Vascular Disease: Aneurysms, Thrombosis, and Embolism
thrombophlebitis, omphalophlebitis, and parasitic arteritis. Aortoiliac thromboembolism has been reported as a complication of valvular endocarditis in a calf and mural endocarditis in a cow.249,250
Clinical Signs and Differential Diagnosis
palpable femoral arterial pulse.
Saphenous vein filling is slow or nonexistent in affected horses, and the metatarsal and other peripheral arterial pulses of the hindlimbs are weak. Rectal examination may be normal, or weak, absent, or asymmetric iliac pulses may be palpated. Fremitus of the iliac arteries or terminal part of the aorta may be palpated. The terminal part of the aorta may feel larger or firmer than normal, or an aneurysmal dilation may be detected. Hindlimb weakness, inability to bear weight on the affected limb(s), and cold limbs with weak or absent femoral arterial pulses occur in affected calves.252 With verminous arteritis of the cranial mesentericSites of thrombosis associated with thrombophlebitis are likely to have pain, swelling, redness, and palpable thickening of the involved vein. These signs frequently occur within 12 to 24 hours after catheter removal when the thrombus is associated with catheterization. If there is bilateral jugular venous thrombosis, sudden, marked swelling of the head may occur. If the thrombosis involves the terminal aorta and iliac arteries in horses, the signs are frequently a vague hindlimb lameness, exercise intolerance, or poor performance. These nonspecific signs make it necessary to rule out lameness from other causes, cardiac disease, or respiratory problems. Failure to ejaculate has been reported in breeding stallions with aortoiliac thrombosis. Aortoiliac thrombosis in horses is also characterized by heavy sweating after exercise, except over the hindlimbs, which are cool. With severe aortoiliac thrombosis the affected limb can be cool to the touch at rest or can be cold with no artery, a thickened, dilated cranial mesenteric artery or aorta may be palpated that may be firmer than normal and have a weak pulse, or fremitus may be palpated.
In calves with aortic or aortoiliac thrombosis weakness, lameness, knuckling, paresis or paralysis of the hindlimbs, inability to rise, and cold hindlimbs 249253255 lacking a femoral arterial pulse have been described. ,The signs attributable to embolism and thrombosis may be identical. Embolism is usually manifested by an acute episode of pain or fever, abnormal pulsation in a peripheral vessel, or a change in skin temperature. If there is peripheral vessel showering, superficial veins may be collapsed and muscular weakness may be present. Embolic showering usually occurs in animals suspected of having or known to have thrombus formation.
Clinical signs associated with an aneurysm depend on its location and may vary from being asymptomatic to being a noticeable enlargement or mass associated with a blood vessel or causing colic, syncope, seizures, or sudden death on rupture. In a peripheral artery, a pulsatile expansile mass may be visualized or palpated. Other considerations for this finding are a false aneurysm and an arteriovenous fistula. A false aneurysm is clinically indistinguishable from a true aneurysm but can be distinguished ultrasonographically. A false aneurysm is caused by a break in the continuity of all three coats of the arterial wall rather than in the tunica media alone. This results in extravascular accumulation of blood in adjacent tissues. Signs attributable to low blood flow (e.g., lameness, colic, edema) may be present with arterial aneurysms. Aneurysms of the cranial mesenteric artery frequently manifest as chronic episodes of colic. With involvement of major cardiac vessels, there may be pain, an auscultable heart murmur, rapid tachycardia, signs of CHF, acute onset of pulmonary edema, or sudden death when the aneurysm ruptures. The latter signs make aneurysms difficult to distinguish from the clinical signs of a horse with valvular heart disease or cardiomyopathy. One cause of an aorticocardiac fistula in horses is the result of rupture of an
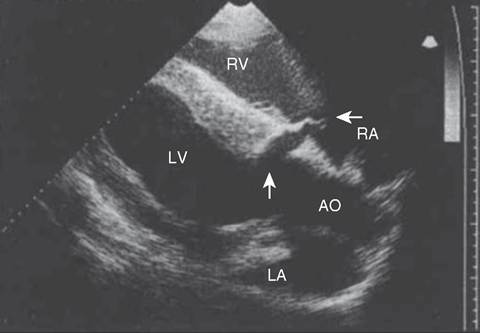
FIG.
30.27 Two-dimensional echocardiogram of a horse with a ruptured sinus of Valsalva aneurysm. Note the defect in the right side of the aorta at the sinus of Valsalva (vertical arrow) extending into the right atrium (horizontal arrow). The right atrium (RA), right ventricle (RV), left ventricle (LV), left atrium (LA), and aorta (AO) can be seen in this left ventricular outflow tract view.aneurysm of the sinus of Valsalva.87,94-96 Aortopulmonary rupture and fistulation occur in young to middle-aged Friesians, resulting in similar clinical signs in some horses, along with collapse, coughing, intermittent lameness, and fever.256,257
Clinical Pathology
Aneurysms or pseudoaneurysms may be visualized radiographically as soft tissue density masses continuous with a vessel wall (true aneurysm) or extending outward from a vessel wall (false aneurysm).242,243 However, the majority of the aneurysms involving the aorta and aortic root are not visible radiographically. Echocardiography is useful in the diagnosis of aneurysms involving the aortic root (Fig. 30.27).86,87,94-96 Echocardiographic diagnosis of rupture of aortic arch with pseudoaneurysm or aortopulmonary fistulation requires obtaining additional echocardiographic views, following the aorta and pulmonary artery cranially and dorsally.257 Recently aortic arch rupture has also been diagnosed with transesophageal echocardiography.257 Angiography can be used in the diagnosis of peripheral vessel swelling or suspected thrombosis but is of little use in diagnosis of aneurysms of major vessels in adult animals. Ultrasonography may be used for the diagnosis of aneurysms or thrombosis of major arteries and peripheral vessels. In aortoiliac thrombosis of horses, ultrasound has been used to determine the origin of the thrombus and the extent of occlusion of the involved arteries (Fig. 30.28).258 Abdominal ultrasonography of the upper left flank dorsal to the left kidney has been used to diagnose aortoiliac thrombosis in calves.253 Diagnostic ultrasound has been used to detect thrombi in the caudal vena cava in cattle.259,260 Although the occluding thrombus is not imaged, detecting a distended oval or round caudal vena cava rather than the normal triangular vessel in the eleventh and twelfth intercostal spaces is consistent with this diagnosis in cattle.
Thrombi have been detected ultrasonographically in the hindlimb in both horses and cattle.261-265 Jugular vein thrombophlebitis has also been diagnosed ultrasonographically in both horses and cattle (Fig. 30.29).128,266 Similarly, diagnostic ultrasound has been used to image the cranial mesenteric artery, its branches, and the aorta in horses with verminous arteritis.267 Aneurysms appear as dilated vascular structures or vascular outpouchings continuous with the vessel wall,86 whereas a thrombus is apparent as a hypoechoic to echogenic mass within a blood vessel.128 Cavitation of an occlusive thrombus is suggestive of septic thrombophlebitis (see Fig. 30.29), whereas a nonseptic thrombus usually has a homogeneously hypoechoic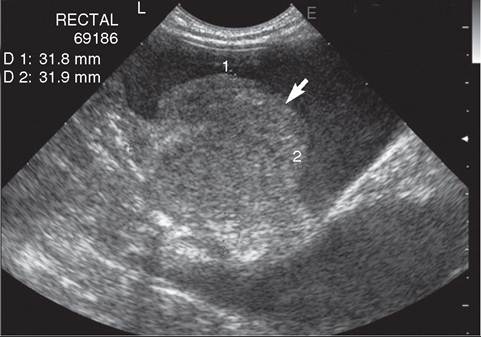
FIG. 30.28 Transverse transrectal sonogram of a large, somewhat heterogeneous thrombus (arrow) in the terminal portion of the aorta measuring 31.8 mm by 31.9 mm in diameter.
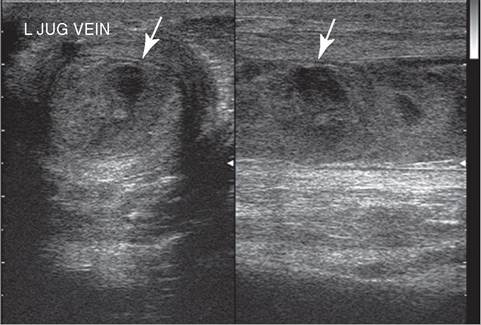
FIG. 30.29 Sonogram of the left jugular vein from a horse with septic thrombophlebitis. Note the cavitary appearance in the center of the thrombus (arrows) consistent with infection.
to echoic appearance.128 Complete occlusion of the vessel can be determined ultrasonographically, or flow within an aneurysm or alongside a thrombus determined. Doppler ultrasound provides a more sophisticated method for determining blood flow and vessel patency.
In the case of catheter-associated thrombosis, a positive catheter tip culture (>103 colony-forming units) along with a positive blood culture provides evidence of septic thrombo- phlebitis.268 An aseptic ultrasound-guided aspiration of the cavitary lesion within a heterogeneous thrombus can be performed, and the aspirate submitted for culture and sensitivity testing.128 Septic thrombophlebitis from any cause or embolic showering of septic thrombi may be accompanied by neutrophilic leukocytosis and elevation in fibrinogen concentration or SAA.
Pathophysiology
Irritation of the intimal lining of a blood vessel, stasis of blood flow, or existence of a hypercoagulable state triggers the clotting cascade and sets the stage for development of thrombosis. Further injury causes hemorrhage, more thrombosis, ulceration, and calcification. These in turn can compromise the media of the vessel, predisposing to aneurysm formation, and impinge on the lumen of the vessel, causing obstruction to blood flow. Either aneurysm or thrombosis can occlude blood flow to vital structures or organs, resulting in ischemia.
Thrombosis in any sizable vein causes venous hypertension, passive congestion, and subsequent edema and pain of the structure. As the thrombus matures, it adheres to the wall more, but with clot retraction and lysis, recanalization may occur. However, parts of the thrombus may protrude into the moving bloodstream and serve as the source of embolic showering, even during thrombus organization. The most common site for an embolus to lodge has not been established in large animals; the femoral and iliac arteries are common locations in humans. Emboli usually lodge at bifurcations, where the caliber of the artery is suddenly reduced.
The most common outcome of aneurysm of a major vessel is thought to be rupture. Rupture of sinus of Valsalva aneurysms into the right atrium, right ventricle, and interventricular septum has been reported in the horse.94-96 VT often occurs with rupture of an aortic sinus of Valsalva aneurysm and dissection into the interventricular septum.95,96 Unruptured aneurysms may have other complications, such as thrombosis or embolization of the thrombus. The frequency of rupture or embolic showering from thrombosis is unknown in animals. In Friesians, rupture of the aorta occurs into the pulmonary artery at the level of the ligamentum arteriosum and into the surrounding perivascular structures.256,257
Epidemiology
The significance of thromboembolism in large animals is poorly defined.
Spontaneous thromboembolism is commonly associated with parasitism in horses, and the aorta and cranial mesenteric arteries are the sites most frequently involved.162 Aortoiliac thrombosis is also a recognized syndrome diagnosed most frequently in heavily exercised horses. Although historically parasitism has been associated with aortoiliac thrombosis in horses, other causes of this syndrome are probable but have not been elucidated. Thrombotic disease can occur in any animal having repeated IV injections or being catheterized for administration of medication or fluids, but it is particularly common in horses with acute toxic enteritis, colitis, or sepsis. Careful skin preparation and aseptic technique are important factors in minimizing the likelihood of the patient developing catheter-related thrombophlebitis. Low doses of heparin have been effective in limiting the development of catheter-related thrombophlebitis in cattle.269 Large intestinal disease, hypoproteinemia, endotoxemia, salmonellosis, fever, diarrhea, and locally produced fluids have all been identified as risk factors for catheter-associated thrombophlebitis.248,270,271Arteriosclerosis is recognized in horses and in cattle. In cattle the lesion is most frequently caused by excessive vitamin D3 supplementation or ingestion of calcinogenic plants, such as Solanum malacoxylon, Cestrum diurnum, or Trisetum flavescens.m In horses the arteriosclerotic lesions were caused by lesions induced by Strongylus vulgaris?1 Ingestion of calcinogenic plants also occurs in horses, resulting in lesions in the aorta.
Aneurysms are uncommon in large animals but have been documented as the cause of sudden death in breeding stallions and racing Thoroughbred and Standardbred horses.96,97 Aneurysms of the sinus of Valsalva are one cause of aortic rupture in older horses and are probably congenital in horses, as they are in humans.86,94-96 Aortic root rupture also occurs without the presence of a preexisting aneurysm and has been associated with medial necrosis of the aorta. Psuedoaneurysm of the aorta in young Friesians is at the level of the ligamentum arteriosus, is a breed problem, and can result in sudden cardiac death, although many horses have a more chronic course.256,257
Necropsy Findings
Aneurysms are detected grossly as dilations of the involved blood vessel. Aneurysms of the sinus of Valsalva are characterized by an absent tunica media in the wall of the aorta, causing the aneurysmal dilation.76,86 Rupture of a sinus of Valsalva aneurysm

FIG. 30.30 Ascending aorta from a horse that experienced an acute onset of uniform ventricular tachycardia after exercise and died within 3 hours of onset. Note the irregular calcified surface of the aorta, consistent with atherosclerosis.
may occur into the right atrium, right ventricle, or interventricular septum, resulting in an ACF and volume over- load.76,86,87,95,96 Rupture through the tricuspid valve or chordae tendineae may also occur. Subendocardial dissection of blood down the interventricular septum may occur. Subsequent ruptures into the left ventricle and of the mitral chordae tendineae have also been reported. Pseudoaneurysms of the aorta with rupture at the ligamentum arteriosum and into the pulmonary artery occur in the Friesian breed.244,256,257 Aneurysms of the major vessels leaving the heart may involve more than one vessel by dissection and hemorrhage. Aneurysms may contain thrombi or parasites, and there may be evidence of embolic showering of thrombi into peripheral vessels or other organ systems, especially the lungs. Histologically there may be necrosis and inflammation at the site of the aneurysm with foci of mineralization.
Thrombosis and arteriosclerotic lesions are recognized as rounded, well-demarcated fibrous plaques frequently located in the thoracic and cranial abdominal aorta (Fig. 30.30). The plaques may contain a central calcified core or parasitic larvae. Microscopically there is a thin layer of fibrin, platelets, and inflammatory cells in early lesions, whereas older lesions have a greater fibrous component. Thrombotic lesions may be associated with proliferation of the underlying aortic intima. In horses, parasitic larvae may be found.
Treatment and Prognosis
Aneurysms of major vessels carry a guarded to grave prognosis because surgical correction is rarely attempted and spontaneous rupture is thought to be relatively common. Intact aneurysms of the sinus of Valsalva can be detected echocardiographically, and once an aneurysm has been detected, the horse should be removed from all athletic competition because of the risk of rupture.86,118 The occlusion of an ACF has been successfully performed with an Amplatzer occluder device in a breeding stallion.273 This stallion survived to discharge but was euthanized a month and half later due to worsening of his underlying heart disease.
Treatment of thrombosis consists of removal of the catheter, if present, and resting the affected vessel. Warm compresses or hydrotherapy may be helpful in some animals. Topical NSAIDs (diclofenac sodium) may also be useful. Support wraps may be useful to control swelling. The effectiveness of anticoagulant therapy (clopidogrel usually at 2 mg/kg twice daily PO in horses, aspirin at 100 mg/kg once daily PO, ruminants; 10 mg/kg once daily, horses; or sodium heparin at 30 to 40 units/kg SC twice daily) or antiinflammatory drugs for dissolving a thrombus is questionable. Anticoagulant therapy may be useful in preventing additional thrombus formation or propagation of the existing thrombus. Ultrasonographic guidance can be used to obtain a sterile aspirate of the cavitated area of the thrombus for culture and sensitivity testing when septic thrombophlebitis is suspected.128 Broad-spectrum bactericidal antimicrobial therapy should be instituted for suspected septic thrombophlebitis or when a cavitated thrombus is detected ultrasonographically and modified, if necessary, on the basis of the results of culture and sensitivity testing.128 Bacterial endocarditis, particularly involving the tricuspid valve, is a potential complication of septic jugular vein thrombophlebitis. With the exception of a jugular venous thrombus or some horses with aortoiliofemoral thrombosis, surgical removal of an embolism or thrombus is rarely attempted in large animals. Surgical resection of a jugular vein with septic thrombophlebitis has been performed successfully when the surgeon could ligate the affected vein above and below the thrombus. Jugular vein thrombectomy with removal of the contents of the affected portion of the vein has been performed successfully in horses.274 Although the prognosis for complete resolution of the thrombophlebitis is guarded, especially if the thrombus is infected, many veins do recannulate with complete resolution of the thrombus and without vascular stricture. However, the time course is slow, and persistent local induration and obstruction to blood flow may persist. The prognosis for nonracehorses to return to the same level of performance is good.275 However, Standardbred racehorses in this same study had a decreased chance of returning to racing at the same level.275
The prognosis for horses and calves with aortoiliac thrombosis is guarded. Although most calves with aortoiliac thrombosis have died or were euthanized, two calves have survived. One calf received antithrombotic treatment with unfragmented heparin and aspirin, and the other was treated with ketoprofen, acepromazine, and local heat. A wide variety of medical treatments have been proposed for horses with aortoiliac thrombosis, including sodium gluconate, larvicidal deworming, phenylbutazone, and a controlled exercise program. Success has been variable. Surgical thrombectomy has also been successful in some horses.276-278
Prevention and Control
Thrombosis and embolization from IV catheters can be prevented or their incidence reduced by aseptic insertion, stabilization of the catheter, use of topical antiseptics, application of a sterile dressing, daily inspection of the catheter and vein, and replacement of the catheter at another site (preferably in another vein) if phlebitis occurs. Dwell time is a significant factor in the development of thrombophlebitis, and catheters should be replaced by new ones at another site every 72 hours.279 Attempts should be made to place long-term catheters in large peripheral or central veins where contact between the endothelium and catheter is minimized and medications administered are diluted by the large volume of blood flow. Catheters left in place for prolonged periods should be of silicone rubber or polyurethane.268 Clopidogrel (2 mg/kg PO twice daily, horses), aspirin (100 mg/kg PO once daily, ruminants; 10 mg/kg/day, horses), and low-dose heparin (30-40 units/kg SC twice daily, ruminants and horses) therapy should be considered to prevent thrombus formation in septic or endotoxic patients. Horses are much more prone to jugular thrombosis than are ruminants.
Parasite control is important in the control of thromboembolic disease and aneurysm in horses. Aneurysms of the sinus of Valsalva may be detected by routine echocardiographic screening of horses but occur so infrequently that this is not practical. In cattle, arteriosclerotic lesions are prevented by proper calcium and vitamin D supplementation.