Pericarditis
Definition and Etiology
Pericarditis is inflammation of the pericardium that results in accumulation of fluid or exudate between the visceral and parietal pericardium. Pericarditis in large animals occurs with trauma from penetration of ingested foreign objects or external wounds, hematogenous spread (septicemia) of infection, extension of infection from the lung or pleura, viral infections such as equine viral arteritis or equine influenza, and neoplasia.
Pericarditis has also been associated with the mare reproductive loss syndrome (MRLS), with Actinobacillus species isolated in the majority of these horses.209 * * * Idiopathic pericarditis, characterized by an aseptic inflammatory exudate, is not uncommon in horses and has recently been reported in cattle.210-217 Autoimmune, hereditary, and metabolic causes of pericarditis have not been documented in large animals.Clinical Signs and Differential Diagnosis
The clinical presentation of pericarditis can vary depending on the volume and rate of development of the pericardial effusion and the cause. Nonspecific clinical signs—fever, anorexia, depression, or weight loss—may be the chief complaints, but more frequently, peripheral edema, jugular venous distention and pulsations, tachypnea, or dyspnea is the presenting clinical sign. Cattle may exhibit pain by an abnormal stance characterized by abducted elbows, a spontaneous or induced expiratory grunt, reluctance to move, or preference to stand with the forequarters elevated. Horses may show signs of colic or syncopal episodes.
The most consistent findings on auscultation are tachycardia, muffling of heart sounds, and absence of lung sounds in the ventral thorax. Dorsally the lung sounds are louder than normal. These findings are in contrast to pleuritis, an important diagnostic rule-out for pericarditis, in which lung sounds are muffled ventrally but heart sounds are not, and radiation of the heart sounds occurs over a wider area than normal.218 In cattle, splashing sounds are frequently audible in the cardiac auscultation area, a sound some refer to as a “washing machine murmur or rub.” This is attributed to accumulation of gas and fluid in the pericardium and is indicative of the presence of gas-forming (anaerobic) organisms and a grave prognosis.
In cattle this murmur distinguishes pericarditis from cardiac neoplasia or other causes of CHF. The splashing sounds are absent in horses and muffled heart sounds are the rule, but pericardial friction rubs may be auscultated, especially after pericardial fluid accumulation has been relieved.213 A gallop rhythm may be auscultated in either horses or cattle.Mucous membranes may be congested and have a prolonged capillary refill time. Jugular venous distention and pulsations are usually present. Arterial pulses are weak. The latter findings may help distinguish pericarditis from primary pleuritis. Percussion of the thorax reveals ventral dullness, and pleural effusion is frequently present in horses with pericarditis. A concurrent pleuropneumonia or septic pleuritis is present in some horses.215,219-222 Ascites is infrequently detected in horses with pericarditis, but concurrent peritonitis has been reported.223
Clinical Pathology
CBC changes are nonspecific and depend on the cause of the pericarditis. There may be hemoconcentration if the animal is dehydrated or toxemic, or there may be a mild anemia associated with chronic infectious pericarditis. WBC count may be normal or increased. There may be an absolute neutrophilia or a lymphopenia. Frequently the fibrinogen concentration or SAA is elevated. Serum chemistries are usually normal except for albumin concentration, which may be low212,213 and accompanied by an elevation in globulin concentration. Liver enzyme, bilirubin, serum urea nitrogen, and creatinine concentrations are frequently mildly elevated, consistent with the development of CHF. Laboratory evidence of dehydration (increased PCV, total protein, serum urea nitrogen, and creatinine concentrations) may be exaggerated when diuretics have been administered previously. Although total serum LDH concentration may be elevated, more specific information may come from finding an increase in the cTnI or the myocardial isoenzymes CK and LDH.
An elevated cTnI was reported in one cow with hemorrhagic pericarditis.216 Electrolyte concentrations are frequently normal, but serum calcium and potassium concentrations may be low because of anorexia. Decreased sodium and chloride concentrations have been reported in horses with pericarditis.213 No consistent abnormalities in arterial or venous blood gas concentrations have been reported in large animals with pericarditis.Radiography is not a sensitive diagnostic test for pericarditis in horses, although an enlarged rounded cardiac silhouette is detected with large pericardial effusions. In cattle, traumatic pericarditis frequently results in fluid and gas accumulation in the pericardium that is detectable radiographically and relatively specific for this disease. A metallic foreign body is usually detected radiographically in the cranial reticulum or caudal thorax in cattle with traumatic pericarditis (Fig. 30.18). Radiographic changes may not be detected in early or uncomplicated pericarditis. If fluid accumulation is large and there is concurrent pleural effusion, changes are indistinguishable from those associated with pleuritis. An enlarged, rounded cardiac silhouette is not specific for pericarditis and is seen with other causes of generalized cardiomegaly. An obscured cardiac silhouette, vena cava, and diaphragm, with dorsal displacement of the trachea, may be seen with pericarditis or pleuritis. The lungs, which may be aerated only dorsally, frequently have interstitial infiltrates.
The ECG changes most commonly associated with pericarditis in large animals are decreased amplitude of the QRS complexes (3.5 g/dL) and an elevated WBC count (>2500∕μL) composed primarily of neutrophils. The fluid is urine colored to slightly blood tinged and foamy’ and it has a foul odor. A mixed population of gram-positive and gramnegative aerobic and anaerobic bacteria (GI flora) are usually present. Protozoa may be found in unusual circumstances.
Hemorrhagic effusion has been reported in several cows with idiopathic pericarditis that responded favorably to pericardial drainage (usually with lavage) along with systemic antimicrobial therapy.216 In horses, protein concentration of the pericardial fluid is elevated (≥2.5 g/dL) and the WBC count is normal or elevated with a population predominantly of neutrophils, although red blood cells, lymphocytes, eosinophils, mesothelial cells, and histiocytes have been observed.212-214,219,223 Bacterial (aerobic and anaerobic) cultures and viral cultures may be negative. Actinobacillus organisms were frequently isolated from mares with pericarditis in association with the MRLS.209 Paired serum may support a viral cause. Analysis of pleural and peritoneal fluid (when present) usually reveals fluid characterized as a modified transudate or as mildly inflammatory.
FIG. 30.24 Insertion of a pericardial chest tube into the left fifth intercostal space for drainage and lavage of the pericardial space. Note that the left foreleg is being pulled forward, the clinician is inserting the large-bore Argyle chest tube into the left fifth intercostal space above the lateral thoracic vein, and the cow is wearing a radiotelemetry electrocardiogram system underneath the surcingle.
Cardiac catheterization demonstrates an elevation in central venous or right atrial pressure, and the atrial and ventricular pressure curve may be abnormal in appearance. Right atrial, right ventricular, and pulmonary artery end-diastolic pressures may equilibrate.224 In combination, these findings are relatively specific for pericarditis.
Pathophysiology
Accumulation of fluid in the pericardium occurs as a result of inflammation. The rate of fluid accumulation and the degree to which the pericardial pressure increases determine the pathophysiologic consequences.
Generally pericarditis results in decreased distensibility (increased ventricular end-diastolic pressure) of the heart, which impairs the ability of the heart to fill during diastole. The elevation in end-diastolic pressure and impairment of ventricular filling elevate atrial pressure and reduce venous flow or venous return to the heart and diastolic perfusion of the myocardium. The result is a depression of ventricular contractility, stroke volume, and consequently cardiac output. In addition, arterial pressure and renal blood flow are decreased. Initially, compensatory mechanisms consisting of vasoconstriction, increased heart rate, and sodium retention (increased vascular volume) may maintain cardiac output. Failure to maintain cardiac output results in circulatory collapse.Pericarditis can be classified as primarily effusive, constrictive, or a combination of both.224 The hemodynamic consequences of effusive pericarditis are primarily caused by the physical presence of pericardial fluid, whereas constrictive pericarditis is classified as such, because the reduction in ventricular compliance is due to fibrinous or fibrotic involvement of the pericardium and epicardium. Removal of pericardial fluid results in improved cardiac performance in effusive pericarditis but is of limited usefulness in constrictive pericarditis.
Epidemiology
Pericarditis is uncommon in horses; when it does occur, it is most frequently idiopathic and can occur in a horse of any age. History of a recent respiratory tract infection is not uncommon. Exposure of horses to Eastern tent caterpillars was the greatest risk factor for the development of fibrinous pericarditis during the MRLS epidemic.227 Traumatic pericarditis has been reported in horses but is rare.228 Iraumatic pericarditis is not uncommon in cattle, but it occurs in less than 10% of cattle with traumatic reticuloperitonitis.75 Most cattle are affected in late gestation or at parturition.
Idiopathic pericarditis is rare in cattle. Cattle with idiopathic hemorrhagic pericarditis may eventually develop cardiac lymphosarcoma.210Necropsy Findings
Gross postmortem examination shows distention of the pericardial sac with serosanguineous or urine-colored fluid that is foamy and may be malodorous (cattle). There may be organization of fibrinous exudate and fibrosis that is also evident on the epicardium (Fig. 30.25) and may infiltrate the myocardium. Pleural effusion may be present. Other signs of CHF such as pulmonary congestion, pulmonary edema, and chronic passive congestion of the liver may be present. If the cause is traumatic, the offending object may be well contained in a fibrous tract located between the reticulum and the pericardium.
Histopathologic examination reveals pericardial, epicardial, and occasionally myocardial fibrosis and inflammation with neutrophilic, lymphocytic, eosinophilic, or plasma cell infiltrates. Bacteria may be visible. The liver may show diffuse centrilobular necrosis, fatty change, dilation and congestion of sinusoids, and perivenous fibrosis.
Treatment and Prognosis
Treatment of traumatic pericarditis in cattle is generally unrewarding and is usually addressed toward salvage or shortterm survival to calving. Repeated pericardial drainage by means of pericardiocentesis or a fifth rib resection, lavage, or peri- cardiectomy may be useful for short-term survival, but the prognosis for return to normal function is poor because CHF results from involvement of not only the pericardium but also the epicardium and myocardium (see Fig. 30.25). Thoracotomy by a split-rib technique followed by pericardiectomy has been effective in treating some cattle with traumatic, restrictive pericarditis.229
Treatment of pericarditis not caused by trauma has been successful in horses, but the initial prognosis should be guarded. Aggressive treatment of horses with moderate to large pericardial effusions should include the placement of a large-bore indwelling chest tube into the pericardial sac under echocardiographic guidance and drainage and lavage of the pericardial sac, with local infusion of antibiotics in addition to the initial broad-spectrum antimicrobial therapy. Obtaining a sample for cytologic examination and culture and sensitivity testing via a pericardiocentesis should be postponed until an indwelling catheter can be safely inserted, if pericardial drainage and lavage is considered as a probable treatment, because it is difficult to insert the catheter once the pericardiocentesis has been performed. The pericardial drainage and lavage, performed once or twice daily as needed, has been effective in treating idiopathic or septic pericarditis in horses.,,,9, Ihe indwelling tube should remain in situ until the fluid recovered at the time of drainage is consistently less than or equal to the volume instilled in the pericardial sac with antimicrobials 12 to 24 hours earlier. The ECG should be monitored because occasionally cardiac arrhythmias occur during the therapeutic procedure or during a routine pericardiocentesis. All horses with pericarditis should initially be treated for septic pericarditis with systemic broadspectrum bactericidal antimicrobial drugs. The antimicrobial choice should be based on the most likely causative agents and modified as needed by the results of culture and sensitivity testing. Fibrinous pericarditis has been successfully treated in horses with broad-spectrum bactericidal antimicrobials when the amount of pericardial fluid detected echocardiographically was too small to safely obtain a sample for cytologic evaluation and culture and sensitivity testing. Treatment of idiopathic pericarditis with corticosteroids should be initiated only after the results of these diagnostic studies demonstrate no evidence of sepsis. Pericardiotomy or (preferably) pericardiectomy are
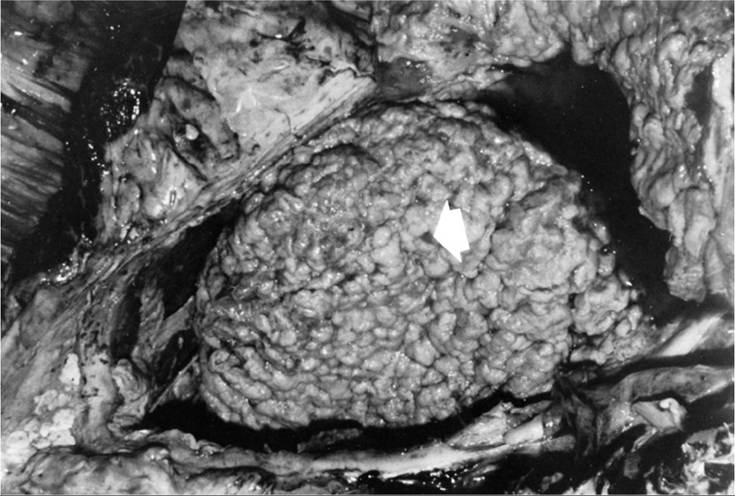
FIG. 30.25 Postmortem photograph of a cow with constrictive pericarditis. The pericardium is opened and reflected, revealing the epicardium (arrow) covered in Abrinopurulent exudate.
the treatments of choice if signs of constrictive pericarditis are present. However, the long-term prognosis for large animals after this surgery is guarded. A partial pericardiectomy was performed in one horse with constrictive pericarditis but was only transiently successful.
In traumatic pericarditis the antibiotic selected must be capable of covering gram-positive and gram-negative aerobic and anaerobic bacteria. Nonsteroidal antiinflammatory drugs (NSAIDs) have been deemed useful as adjunctive therapy, as have corticosteroids if bacterial culture of the fluid is negative and no evidence of sepsis is detected cytologically.
Although diuretics are effective in eliminating the severity of peripheral edema, they further reduce venous return and preload in animals with pericarditis. The result is further compromise of cardiac output and worsening of heart failure.
Prevention and Control
Traumatic pericarditis in cattle can be prevented by routine administration of magnets to heifers at the time of pregnancy diagnosis. At each subsequent pregnancy diagnosis, the cow should be checked for the presence of the magnet in the reticulum. It is not beneficial to have more than one magnet present at one time.
Horses should not be grazed on pastures containing trees infected with Eastern tent caterpillars. Removal of black cherry trees from equine pastures removes the preferred host tree for the Eastern tent caterpillar. Some types of infectious pericarditis in horses may be controlled by routine vaccination against the common respiratory pathogens.
Cardiac Tumors carcinomas, especially squamous cell carcinomas in horses, may involve structures adjacent to the heart and may extend to the heart or heart base, producing signs of heart disease.230,231 An infiltrative cardiac lipoma has been reported in a horse, but no signs of cardiac disease were attributed to it.232 A metastatic anaplastic pulmonary carcinoma caused signs of CHF in one horse,231 and disseminated hemangiosarcoma with myocardial involvement was thought to be responsible for VA in another horse.233 Primary pericardial hemangiosarcomas have also been reported in a horse.234
Clinical Signs and Differential Diagnosis
The clinical signs of cardiac neoplasia are nonspecific and depend on the cardiac site involved and other sites of tumor manifestation. Nonspecific signs of neoplasia are common and include anorexia, depression, weight loss, and fever. These signs can be produced by any site of chronic disease, and in large animals, pneumonia, peritonitis, enteritis, and liver and kidney disease are considered differential diagnoses, among others. If the tumor involves the pericardium, signs of pericarditis or pericardial effusion such as tachycardia, pain, jugular venous distention, peripheral edema, and weak arterial pulses may be seen. Myocardial involvement, as is most common with lymphosarcoma, may result in cardiac signs that include tachycardia, cardiac arrhythmias, and cardiac murmur (atrioventricular valve insufficiency) or signs of CHF such as peripheral edema, ascites, and diarrhea. Clinical signs attributable to tumor involvement of the endocardium (e.g., obliteration of a cardiac chamber, valvular obstruction or damage, embolic showering) are rare in large animals.
Tumor involvement of other organ systems and tissues can be manifested by lymphadenopathy, peripheral edema, diarrhea, melena, dysphagia, tachypnea, pleural effusion, or rectal palpation of abdominal masses.
Clinical Pathology
Cardiac tumors present no consistent clinicopathologic feature. The CBC from horses or cattle with lymphosarcoma may reveal neoplastic lymphocytes. The absence of leukemic changes does not rule out lymphosarcoma. Cattle with lymphosarcoma may test positive for fecal occult blood. A serum chemistry profile may reveal nonspecific changes, such as hypoalbumin- emia, hyperglobulinemia, or elevated liver enzyme concentrations, depending on the other organ systems affected by the tumor or the animal's debilitation. Diagnosis of the cardiac tumor is based on histopathology of tumor tissue. Tumor cells may be found in pericardial or pleural fluid or adjacent lymph nodes. Serologic evidence (agar gel immunodiffusion or radioimmunoassay) of BLV infection does not confirm a diagnosis of lymphosarcoma, but a negative test result virtually rules out the adult or enzootic form of lymphosarcoma in cattle. No evidence of BLV infection is found in cattle with the thymic form of lymphosarcoma.
If electrocardiographic evidence of cardiac tumors is present, it is nonspecific. Cardiac tumors may produce cardiac arrhythmias, reduce amplitude of the QRS complexes, or alter the normal appearance of the P, QRS, and T complexes. Twodimensional echocardiography or an ultrasound examination of the lungs or pleura may show evidence of the cardiac tumor by providing direct evidence of echogenic masses involving the heart or surrounding tissue, abnormal fluid accumulation, or myocardial functional changes. Ultrasound findings can determine whether any masses can be safely biopsied to confirm the diagnosis.
Radiographs may provide evidence of cardiac tumors by showing abnormal soft tissue densities in the thorax that obscure the cardiac silhouette or ventral lung borders.
Pathophysiology
Lymphosarcoma, the most common cause of cardiac tumors in cattle, has a predilection for the right atrial myocardium. Right ventricular myocardial involvement is not uncommon; left atrial or left ventricular involvement is rarer. Involvement of the right side of the heart may result in little or no evidence of heart disease. More commonly, the myocardial involvement results in dilation of the chamber involved. As a consequence, the tricuspid valve ring may be dilated, and TR occurs. Chamber enlargement or infiltration of the myocardial conduction system may cause cardiac arrhythmias. Myocardial function may be impaired so that signs of right-sided heart failure become apparent, including tachycardia, peripheral edema, jugular venous distention or pulsations, pericardial or pleural effusion, hepatic congestion, and ascites.
Epidemiology
Cardiac tumors are rare in large animals. The most common cause in cattle is lymphosarcoma. Although more than 50% of cattle in some parts of the United States are infected with BLV, only 1% to 5% develop lymphosarcoma.235-237 In herds with more than 50% of cattle infected with BLV, the incidence of lymphosarcoma may be higher. Cardiac involvement is common in cattle with the adult or enzootic form of BLV, a disease that occurs most commonly in cattle older than 4 years old.238 Thymic lymphosarcoma, which is not associated with BLV infection, also involves the heart but is much less common, occurring in cattle younger than 30 months of age.
Lymphosarcoma, mesothelioma, and squamous cell carcinoma are probably the most common causes of neoplastic involvement of the equine heart, but the prevalence is not documented.
Necropsy Findings
Necropsy findings depend on the type of cardiac tumor. Direct involvement of the myocardium with lymphosarcoma is associated with finding diffuse infiltration by a pale, tan, homogeneous tissue that frequently causes enlargement of the cardiac chamber. Involvement of the right atrium (Fig. 30.26) is the most common manifestation of adult enzootic BLV, but any area of the myocardium and pericardium may be involved. Intracavitary extension of the tumor may be evident (see Fig. 30.26). Histologic evaluation of the tumor shows diffuse infiltrates of lymphoblastic cells that obliterate the normal architecture of the myocardium.
Other tumors, such as fibrosarcoma, squamous cell carcinoma, pulmonary carcinoma, thymic lymphosarcoma, mesothelioma, and melanoma, may involve the heart by extension or metastasis from other sites in the thorax.

FIG. 30.26 Postmortem photograph of a cow with lymphosarcoma demonstrating right atrial myocardial infiltration by a tumor and extension of the tumor into the atrial lumen.
Treatment and Prognosis
No definitive treatment exists for cardiac neoplasias, and the prognosis for survival is poor. Death is expected within 6 months with most cardiac tumors. Lymphosarcoma of the heart in cattle has a grave prognosis and is usually associated with death within a few months. Short-term improvement has been achieved in cattle with lymphosarcoma treated with a combination of corticosteroids, L-asparaginase, and cytotoxin. Thoracoscopic pericardiotomy has been used as a palliative treatment in a cow with pericardial lymphoma.
Prevention and Control
Prevention and control of BLV can be accomplished by isolation of BLV-positive and BLV-negative animals; use of individual or sterilized supplies, such as needles, rectal examination sleeves, tattooing, dehorning, and ear-tagging equipment on each animal; rigorous attention to a vector control program; and feeding colostrum from serologically negative cows only.236,240 Frequent testing (at least every 6 months) and isolation of serologically positive animals over 6 months of age should be performed. Prevention and control of other cardiac tumors are not possible.