Silicate Associated Osteoporosis
Scott A. Katzman
■ Introduction Silicate associated osteoporosis (SAO), also referred to as bone fragility syndrome (BFS) or bone fragility disorder (BFD), is a progressive debilitating musculoskeletal disorder with a geographic distribution similar to that of pulmonary silicosis, primarily affecting horses in the region of the Monterey-Carmel peninsula of California, Sonoma and Napa counties, although occasional cases are identified in other regions of California.1-3 Although SAO, BFS, and BFD tend to be used interchangeably to describe this condition, SAO is preferred, as this most accurately represent the disease process, reflecting its close association with pulmonary silicosis and similar geographic distribution.1-3 Briefly, pulmonary silicosis in horses results from inhalation of cytotoxic, fibrogenic silicates, with cristobalite being primarily implicated in the development of the condition and geographic distribution related to exposure of horses to Miocene Monterey Shale soil of the Monterey Peninsula region of California, which contains high levels of cristobalite.4
Early clinical features associated with SAO include intermittent lameness affecting one or multiple limbs that cannot be localized,1,2,5 exercise intolerance, and generalized stiffness.1,2 In the later stages of the disease process, lameness may become severe1,2; scapular bowing (Fig.
38.42, A and B) and lordosis (Fig. 38.42, C) are common features,1,2,5 with a pain response elicited on palpation of the scapulae5; and range of motion of the cervical spine may be decreased in both mediolateral and dorsoventral planes.1,5 Generalized weight loss is also commonly observed, with varying degrees of localized muscle atrophy developing in the shoulder and gluteal regions.1Whether in the early or late stages of the disease process, the cause for progressive musculoskeletal abnormalities observed in SAO-affected horses is secondary to abnormal bone turnover and pathologic fractures affecting primarily the axial and proximal appendicular skeleton.
However, clinically significant lesions have occasionally been identified in the radii and tibiae, and changes in bone morphologic and mechanical properties in affected horses have been demonstrated to develop as far distally as the distal metacarpus.6Signs of respiratory tract disease are often identified on physical examination or are a noted as a historical feature and include adventitious bronchovesicular sounds on auscultation,1 increased respiratory rate,1 flaring of the nostrils at rest,1 and coughing.2 Although a direct link has not yet been elucidated, the signs of respiratory disease observed in several of these instances are suspected to be related to concomitant pulmonary silicosis, which has been confirmed in select cases. In one study describing the clinical features of 16 horses diagnosed with SAO,1 a definitive diagnosis of pulmonary silicosis was made based on results of bronchoalveolar lavage in 3 of 7 horses for which this diagnostic was pursued, and 4 others had characteristic radiographic evidence of pulmonary silicosis7 on thoracic radiographs. In another study, 9 of 9 horses diagnosed with SAO on postmortem examination had cytotoxic silica dioxide polymorphs (cristobalite, quartz, tridymite) identified in lung tissue (6 of 9) and/or tracheobronchial lymph nodes (8 of 9).3
Treatment of SAO-affected horses is primarily palliative,1,2 and the most devastating consequence of SAO is catastrophic fracture of an affected bone, necessitating euthanasia.1
■ Etiology and Pathogenesis To date, the etiology and pathogenesis of SAO have not been completely determined, although development of pulmonary silicosis and silicotic tracheobronchial lymphadenitis is attributed to the inhalation of the cytotoxic silicate cristobalite, which is suspected to be the etiologic agent directly responsible for SAO.1-3 As noted previously, this is due to the similar geographic distribution between the two conditions, as well as to the diagnosis of both conditions simultaneously, as documented in several instances.1,3 Proposed mechanisms for development of SAO include exposure to high levels of cristobalite, causing chronic systemic inflammation; dissemination of silicate-containing macrophages to bone marrow secondary to pulmonary silicosis or silicate tracheobronchial lymphadenitis; or abnormal resorption and remodeling of bone due to abnormal osteoclastic activity, comparable to Paget's disease of bone in humans.2,3 Microscopically, bone lesions are characterized by multinucleate hypertrophied osteoclasts indiscriminately resorbing bone and associated hypertrophied osteoblasts lining bone surfaces.3
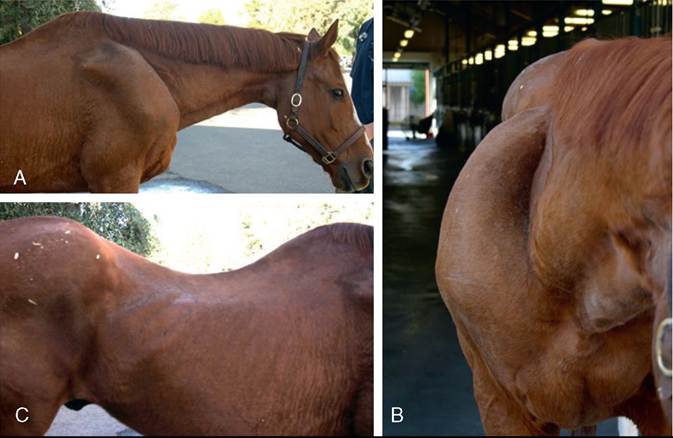
FIG.
38.42 Advanced case of SAO showing phenotypical (A) pronounced lateral bowing and (B) deformation of the scapula, as well as (C) marked lordosis.■ History and Clinical Signs There does not appear to be a breed or sex predilection for development of SAO, and it has been diagnosed in horses ranging in age from 4 to 22 years, with a mean age of approximately 10 to 14 years.1-3,5 Due to its geographic distribution, SAO should be considered in the differential diagnosis for horses that reside or have resided in the Monterey-Carmel peninsula of California, Sonoma or Napa counties, and that are presented for any of the previously mentioned early signs of the disease (nebulous persistent or intermittent lameness, exercise intolerance, or generalized stiffness). For the horse older than 10 years that is presented with signs of advanced disease (marked lordosis, severe lameness, scapular deformation, weight loss, decreased cervical range of motion with or without signs of concurrent respiratory pathology), SAO should be a top differential.
It is important to remember the strong circumstantial evidence for a direct association between SAO and pulmonary silicosis and that exposure to cristobalite is responsible for the development of SAO.2,3 It is unclear how long and at what concentration horses need to be exposed to the aerosolized silicate particles for disease to develop, and it is also unknown at what rate SAO develops following exposure8; however, severe multifocal osteolysis associated with SAO has been reported in a horse stabled in an endemic area after a period of only 2 years. In some instances, horses may have no known history of residing in endemic areas or may have spent only short times in these areas. In addition, there are endemic farms from which multiple horses develop SAO, and recent excavation in endemic areas can result in aerosolization of high concentrations of silicates that may be subsequently inhaled by susceptible horses, potentially accelerating the development and progression of disease.
Therefore recent excavation in the vicinity of a horse presented with signs attributable to SAO as well as a history of clusters of affected horses in a small geographic area should be noted.Because much remains unknown about the etiology and pathogenesis of SAO, it can present a diagnostic challenge, particularly in the early stages of the disease process.
■ Diagnosis Definitive diagnosis is made on postmortem examination. Currently, nuclear scintigraphy is the most reliable antemortem diagnostic test available for making a presumptive diagnosis of SAO.5 Characteristic multifocal areas of increased radiopharmaceutical uptake (IRU) identified on whole body scintigraphic examination include, in descending order of prevalence, the scapulae (Fig. 38.43, A), ribs (Fig. 38.43, B), sternebrae, cervical vertebrae, tuber sacrale, ilium, ishium, and tuber coxae.1 Less commonly, areas of focal IRU are identified in the long bones of the appendicular skeleton.1,2 It has been established that because the majority of lesions are located from the ribs cranially, hind end scintigraphy is unnecessary in making a presumptive antemortem diagnosis.2
Other diagnostic methods that have been investigated to evaluate their efficacy in the diagnosis of SAO include scapular ultrasonography, serum biomarkers of bone turnover, and findings on physical examination.5 When compared to scintigraphy, it was found that in moderate to severe cases, bowing of the scapulae on physical examination and widening of the scapular spine on ultrasonographic examination were strongly supportive of a diagnosis of SAO and that serum biomarkers of bone turnover were not accurate in supporting the diagnosis.5 In mild cases, none of these three methods were accurate, and regardless of the severity of SAO, none was as accurate as scintigraphy under any circumstance.
Bone biopsy obtained from regions of focal IRU may reveal osteopenia, fibrosis, and focal regions of bone resorption, but in some cases may be unremarkable.1 Currently, bone biopsy is not routinely performed in the diagnosis of SAO.
In addition, CBC and serum biochemistry are consistently unremarkable in these cases.■ Treatment Treatment is palliative and aimed at decreasing inflammation and osteoclastic bone resorption. The most effective treatment to date has been intravenous administration of the nitrogen-containing bisphosphonate zoledronate at a dose of 0.057 to 0.075 mg/kg.2,9 In one study, 9 of 10 SAO-affected horses treated with zoledronate had improvement in lameness scores or resolution of lameness.2 Eight of ten of these horses also had a subjective decrease in radiopharmaceutical uptake on nuclear scintigraphy performed 6 months after a diagnosis of SAO based on initial scintigraphic examination.
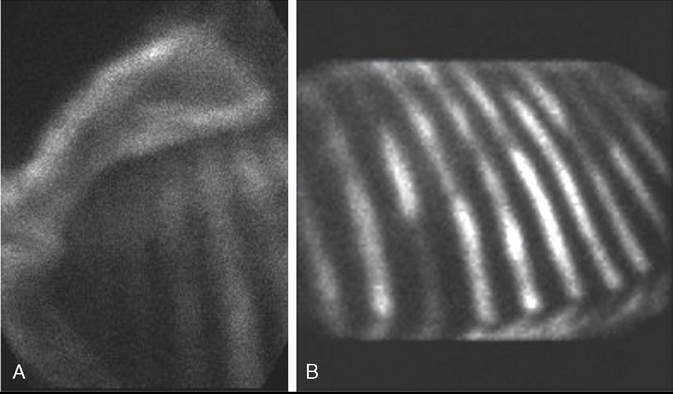
FIG. 38.43 Scintigraphic images of the same horse shown in Fig. 38.42, demonstrating (A) lateral bowing of the scapula with increased radiopharmaceutical uptake (IRU) in the regions of the scapular spine and caudal border of the scapula, as well as (B) diffuse patchy multifocal IRU noted along the length of several ribs.
Bisphosphonates are a class of drugs that inhibit bone resorption through osteoclast inhibition.10 Following administration, bisphosphonates are incorporated into hydroxyapatite, the inorganic component of bone. When released from hydroxyapatite through osteoclastic resorption of bone, they induce osteoclast apoptosis, halting bone resorption. The non-nitrogen-containing bisphosphonate tiludronate has been used in the treatment of SAO, with limited, transient improvement noted after administration.2
One third to two thirds of bisphosphonates administered are incorporated into the skeleton, with the remainder excreted through the kidneys. Adverse systemic reactions following bisphosphonate administration are relatively rare in horses. There have been anecdotal reports of horses developing signs of acute renal failure following administration of bisphosphonates, so it is recommended to perform serum biochemical analysis to rule out preexisting renal disease prior to administration.
Additional complications that have been reported following bisphosphonate administration include signs of abdominal discomfort and hypocalcemia. For these reasons, it is recommended to administer a single intravenous dose of flunixin meglumine (1.1 mg/kg) 30 minutes prior to zoledronate administration and maintain the horse on a 50% alfalfa diet to promote dietary calcium intake.2In moderate to severe cases of SAO, exercise restriction is recommended to decrease the risk for catastrophic fracture, and judicious use of NSAIDs is often instituted to further reduce inflammation. In mild cases, exercise restriction and further pharmacologic intervention may not be necessary, but this must be determined on a case-by-case basis.
Finally, moving affected horses out of an endemic area may be of benefit, although doing so may not halt the progression of signs or prevent further signs from developing.
■ Prognosis Prognosis is fair in the early stages, with return to athletic function possible following diagnosis and treatment. However, the owner must be warned of the risk for musculoskeletal injury secondary to decreased bone strength in these cases.
Prognosis is guarded to poor in later stages, and athletic use cannot be recommended due to the increased risk for musculoskeletal injury. In the advanced stages, SAO can be debilitating, resulting in poor quality of life. Catastrophic fractures frequently occur in these moderate to severe cases, regardless of the treatments used. These two factors, poor quality of life and catastrophic fracture, often necessitate euthanasia in advanced cases of SAO.