (corneal stroma softens or begins to dissolve) is highly suggestive of a bacterial infection (Color Plate 39.19). Many corneal ulcers are accompanied by some degree of anterior uveitis (miosis, aqueous flare, hypopyon, anterior chamber fibrin). The uveitis that occurs during a corneal infection tends to be much more severe than that which is present with sterile corneal wounds (see Color Plate 39.7). In cases in which the initially damaged epithelium heals over microorganisms in the corneal stroma, a bacterial stromal abscess may form.58 Such lesions do not stain with fluorescein, and many topical antibiotics cannot penetrate the epithelial barrier to reach the site of infection. Most stromal abscesses, particularly if they are located in the deep or posterior stroma, are fungal in etiology.59-61 Fungal keratitis may exhibit similar clinical behaviors and may become secondarily infected with bacteria.
■ Clinical Pathology A diagnosis of a bacterial keratitis is made via corneal cytology and microbial C&S. Stained scrapings from the ocular surface wound may show intracellular and extracellular bacteria and neutrophils (Fig. 39.11). Bacterial morphology and Gram staining will guide the choice of empirical therapy while the results of C&S are pending. Bacterial organisms are definitively identified after culture of the ulcerated cornea. Aerobic culturing techniques are usually used. Culturing for anaerobic organisms may be indicated if aerobic culture does not reveal an organism and the ulcer fails to respond appropriately to medical therapy. Anaerobic infections are far less common than aerobic bacterial and fungal infections in the equine cornea.57
■ Pathophysiology Bacterial keratitis is the result of pathogenic or opportunistic organisms colonizing a damaged cornea. The cornea is most likely to be damaged by mechanical trauma, but other causes such as chemical injury or corneal exposure are possible. Many different types of bacteria can be cultured from a normal eye, including Corynebacterium, Streptococcus, Staphylococcus, Bacillus, and rarely Pseudomonas spp. or other gram-negative bacteria.48,50 Damage to the epithelium enables
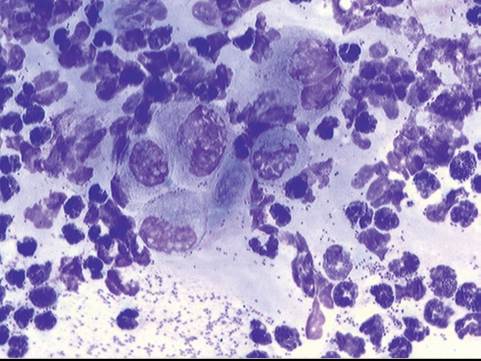
FIG. 39.11 Cytology of bacterial keratitis. Wright-Giemsa, ?100. Note the corneal epithelial cells in the center of field, numerous degenerate neutrophils, and intracellular and extracellular cocci and diplococci bacteria.
bacteria to adhere to the exposed corneal stroma, colonize, and begin replicating.54 Some bacteria such as Pseudomonas elaborate collagenases and other proteoglycanolytic enzymes,55 which results in corneal collagen destruction. Proteases and collagenases liberated by white blood cells and corneal epithelial and stromal cells also contribute to this “melting” process.62,63 In this way, what begins as a small wound to the cornea can progress to a corneal perforation within 24 to 48 hours.
■ Treatment and Prognosis Prognosis is guarded for any corneal ulcer that is rapidly progressing or melting. These ulcers can easily progress to corneal perforation and loss of vision or of the eye despite timely, appropriate treatment. On the other hand, with aggressive therapy many eyes with infected ulcers can be saved and vision maintained, although scarring may be present.
In any ulcer in which a bacterial component is suspected, C&S of the ulcer and a corneal scraping for Gram staining and cytology should be taken. The horse is restrained or sedated and an auriculopalpebral block is performed. A sample for culture should be obtained with a moistened swab before any solutions or medications are applied to the eye. Following culture, a topical anesthetic is applied to the cornea, and the ulcer margins are then scraped gently with a cytology brush, a Kimura spatula, or the blunt handle end of a scalpel blade.
In cases of equine bacterial keratitis, therapeutic goals are to eliminate the bacteria, prevent or slow melting if present, and treat the concurrent uveitis.64-66 Because this requires very frequent applications of numerous medications to a horse with a painful and often fragile eye, a subpalpebral lavage system is usually required.
PLACEMENT OF SUBPALPEBRAL LAVAGE SYSTEM. The following equipment is necessary:
• Subpalpebral lavage (SPL) kit (MILA International [Fig. 39.12])
• White tape
• Applicator stick (tongue depressor)
• Injectable anesthetic (lidocaine, mepivacaine)
• Topical ophthalmic anesthetic (proparacaine, tetracaine)
• Monofilament nonabsorbable suture on a cutting needle
The horse should be sedated. Additional manual restraint (e.g., twitching) may be necessary depending on the animal's temperament and degree of discomfort and on the handler's comfort and experience. The auriculopalpebral nerve is blocked over the zygomatic arch to paralyze the orbicularis oculi muscle and reduce eyelid movement. If the SPL is to be placed in the upper eyelid, a supraorbital (frontal) block is performed to desensitize the eyelid. This nerve is accessed at its exit from
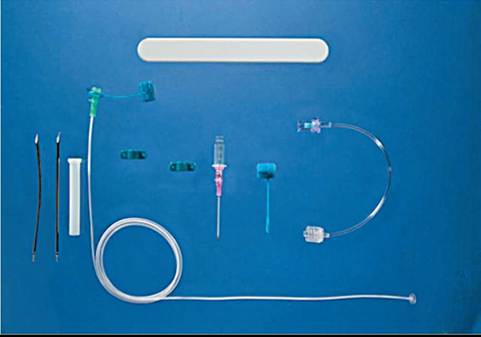
FIG. 39.12 Subpalpebral lavage kit. (Courtesy Mila International Inc.)
the supraorbital foramen. If the SPL is going into the lower lid, a line block is performed along the ventral orbital rim for regional anesthesia. Topical anesthetic is then applied to the eye by directing a gentle stream onto the globe and into the conjunctival fornix with a small syringe with a 25-gauge needle broken off at the hub. The eyelid and conjunctival fornices should be flushed with a dilute Betadine solution (0.5%).
Once the periocular structures are prepared, a gloved finger or the plastic applicator stick or needle guard from the kit is advanced under the eyelid and used as a guide for the needle to which the SPL tubing is attached. The needle is directed between the eyelid and the guide and then through the skin. In the upper eyelid, it should be placed as high as possible and should grab the periosteum of the orbital rim as it exits, which will help keep the lavage footplate in place and decrease the likelihood of slippage and subsequent irritation of the cornea. While passing the needle through the skin, care must be taken not to inadvertently push the end of the needle onto or against the fragile globe. The needle and Silastic tubing are threaded through the hole in the skin until the footplate is in direct contact with the palpebral conjunctiva. Tape is used to secure the tubing to the upper eyelid, and sutures secure the tape to the skin. The tubing can be braided through the forelock and then run down the neck through several braids to keep it secure. A small catheter is directed into the distal end of the tubing, and an injection port is fixed to the end of the catheter. The catheter and tubing are taped to an applicator stick to prevent kinking. The stick is then taped to a braid of the mane (Fig. 39.13).
Poorly placed lavage tubes or tubes that slip ventrally can rapidly produce a corneal ulcer. A displaced tube footplate can also cause topical medications to leak into the subcutaneous tissues, leading to a swollen and inflamed eyelid. Therefore the tube position should be checked at least once daily by gentle dorsal traction on the exposed tubing to ensure that it has not slipped into the conjunctival cul-de-sac. Excess traction will pull the footplate through the conjunctiva and into the eyelid itself. Most horses tolerate this system well, and well-maintained tubing may be kept in place for up to several months. Occasionally horses try to rub their heads and can damage the tubing; neck cradles or protective eye cups can be used in such horses.
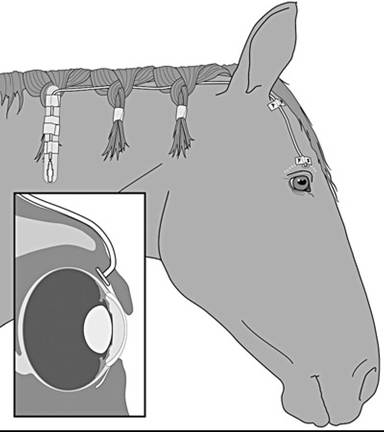
FIG. 39.13 Diagram illustrating a subpalpebral lavage system with correct positioning in superior fornix and fixation with a tape butterfly at exit site of tubing from the eyelid. Tubing is woven through braids in the mane, and injection catheter and stopcock taped to a stick applicator (tongue depressor). (Diagram courtesy Anne Gemensky-Metzler.)
MEDICAL/SURGICAL APPROACHES AND GOALS. For noninfected ulcers a broad-spectrum preparation (e.g., neomycin- polymyxin-bacitracin, neomycin-polymyxin-gramicidin, chloramphenicol) is appropriate. In a cornea with rapidly developing keratitis or melting ulcer, the clinician should always suspect the presence of an infectious agent. Treatment should be initiated with an appropriate antibiotic, the choice of which should be based on cytologic analysis, administered every 1 to 2 hours. If rods or gram-negative organisms are observed, bacitracin-neomycin-polymixin B, aminoglycoside antibiotics (gentamicin, tobramycin), or fluoroquinolones (ciprofloxacin, ofloxacin)67 are reasonable choices for treatment. To avoid contributing to bacterial resistance, fluoroquinolones should not be used for bacterial prophylaxis in noninfected ulcers. If cocci or gram-positive organisms are seen on the corneal cytology, bacitracin-neomycin-polymyxin B, neomycin-polymyxin B-gramicidin, chloramphenicol, levofloxacin or cefazolin, or penicillin or ampicillin can be used.56,66 Cefazolin is mixed with artificial tears to a concentration of 55 mg/mL,61 ampicillin to 10 mg/mL,49 and penicillin G to 100,000 U/mL. If the ulcer continues to worsen, antibiotics should be changed on the basis of the initial susceptibility results, and the cornea should be recultured because organisms can become resistant to the first antibiotic used or a secondary infection can develop. For resistant organisms, susceptibility testing that gives minimum inhibitory concentration (MIC) may be very useful because higher drug concentrations are more readily and safely attainable in the ulcerated cornea than in the systemic circulation.
Keratomalacia (i.e., “melting”) must be treated with collagenase and protease inhibitors, in addition to antimicrobial medications. Autologous serum, oxytetracycline, disodium ethylenediaminetetraacetic acid (disodium EDTA; mixed with sterile water to a concentration of 0.17%), or ATcetylcysteiiie (5% to 10% in artificial tears) can be used topically for their antiprotease and anticollagenase activity, as can systemic doxycycline (10 mg/kg orally [PO] twice daily or 20 mg/kg PO once daily).49,68 Tetanus toxoid, topical doxycycline, and ilomastat have also been applied to the diseased cornea to decrease collagen dissolution.69
Surgical therapy can also be used and may improve prognosis. Conjunctival pedicle grafts can be used to bring a blood supply and conjunctival fibroblasts to deep corneal ulcers, with the goal of slowing progression and aiding stromal reconstruction56 while still allowing medication to reach the wound. A conjunctival graft allows observation of the cornea so that treatment can be adjusted as corneal health improves or changed if the cornea continues to deteriorate. A nictitating membrane “flap” should not be used in rapidly progressing or deep ulcers because it creates a barrier to topical medications and observation of the cornea such that worsening of the ulcer goes unnoticed, repeated culturing cannot be performed, and appropriate changes in therapy cannot be instituted.
A corneoconjunctival transposition using autologous tissue or a corneal graft (penetrating keratoplasty or deep anterior lamellar keratoplasty) using donor cornea is an excellent treatment to repair very deep ulcers, descemetoceles, and perforations if melting has ceased and the ulcers are sterile.60,61,70 Other grafting materials, such as porcine small intestinal submucosa,71 equine amniotic membrane,72 or bovine pericardium, may be substituted for cornea. Placement of any graft requires micro- surgical instruments, techniques, training, and experience. Highly specialized techniques, such as keratectomy with a conjunctival graft, penetrating keratoplasty, posterior lamellar keratoplasty, or deep lamellar endothelial keratoplasty, are necessary to treat stromal abscesses.53,60,73-76
The initial desired response to appropriate therapy of a malacic ulcer is simply cessation of worsening of the ulcer. That is, the ulcer does not appear to be healing or shrinking but also is not becoming larger or deeper. This suggests that bacteria have been killed and tissue destruction has halted. Epithelium will then begin to migrate toward the center of the ulcer, covering the stroma or Descemet’s membrane if it is exposed, and blood vessels will slowly begin growing into the cornea from the limbus. Once re-epithelialization is complete, new infection with microorganisms is unlikely. If surgery has not been performed, however, the area that had been ulcerated will be thinner than the surrounding stroma. This area will gradually thicken by slow reconstruction of stromal collagen by corneal fibroblasts (keratocytes) or when corneal blood vessels fill the old ulcer bed. This can take weeks to months, and until this happens, the cornea may be susceptible to traumatic rupture.
Another goal of therapy for an infected ulcer is suppression of the trigeminal nerve-mediated anterior uveitis that is associated with any corneal irritation. Topical atropine is used for this purpose because it decreases pain associated with ciliary body muscle spasm and maintains pupil dilation, which reduces the chance of posterior synechia formation. Atropine should be applied to effect (i.e., until reduced pain or pupil dilation is noted). This may be as frequently as every 6 to 8 hours initially but should be decreased after 24 hours and used only to effect once pupillary dilation is maintained.77 Because topical atropine is absorbed into the systemic circulation and is associated with altered gastrointestinal (GI) motility,78 small quantities of drug should be applied (1/8- to 1/4-inch strip of ointment or 0.1 mL solution), gut sounds should be assessed frequently, and the patient should be monitored for signs of colic. Systemic NSAIDs also should be used to decrease corneal and uveal inflammation. However, these drugs do slow corneal vascularization to some extent.79,80 Topical NSAIDs (as with corticosteroids) are contraindicated in infected ulcers. Topical corticosteroids are sometimes recommended by some to reduce corneal vascularization once epithelialization is complete. However, corneal vascularization is a critical means by which corneal stroma (and strength) is reformed, and topical corticosteroids hasten regression of granulation tissue, suggesting that this approach is inadvisable. No evidence indicates that corticosteroid administration decreases the final size of the scar, and steroids may compromise healing and predispose to local immunosuppression, additional or persistent infection, and corneal rupture.
■ Fungal Keratitis in Horses
Definition and Etiology
Fungal keratitis (or keratomycosis) occurs when an ulcerated cornea becomes infected with a mycotic organism. As with bacteria, no fungi are known to initiate corneal ulcers. The most common genera isolated in cases of equine fungal keratitis are Aspergillus and Fusarium spp., but many other species of other genera have been cultured.81-86 Horses seem unusually susceptible to fungal keratitis compared with the other domestic species.
■ Clinical Signs and Differential Diagnoses Fungal keratitis is very common in the horse, particularly in certain geographic regions (i.e., southeastern United States), but has been reported all over the world. Nonspecific signs of keratomycosis may include pain (blepharospasm, photophobia), serous to mucopurulent ocular discharge, corneal edema, variable corneal vascularization, loss of stromal integrity (melting or keratomalacia), and secondary anterior uveitis (aqueous flare, hypopyon, fibrin, miosis), which may be severe. Fungal keratitis has various clinical presentations ranging from superficial punctate nonulcerative keratitis, to necrotic plaques, to stromal lesions with keratomalacia and furrowing, to deeper stromal defects or deep stromal abscesses.87,88 A superficial epithelial to subepithelial form presents with microerosions and multifocal, whitish punctate to branching subepithelial opacities that often retain rose bengal stain.89,90 This form, if treated promptly, will usually resolve without incident. However, the forms wherein overt ulceration develops are much harder to control. Superficial fungal ulcers often appear with a roughened, gritty ulcer bed and considerable edema (Color Plate 39.20). Often this form develops into a more severe presentation wherein enzymatic destruction of corneal collagen results in a furrow or groove around the margins of the lesion.91 This furrow is a form of corneal melting and may progress rapidly and lead to corneal perforation. In other cases of keratomycosis, a plaque of tissue that is typically an accumulation of necrotic collagen, degenerating inflammatory cells, and a mat of fungal organisms forms centrally within the ulcer bed (Color Plate 39.21).88,91,92 A very common manifestation of fungal infection is the formation of a white or yellow deep stromal abscess, typically accompanied by corneal vascularization and edema and moderate to severe anterior uveitis (Color Plate 39.22). Fungi have an affinity for the deep corneal stroma and Descemet's membrane, and in severe cases the organisms may invade through the cornea into the anterior chamber. Fungal involvement should be suspected in any corneal ulcer that is associated with plant or organic material; has been treated with corticosteroids; does not heal as quickly as expected; does not vascularize as expected; exhibits a gritty or pigmented surface; develops a plaque, groove, or deep stromal abscess; or if the uveitis present worsens initially when topical antifungal therapy is initiated. Vascularization is usually necessary for the resolution of fungal lesions in the cornea.
■ Clinical Pathology A diagnosis of superficial fungal keratitis is made when fungal hyphae or yeast are seen on cytologic analysis or cultured from corneal scrapings (Fig. 39.14). A diagnosis with deep keratitis or a stromal abscess may require a full-thickness corneal biopsy from which the fungus is identified using culture or histopathologic evaluation. Unfortunately, some diagnoses of fungal keratitis are made only after enucleation.84 Fungal culture with susceptibility testing is recommended, but because results are often pending for prolonged periods, empirical antifungal therapy is required. Recent reports have described the use of confocal microscopy in the standing horse to confirm and assess the depth of fungal keratitis.93
■ Pathophysiology Fungal hyphae do not generally colonize intact corneas. An attachment may be initiated if
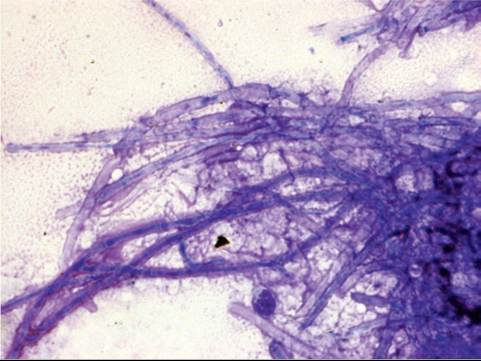
FIG. 39.14 Cytology of fungal keratitis. Diff-Quik, ?100. Note numerous basophilic septate and branching fungal hyphae. A single neutrophil serves as a reference for size of hyphae. (Image courtesy Anne Gemensky-Metzler.)
there is a disturbance in the overlying tear film, but damage to epithelium is usually necessary for pathogenic or opportunistic fungi to begin growth in the corneal stroma. This usually results from a traumatic incident that may or may not be noticed by the owner. Use of antibiotics and corticosteroids alters normal flora and decreases the normal immune response, which may encourage fungal growth.94 Fungi implicated in keratomycoses are usually present in the horse's environment and can be cultured from more than 90% of normal horse eyes, with Aspergillus spp. being the most common isolate.81,95 There is one report in the literature of keratomycosis caused by Candida albicans secondary to disseminated candidiasis.85
■ Epidemiology This disease is sporadic, with varying seasonal distribution and worldwide incidence.81-88,96
■ Treatment and Prognosis Keratomycosis in any form typically requires extended medical therapy (generally >6 weeks, sometimes considerably longer), and if stromal loss is detected, early surgical intervention is advisable. Treatment consists of eliminating the fungus from the cornea and controlling secondary bacterial invasion and melting, along with reflex uveitis, as for bacterial keratitis. Subpalpebral lavage systems are usually essential for delivering these drugs. Healing is usually not complete until corneal vascularization has reached the infected area, except when the fungus has reached Descemet's membrane; in these cases blood vessel growth does not always stop fungal growth. Medical therapy is most effective for treating superficial disease. For deep disease, surgical therapy is often necessary in combination with medical therapy. Deep lamellar and penetrating keratoplasty probably carry the best progno-
7475 8891
sis, ’’’ although superficial keratectomy with a conjunctival graft can also be used for lesions in the anterior stroma.
A number of antifungal agents are available. Miconazole, used as the undiluted IV preparation, was once the drug of choice for many ophthalmologists. Unfortunately, it is no longer available commercially in this formulation, although it can be compounded. Natamycin (Natacyn) is manufactured as an ophthalmic suspension and is the only commercially available topical ophthalmic antifungal medication approved by the U.S. Food and Drug Administration (FDA). However, natamycin does not penetrate intact epithelium well, and some Fusarium spp. may be resistant to the drug.97,98 Voriconazole administered topically in a 1% solution penetrates intact corneal epithelium and reaches therapeutic corneal concentrations; it has a relatively wide spectrum of action and is efficacious against the common fungal species.99-101 It is probably the most commonly used antifungal agent presently.
Fluconazole may be used topically or systemically and is generally regarded to have the best penetration of the bloodbrain and blood-ocular barriers among the antifungal agents. However, one study reported that fluconazole had lower in vitro activity than a number of other antifungal drugs.98 The IV preparation is a 2 mg/mL solution, which is used undiluted as a topical preparation. Miconazole and fluconazole do penetrate intact corneal epithelium when given topically, but drug concentrations in the stroma are higher if epithelium is absent.102 Fluconazole can also be used subconjunctivally, intracamerally, or intravitreally. Ophthalmologists may use fluconazole systemically to treat deep corneal fungal disease because this drug does reach adequate concentrations in the aqueous humor, which may be appropriate for deep stromal or endothelial infections.103 No toxicity studies have been performed on the horse, but anecdotal evidence does not suggest toxicities, and fluconazole has been associated with resolution of deep disease in some instances. It is not commonly used, however, because of its relatively narrow spectrum.
Compounded formulations of itraconazole/DMSO ointment have also been used for equine keratomycosis. High concentrations of itraconazole can be achieved in the corneal stroma with this preparation, even when the overlying epithelium is intact, and it has been used successfully in clinical cases.104 In contrast to fluconazole, systemically administered itraconazole does not penetrate noninflamed equine eyes.105
Other drugs have been suggested as treatment for fungal keratitis. Miconazole dermatologic or vaginal creams seem to work for mild superficial disease, but no clinical trials describing their efficacy and safety for ocular use have been reported. Amphotericin B has good antifungal properties but can be very irritating. It is useful for the rare cases in which a yeast is the offending pathogen. In vitro research shows that silver sulfadiazine is fungicidal against isolates from equine patients with keratomycosis.97 Unfortunately, in vitro results do not necessarily correlate with clinical results in patients with keratomycosis.106-108 Corneal penetration of the drug, the horse's immune system, and the site and severity of the fungal infection all play important roles in drug choice.97 The use of newer agents such as posaconazole, caspofungin, and anidulafungin is currently being explored.109-111
In addition to topical antifungal agents, therapy should proceed as with any ulcer, with topical antibiotics, antiprotease medications, and atropine, as well as systemic NSAIDs when indicated. Systemic NSAIDs should be used for the secondary uveitis, especially at the beginning of treatment when fungal death can exacerbate uveitis. However, NSAIDs slow vascularization of the cornea, and treatment with these drugs should be decreased as the uveitis is controlled.79
Prognosis is guarded to poor in many cases of fungal keratitis. Usually the best possible outcome is a visual eye with some degree of residual corneal scarring. Because no evidence suggests that corticosteroids decrease the eventual size of the scar, and because they will promote the presence of residual hyphae, their use is not recommended in a healing fungal ulcer. Complications of fungal keratitis include perforation of the ulcer with loss of the eye, superinfection with bacteria, and phthisis bulbi.
Viral Keratitis in Horses
Equine herpesvirus serotype 2 (EHV-2) and serotype 5 (EHV-5) have been isolated from eyes in herd outbreaks of keratoconjunctivitis in horses.112-116 Clinical signs in one outbreak included photophobia, epiphora and corneal neovascularization, color change, and pinpoint ulcerations; eyes healed within 2 weeks.112 In another outbreak, conjunctivitis and multifocal superficial corneal opacities were seen; eyes healed within 2 weeks on topical idoxuridine.113 Experimental inoculation of EHV-2 intranasally in two ponies pretreated with dexamethasone caused conjunctivitis, lymphadenopathy, and coughing.117 Conjunctivae from both ponies was positive for virus by PCR 6 months after inoculation. EHV-2 can also be isolated from the blood of normal horses,118 and positive PCR results can be obtained from normal eyes as well as eyes with keratoconjunctivitis, making diagnosis difficult.116 Miller and colleagues119 confirmed EHV-2 by fluorescent antibody staining after isolating virus from the cornea of a Thoroughbred mare with multiple superficial punctate corneal lesions. The keratitis was successfully treated with topical 1% trifluridine ophthalmic solution.
Acute cases may be moderately painful (blepharospasm, serous epiphora), with chemosis and conjunctival hyperemia. Recurrence is common and is often associated with corneal vascularization. The superficial or punctuate lesions (epithelial, subepithelial, or anterior stromal) of EHV may or may not retain fluorescein stain. Diagnosis may be difficult, and other differential diagnoses should be considered, including fungal keratitis and immune-mediated keratitis. Therapy for EHV keratitis includes topical antiviral and NSAID therapies. Idoxuridine (0.1%) and trifluridine (0.3%) limit viral replication but do not kill the virus; frequent dosing is required (4 to 12 times daily for 3 to 5 days until the condition stabilizes, then 3 to 6 times daily thereafter). A newer antiviral, 0.5% cidofovir, is effective in cats and requires only twice-daily dosing, but its use in horses has not been reported. Topical NSAIDs such as 0.03% flurbiprofen and 0.1% diclofenac are helpful for secondary uveitis and keratitis, but they should be used with caution because they have been reported to cause recrudescence of viral keratitis in human patients. Systemic flunixin meglumine is often helpful to improve comfort. If defects in the corneal epithelium are present, the additional use of a broad-spectrum topical antibiotic agent is indicated to prevent secondary bacterial infection.
More on the topic Infectious Ocular Diseases:
- Signs of Ocular Disease*
- Infectious Ocular Diseases
- Immune-Mediated Ocular Diseases
- Ocular Manifestations of Systemic Disease
- DISEASES
- REFERENCES
- Ocular Trauma
- Ophthalmic History and Examination
- Smith Bradford P., Van Metre David C., Pusterla Nicola (eds.). Large Animal Internal Medicine. Part 2. 6th edition. — Elsevier,2020. — 2279 p., 2020
- In Animals