Signs of Ocular Disease*
Renee T. Carter
Clinical signs of ocular disease can be grouped into five primary categories at the time of presentation:
• Ocular or periocular asymmetry
• Ocular color change
• Ocular discharge
• Ocular pain
• Visual deficits or blindness
Patients may present with one or a combination of these clinical signs.
This section provides a general description of the signs and examples of ocular diseases in which a particular sign predominates. Tables 39.1 and 39.2 summarize common signs of ocular disease in large animals.Ocular or Periocular Asymmetry
Ocular or periocular asymmetry results from unilateral changes in facial soft tissue or orbital structures, orbital volume, globe size, eyelid position, or pupil size and position (see Table 39.1). Changes in symmetry often involve a reduction or increase in volume of a certain tissue. Reduction in tissue volume occurs with congenital hypoplasia, cicatricial shrinkage, atrophy, or dehydration. Increase in tissue volume may involve the whole globe (buphthalmos) or be characterized by irregular enlargement, as seen with inflammatory or neoplastic lesions involving the globe, orbit, or eyelids. Asymmetry may also result from a neurologic dysfunction. Common examples include reduced palpebral fissure size (secondary to facial nerve paralysis), strabismus, third eyelid protrusion, and anisocoria (see Chapter 8). This section describes the common signs of ocular disease. It is not the intent to describe in detail each of the diseases that may be noted; these disorders are covered in other sections of this chapter.
Change in Globe Position
Changes in globe position affect symmetry and include exophthalmos, enophthalmos, and strabismus. Forward displacement of the eye (exophthalmos; Fig. 39.7) is often associated with a space-occupying orbital lesion (neoplasia, inflammatory,
^Contributions to previous editions by Cecil P.
Moore and David J. Maggs are acknowledged.
FIG. 39.7 Hereford with marked exophthalmos of the left eye that was present bilaterally.
vascular, cystic) or, less often, a congenitally shallow, underdeveloped orbit. Posterior malposition of the globe (enophthalmos) may result from active globe retraction caused by pain or from loss of supporting retrobulbar soft tissues as seen in cases of muscle atrophy, loss of orbital fat, or denervation. Congenital strabismus is a developmental abnormality that results in ocular asymmetry due to deviation of normal globe position and has been reported in Jersey, Shorthorn, Holstein, and German Brown Swiss cattle.1,2 Strabismus can occur with exophthalmos and has also been associated with systemic disorders such as polioencephalomalacia and listeriosis.2 Unequal orbit volume resulting in displacement of the globe or globe malposition may also occur with traumatic orbital fractures.
Change in Globe Size
Unequal globe size can also account for ocular asymmetry. A congenitally small globe (microphthalmia) occurs as a genetic defect in sheep, cattle, and horses1,3,4 and has also been associated with exposure to infectious agents and teratogens. Microphthalmia is frequently accompanied by multiple ocular anomalies and may be associated with multiple organ involvement or vertebral abnormalities.2 Acquired variations in globe size usually result from shrinkage of the globe secondary to globe rupture or with phthisis bulbi (Color Plate 39.11) secondary to chronic uveitis; stretching or enlargement of the globe (megaloglobus, buphthalmos) occurs with glaucoma. Cornea globosa has been reported in horses and ponies with multiple congenital ocular anomalies (MCOA) syndrome with the silver mutation and coat color.5,6
Changes in Eyelid Conformation
Asymmetry of the upper or lower eyelid may be due to entropion, ectropion, blepharitis, conjunctivitis, or ptosis (facial nerve paralysis or sympathetic denervation).
Entropion has been reported in Simmentals1 and as an inherited trait in sheep.7 (see Color Plate 39.3) However, entropion most commonly occurs secondary to microphthalmos or enophthalmos (retraction of the eye with pain, reduction in orbital volume, denervation). Trauma with secondary scar formation may result in either entropion or ectropion. Nictitating membrane (third■ TABLE 39.1
Causes of Important Ocular Signs in Large Animals
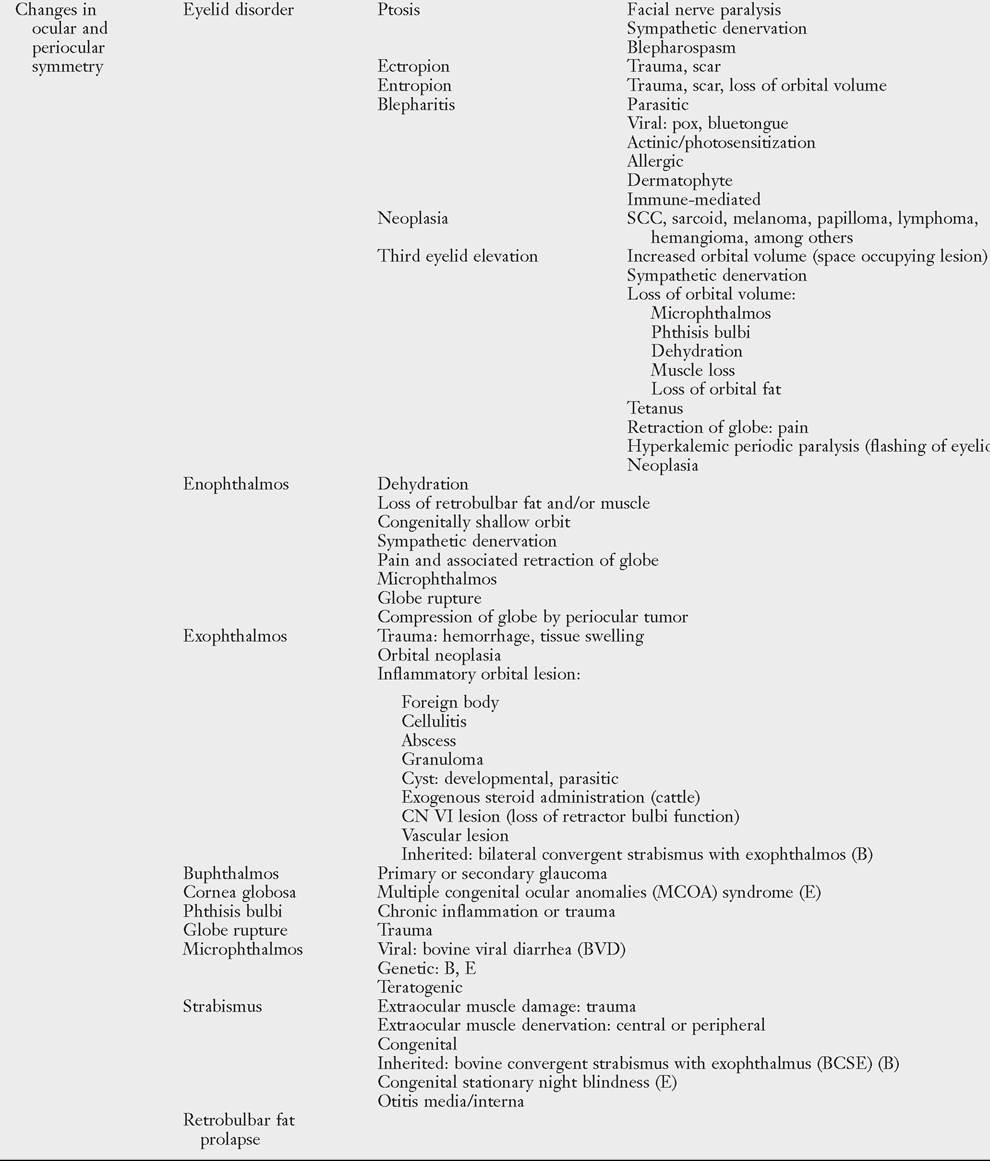
■ TABLE 39.1
B, Bovine; CN, cranial nerve; E, equine; SCC, squamous cell carcinoma.
Data from Gosselin VB, Francoz D, Babkine M, et al.: A retrospective study of 29 cases of otitis media/interna in dairy calves. Can Vet J 53:957-962, 2012; and Estell K: Periocular neoplasia in the horse. Vet Clin Equine 33:551-562, 2017.
■ TABLE 39.2
Differential Diagnoses for Ocular Signs in Large Animals
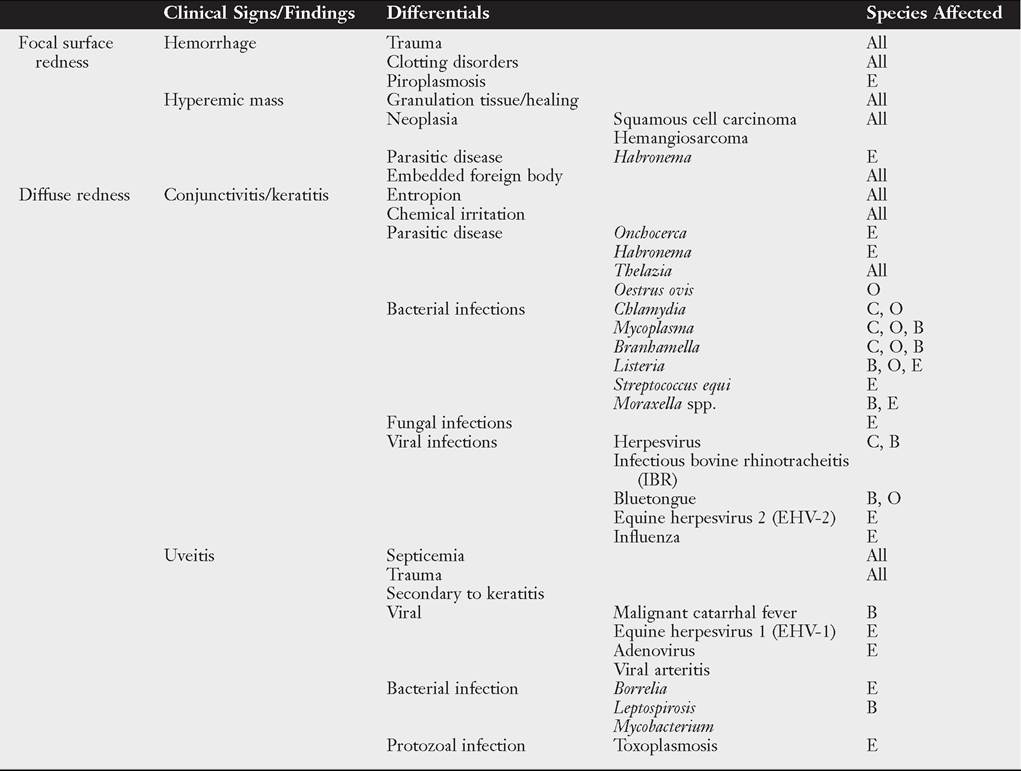
■ TABLE 39.2
Differential Diagnoses for Ocular Signs in Large Animals—cont'd
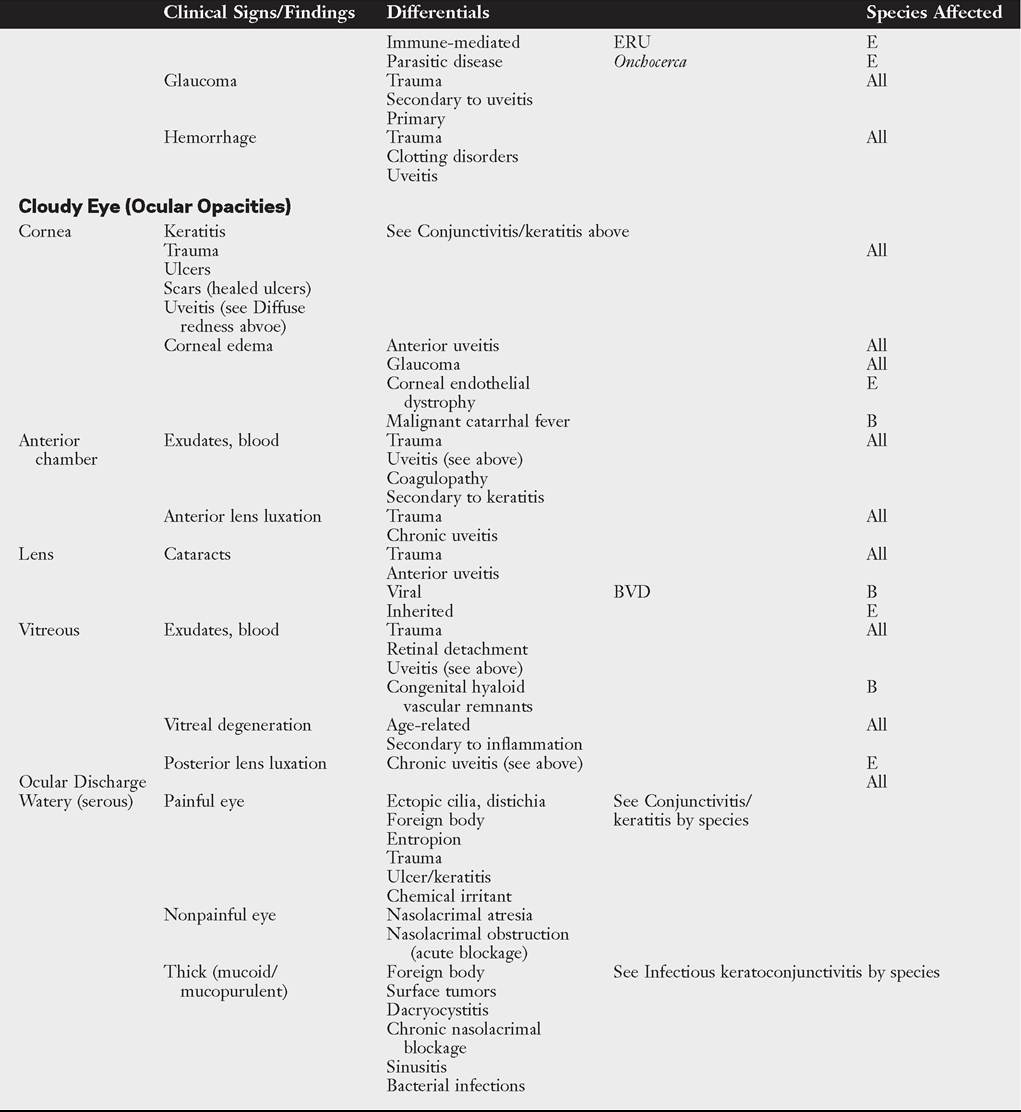
B, Bovine; BVD, bovine viral diarrhea; C, caprine; E, equine; ERU, equine recurrent uveitis; O, ovine.
eyelid) protrusion is frequently seen secondary to active retraction of the globe in response to ocular pain, enophthalmos caused by loss of orbital contents (dehydration, malnutrition, atrophy), presence of third eyelid masses, orbital spaceoccupying masses, or neurologic disorders (e.g., Horner’s syndrome, tetanus).
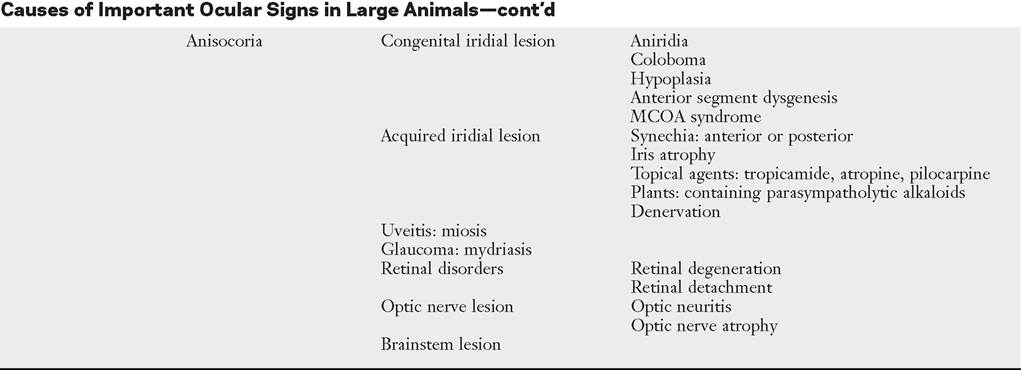
Anisocoria
Pupillary asymmetry, or anisocoria, may develop for a variety of reasons that can be grouped into (1) primary iridal lesions, including congenital iridal defects (hypoplasia, aniridia, coloboma, anterior segment dysgenesis, synechia, iris atrophy), (2) neurologic disorders (Horner’s syndrome, oculomotor nerve dysfunction), (3) intraocular diseases (uveitis, glaucoma, unilateral retinal lesions), (4) diseases involving the optic nerve or brainstem, and (5) previous use of pharmacologic agents such as atropine that alter iris sphincter muscle function or exposure to plants containing parasympatholytic alkaloids.
Changes in Tissue Volume
The presence of an ocular mass may be the primary cause of ocular asymmetry. Ocular surface neoplasms are relatively common in horses and cattle. Ocular squamous cell carcinomas usually arise from nonpigmented tissues of the nictitating membrane, the lateral limbal region, or the eyelid margin where ultraviolet (UV) light exposure is highest.8 They may appear as irregularly raised, papillary surface masses or, less often, as smooth, vascularized lesions that invade the globe (Color Plates 39.12 and 39.13). Ulceration, exudation, and mucopurulent ocular discharge are frequent concurrent findings (see the Ocular Neoplasia section later). Periocular sarcoids are also common in horses; their appearance is variable, ranging from flat foci of alopecia to fleshy or nodular nonulcerative lesions.9,10 Other ocular tumors occur in large domestic animals but are relatively uncommon. Dermoids and orbital cysts are congenital masses involving the periocular tissues, eye, or orbit. Other nonneoplastic ocular masses seen in large animals include firm parasitic and foreign body granulomas and soft, fluctuant subconjunctival swelling characteristic of prolapsed periorbital fat. Ocular and orbital pseudotumors have also been described in the horse.11
Ocular Color Change
Changes in the color of ocular or periocular tissues or the presence of opacities in the clear ocular media (cornea, aqueous humor, lens, or vitreous) are important features of ocular disease. Such changes must be differentiated from normal congenital differences in ocular pigmentation. Developmental color dilution or absence of ocular pigmentation results in light or multicolored irides (heterochromia iridis). Examples of abnormal coloration include hyperemia of conjunctival (superficial) or episcleral (deep) blood vessels associated with ocular inflammation (see Table 39.2), hemorrhage secondary to trauma or coagulopathies, pallor of the conjunctiva (which reflects severe anemia), and yellowing of the sclera and sometimes iris, indicating icterus.
A change in the color of the iris may also occur with anterior uveitis.Opacities of the ocular media may occur as either surface (corneal) or intraocular (anterior chamber, lens, or vitreous) phenomena. Brown discolorations of the cornea are the result of pigmentation, iris prolapse, embedded foreign body, or pigmented fungal plaques. Grayish scars occur from previous episodes of keratitis; infectious keratitis will present with cream- to white-colored infiltrate; corneal degeneration will appear as white deposits of lipid or mineral; vascularization occurs secondary to chronic inflammation or neoplasia; and bluish discoloration is caused by corneal edema. These color changes frequently occur in various combinations in more severe keratitis, especially those of infectious origin such as chronic keratoconjunctivitis caused by Chlamydia spp., Mycoplasma spp., or Moraxella bovis. Cataracts are perhaps the most obvious cause of intraocular opacities in large animals (Color Plate 39.14). Inherited cataracts have been reported in Thoroughbreds, Quarter Horses, Morgans, and Rocky Mountain horses.12 However, the presence of exudates within the aqueous humor or vitreous, congenital vascular remnants in the vitreous, degeneration of the vitreous, or retinal detachment may also account for intraocular opacities (see Table 39.2).
Ocular Discharge
Ocular discharge can be characterized as serous, mucoid, purulent, or hemorrhagic. The type of discharge may assist in determining the severity and chronicity of the eye disease. Serous discharge generally indicates mild eye disease, whereas mucopurulent or hemorrhagic discharge indicates more serious disorders. A notable exception to this generalization is equine recurrent uveitis (ERU), which is associated with serous discharge (see the Immune-Mediated Ocular Diseases section later). The nature of ocular discharge tends to change as the disease progresses or improves. This is most notable in inflammatory or infectious ocular diseases.
Initially the discharge is predominantly serous, but it tends to become mucopurulent with chronicity (see Table 39.2).Epiphora describes facial wetting and results from overflow of tears over the eyelid margin. This may result from excessive secretion of tears (e.g., painful stimulus) or from physical or functional obstruction of the nasolacrimal system. In large animals, reflex lacrimation with an associated overabundance of tears is the typical response to ocular irritation or inflammation (e.g., foreign body, lash disorders, conjunctivitis, keratitis, uveitis). When epiphora is noted, careful digital and visual examination for foreign bodies within the conjunctival fornix or under the third eyelid is indicated. Epiphora is generally one of the earliest signs of conjunctivitis, ulcerative keratitis, or anterior uveitis. In cattle with keratoconjunctivitis caused by Moraxella bovis, epiphora is present several days before visible corneal ulceration occurs13 (see the Infectious Bovine Keratoconjunctivitis [IBK] section later).
If signs of painful stimuli are not noted, the patency of the nasolacrimal system should be evaluated. Developmental defects or malformations of the nasolacrimal duct system (e.g., imperforate puncta) result in epiphora secondary to impaired outflow in neonates. In these cases, the presence of epiphora may be misinterpreted as overproduction of tears. Previously undiagnosed congenital defects may also be the cause of persistent ocular discharge in adult animals. Acquired obstructions of the nasolacrimal ducts may result from infections, foreign bodies, facial trauma, nasal tumors, or sinusitis that involve the duct system. Whether congenital or acquired, simple nonseptic obstructions are characterized by epiphora; septic occlusions result in mucopurulent discharge from the eye or nostril on the affected side. Excessive mucus production is a feature of follicular conjunctivitis, possibly as a result of the rubbing of elevated lymphoid follicles on apposing conjunctival surfaces. Lymphoid follicles are noted in subacute or chronic forms of chlamydial conjunctivitis in sheep and with Onchocerca larval migration in horses. Mucoid ocular discharge may be observed concurrently with epiphora in acute ocular surface infections caused by viral or chlamydial agents. Excessive tenacious mucus may also result from inadequate secretion of the aqueous component of tears (i.e., keratoconjunctivitis sicca). Although keratoconjunctivitis sicca (KCS) is not diagnosed as commonly in large animals as it is in dogs, neurogenic KCS due to loss of parasympathetic innervation has been reported in horses, usually as a complication of guttural pouch pathology.14 KCS has also been reported with locoweed poisoning and hypothyroidism.15
Purulent to mucopurulent material is characteristic when bacterial organisms are involved in the ocular disease process. Bacterial conjunctivitis occurs frequently in large domestic species and manifests as red eyes with copious mucopurulent ocular exudate. Ocular foreign bodies and surface masses (e.g., squamous cell carcinoma) may predispose to secondary bacterial infections. Mucopurulent discharge in the absence of ocular inflammation suggests infection of the nasolacrimal sac (dacryocystitis) or ducts, with reflux of exudate from the lacrimal puncta.
Sanguineous or hemorrhagic discharge most often occurs after blunt or penetrating trauma to the eye (see the Ocular Trauma section later). Foreign body penetration may damage the eyelid, conjunctiva, or globe, resulting in bleeding onto the ocular surface. In addition, bloody-tinged ocular discharge has been reported in equine piroplasmosis.16 Corneal ulcers may rupture and result in uveal prolapse and subsequent hemorrhage on the ocular surface. Patients with conjunctivitis or ocular surface tumors may develop ulceration resulting in bloody ocular discharge. Whenever blood is noted on the surface of the eye, it is imperative that a thorough ophthalmic examination be performed to determine the cause and evaluate integrity of the globe.
Ocular Pain
Ocular pain can be manifested as blepharospasm, epiphora, photophobia, and periocular hyperesthesia. Animals with severe ocular pain usually resist manipulation of the eyelids or any form of ocular examination by persistently jerking the head away from the examiner and closing the eyelids tightly. In cases of persistent ocular inflammation, discomfort and pruritus may be manifested by rubbing and self-trauma to ocular or periocular structures.
Ocular pain may result from conjunctivitis, trauma, keratitis, uveitis, and glaucoma. Other causes of ocular pain include mechanical irritation from entropion, trichiasis, distichia, ectopic cilia, or foreign material.17 Foreign bodies that cause ocular irritation in large animals are typically plant materials like seeds, hay stems, straw, twigs, bark, or thorns, although particles of sand or soil can also cause severe ocular irritation. Nonembedded particulate matter is usually entrapped by mucus and washed out of the eye by reflex tearing; it typically results only in transient discomfort. By contrast, embedded foreign material (i.e., between ocular surface layers or within ocular tissues) causes persistent ocular pain.
Blindness
Visual deficits in large animals manifest in a variety of ways. Obvious signs include bumping into objects and lack of response to visual stimuli such as light or hand motions. Another sign of blindness is reliance on stationary objects (e.g., fences, railings, other animals) to maneuver within the environment. Behavioral changes include reluctance to move or to venture into unfamiliar areas, nervousness, and spooking in response to sudden noises or movements.18 The nonvisual animal is frequently found standing isolated from the group and may experience injury by dominant individuals in the herd and suffer from weight loss.18 Searching nystagmus is also seen in some animals with congenital blindness.
Nonvisual animals attempt to compensate for loss of vision with their other senses, which may result in an elevated head position or a head tilt. Patients may also exhibit maximum neck extension or snorting or intensive sniffing associated with nervousness. Frequently, blind animals will show exaggerated elevation of the limbs while walking. This must be differentiated from true hypermetria (see Chapter 8). Partial loss of vision may be difficult to determine, and detection depends on observing more subtle behavioral changes such as slight head cocking or tilting, difficulty maneuvering in dim light, or shying and startling from objects on one side or objects present in some specific part of the visual field. Conduction of a maze test will assist the clinician in the detection of partial vision loss. Animals may effectively compensate for congenital blindness or slow diminution of vision, particularly when they remain with other unaffected animals in a familiar environment. Visual disturbance may not be apparent until an affected animal is isolated or moved to an unfamiliar area.
There are numerous causes of blindness in large animals, including those that involve only the visual system and some that involve other nervous system tissues or are multisystemic (Box 39.1). A functional approach to blindness involves anatomically classifying the cause as one of the following:
• Cloudy ocular media (light does not reach the retina)
• Retinal detachment or retinopathy
• Optic nerve or central nervous system (CNS) disorder
■ BOX 39.1
Guidelines for Inspection (Antemortem and Carcass) and Disposal of Animals, Carcasses, and Parts Affected With Neoplasia
A. Epithelioma of the Eye
1. Any animal found on antemortem inspection to be affected and the eye has been destroyed or obscured by neoplastic tissue and which shows extensive infection, suppuration, and necrosis, usually accompanied by foul odor, or any affected animal with cachexia, regardless of extent, shall be condemned.
2. Carcasses of animals with the eye or orbital region affected will be condemned if the affection has:
a. Involved the osseous structures of the head with extensive infection, suppuration, and necrosis;
b. Metastasized from the eye or orbital region to any lymph node (including the parotid lymph node), internal organs, muscles, skeleton, or other structure, regardless of the extent of the primary tumor; or
c. Regardless of extent is associated with cachexia or evidence of absorption or secondary changes.
3. Carcasses of animals affected to a lesser degree than above may be passed for human food after removal and condemnation of the head, including the tongue, provided the carcass is otherwise normal.
B. Neoplasms
1. An individual organ or other part of a carcass affected with a neoplasm shall be condemned. If there is evidence of metastasis or that the general condition of the animal has been adversely affected by the size, position, or nature of the neoplasm, the entire carcass shall be condemned.
2. Carcasses affected with malignant lymphoma shall be condemned.
From Code of Federal Regulations, Title 9, Chapter 3, Parts 309.6, 311.11, and 311.12 (1-1-87 edition).
Assessment of PLRs aids in localization of the lesion. Cloudy ocular media can be identified on retroillumination. Animals with lesions involving the retina, optic nerve, optic chiasm, or optic tracts generally do not have a normal PLR, whereas those with more central (“higher”) lesions involving the lateral geniculate bodies, optic radiations, or occipital (visual) cortex are likely to exhibit a normal PLR (see Chapter 8).