Pharyngeal Trauma and Abscess
Bradford P. Smith
Definition and Etiology
Pharyngeal trauma occurs relatively frequently in cattle, which results in cellulitis, abscessation, or hematoma formation. One case resulted in megaesophagus.
Pharyngeal trauma is almost always associated with use of a balling gun, long dose syringe, speculum, paste wormer gun, rigid probe of calf esophageal feeder, or rigid stomach tube.1 A foreign body such as a sharp stick or wire occasionally perforates the pharynx. Hematomas may result from unidentified blunt trauma. The puncture or laceration may be very small and usually is located in the area near the origin of the esophagus. The result is that feed and saliva enter the retropharyngeal area, and inflammation develops (also see Chapter 31, Retropharyngeal Lymph Node Abscessation section).Clinical Signs and Differential Diagnosis
The clinical signs include anorexia, drooling of saliva, malodorous breath, extended head and neck, localized or diffuse pharyngeal pain, feed coming from the external nares, and forestomach stasis or bloat. Severe cases may involve obvious pharyngeal swelling, fever, easily elicited cough on laryngeal palpation, dyspnea, and aspiration pneumonia. Intraluminal submucosal pharyngeal abscesses with similar clinical signs have been reported. The differential diagnosis in cattle must include retropharyngeal abscesses (also see Chapter 31, Retropharyngeal Lymph Node Abscessation section), pharyngeal foreign body, actinobacillosis, megaesophagus, and lymphosarcoma or other tumors that involves the pharyngeal lymph nodes.
Careful digital palpation of the pharynx via the mouth often reveals the diagnosis, although restraint is difficult because the area is painful and swollen, causing dyspnea and struggling. A well-lubricated stomach tube should be gently passed to relieve bloat and ascertain that no esophageal obstruction is present.
Pharyngeal trauma is rare in sheep and goats, and retropharyngeal abscesses caused by Corynebacterium pseudotuberculosis (caseous lymphadenitis) are the most common cause of pharyngeal swelling.Clinical Pathology and Laboratory Aids
Endoscopy and radiography may be of great help in diagnosing the site of the lesion, the extent of cellulitis, and the presence of a foreign body. Endoscopy reveals a swollen, collapsed pharyngeal air space. The wound may be visible, and it may have exudate at its origin. Endoscopy can help rule out intraluminal masses and foreign bodies. Retropharyngeal cellulitis, abscess, or hematoma often can be visualized radiographically, and radiopaque foreign bodies can be seen (Fig. 32.87). Gas in the soft tissues or a discrete mass can be seen with cellulitis and abscess, respectively. Gas can often be seen in the lumen of the esophagus as well. Radiographs of the lungs and thorax may be helpful if aspiration pneumonia or mediastinitis is suspected. In some cases in which no appropriate treatment is instituted early or treatment fails, the infection can reach the mediastinum via the thoracic inlet, and the prognosis becomes more guarded. The results of hematologic analysis may reflect an infectious inflammatory process.
Pathophysiology
Inflammation, swelling, and necrosis in the retropharyngeal tissues interfere with normal swallowing by causing pain when swallowing is attempted, by causing physical interference with
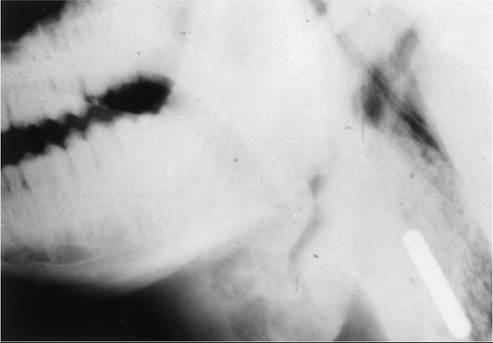
FIG. 32.87 Pharyngeal trauma in a 2-year-old bull caused by a magnet that was given forcefully with a balling gun 24 hours previously. The magnet is visible in the retropharyngeal tissues surrounded by cellulitis, with swelling and gas in the tissues. The area is swollen and painful.
passage of a bolus, and by causing neurologic involvement. The resultant dysphagia may predispose the animal to inhalation of feed and saliva.
If the retropharyngeal inflammation affects the pharyngeal branch of the vagus nerve on the dorsolateral surface of the pharynx, the esophageal and pharyngeal phases of swallowing and eructation are disturbed.1 The resultant pharyngeal paresis may lead to reflux of feed through the nares. Involvement of the adjacent cranial laryngeal nerve makes the laryngeal mucosa less sensitive to foreign material and thus diminishes the cough reflex. Severe inflammation may involve the vagus nerve itself and cause forestomach stasis with bloat and laryngeal motor dysfunction.1-3 Eructation also involves pharyngeal muscular activity, and the maneuver is likely to be quite painful when cellulitis is present in the area.
Treatment and Prognosis
In spite of the fact that affected animals often are completely anorexic and febrile and look very ill, most cases of pharyngeal puncture or laceration resolve successfully if the animal can be vigorously treated with broad-spectrum antimicrobial drugs for 7 to 14 days, if aspiration pneumonia can be controlled by limiting access to feed, and if adequate supportive care can be given. Tetracyclines, ampicillin, ceftiofur, trimethoprimsulfonamide, and florfenicol have been used successfully. NSAIDs should be given for analgesia and for their ability to reduce inflammation. Oral administration of boluses should be avoided. FARAD must be checked before drugs are given off label (www.farad.org/vetgram/).
Affected animals should have access to water; if they cannot drink, and if passage of a tube is possible, a soft stomach tube should be used several times daily to gently administer a total of 30 to 50 L (8 to 13 gallons) of water plus electrolytes daily. If tolerated, it can be passed nasally and left in place securely sutured or taped in place to a halter. Alternatively, a rumen fistula may be surgically placed and used to water and feed the animal. The most important electrolyte to administer is potassium: 60 to 100 g of potassium chloride should be given daily with the water.
Once the animal can drink without coughing or nasal reflux, soft green grass or a soft mash should be offered. If this is well tolerated, it should be continued for 2 weeks, after which green pasture or soft, green, leafy alfalfa hay or other equally palatable feed should be gradually and carefully introduced into the diet.If a discrete retropharyngeal abscess forms, it is best first to attempt drainage into the pharynx through the original laceration by pushing a finger into the healing wound until pus escapes. If this fails, a surgical approach to the area may be necessary. Surgery is rarely required in cases of pharyngeal trauma or laceration with cellulitis.
Prevention and Control
Careful use of balling guns, paste wormer guns, and other equipment that can damage the pharynx is the best prevention. Adequate restraint of the head of any animal that is to be orally treated also helps prevent pharyngeal trauma. Care should also be taken to ensure that no wire, thorns, or sticks are incorporated in hay.