Temporohyoid Osteoarthropathy
Tracy E. Norman
■ Definition and Etiology Temporohyoid osteoarthropathy (THO) is a disease of bony proliferation at the junction of the stylohyoid and petrous temporal bones.
Several etiologies have been proposed for this condition, and the true etiology is likely variable. In some cases, bone inflammation and remodeling may occur secondary to extension of otitis media, otitis interna, or upper respiratory tract infection.1-5 There is also evidence that many of these cases are due to primary degenerative joint disease.6 Regardless of the cause, the result is bony proliferation of the tympanic bulla, proximal stylohyoid bone, and petrous temporal bones, often resulting in arthrosis of the temporohyoid joint and subsequent fracture of the stylohyoid and petrous temporal bones.1-6 These fractures rarely extend into the basisphenoid and basioccipital bones, resulting in meningitis and brainstem disease.1 Pain and inflammation associated with fracture or altered mobility of the joint and impingement on surrounding nerves result in the observed clinical signs.■ Clinical Signs Horses with THO may not show clinical signs, but two clinical syndromes are associated with THO. Nonneurologic signs may be chronic and include difficulty chewing, nasal discharge, head tossing, ear rubbing, otorrhea, resentment of the bit, head shyness, and pain on manipulation of the head or ears.1-3 Neurologic abnormalities generally include acute onset of signs of facial and vestibular nerve dysfunction, including ear droop, ptosis, muzzle deviation away from the affected side, corneal ulceration, head tilt toward the affected side, circling, ataxia, nystagmus, and collapse.1,5,6 Auditory dysfunction is common or ubiquitous in horses with neurologic signs associated with THO but may not be appreciated on standard clinical observation.5,7 Damage to the parasympathetic portion of the facial nerve may result in reduced lacrimation.4 Occasionally dysphagia is also observed.
Rarely, seizures or sudden death may occur secondary to fractures that extend into the cranial vault.1 Clinical signs generally have an acute onset and may be associated with manipulation of the head for other reasons (passage of nasogastric tube, etc.).1■ Diagnosis Pathologic alterations at the temporohyoid joint may be identified using radiography, guttural pouch endoscopy, CT, or MRI. Otoscopic examination has been reported to identify THO.8 Radiographs may show evidence of osseous proliferation at the temporohyoid joint on lateral and dorsoventral projections but in general are found to be less sensitive at detecting abnormalities than other diagnostic modalities.1
Endoscopy of the guttural pouches has been shown to be sensitive in detecting early, as well as advanced, changes at the temporohyoid joint, including soft tissue inflammation and hemorrhage, osseous proliferation, enlargement of the stylohyoid bone, and previous sites of fractures (Fig. 38.44).1 The contralateral guttural pouch should always be evaluated, as
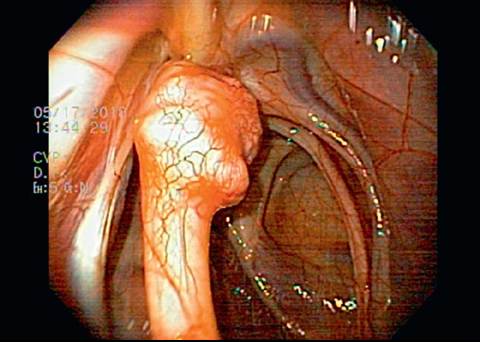
FIG. 38.44 Transendoscopic image of the right guttural pouch demonstrating enlargement of the proximal aspect of the right stylohyoid bone consistent with temporohyoid osteoarthropathy.
some horses have bilateral disease. Evaluation of laryngeal function may be performed concurrently; in a recent study, 61% of horses with THO also had some degree of left laryngeal dysfunction. The association between these conditions was assessed to be most likely coincidental. Awareness of laryngeal dysfunction is important, however, especially in surgically managed cases.7 Because endoscopy equipment is readily available and evaluations can be performed in the conscious horse, it may be the diagnostic modality of choice.
CT and MRI may be indicated to provide additional information.
CT allows exceptional visualization of bony proliferation and can reveal fractures that cannot be detected on plain radiographs because of superimposition of structures. Advancements in this technology and full understanding of the appearance of the topographic anatomy have increased the utility of this modality.2,3,6MRI yields greater soft tissue detail than CT and is useful in documenting fluid accumulations in the middle and inner ear, as well as identifying inflammatory brain lesions.1 The biggest impediment to the implementation of these imaging technologies is the requirement for general anesthesia and the difficulty of recovering a horse with vestibular abnormalities following the procedure.
■ Treatment and Prognosis Treatment of THO may include both medical and surgical management. Medical management generally includes antiinflammatory and supportive care. If ptosis and reduced lacrimation lead to exposure keratitis and corneal ulceration, tarsorrhaphy may be beneficial, and intensive medical therapy is required. If otitis is suspected, or if there is a suspected fracture into the cranial vault, the use of broad-spectrum antimicrobials with good penetration of the blood-brain barrier is indicated.
Surgical therapy for THO has been described.1,9,10 Partial stylohyoidectomy has been used in some cases to reduce the forces on the ankylosed temporohyoid joint and prevent fracture of the petrous temporal bone.1,9 This procedure risks damage to the adjacent nerves and may result in the formation of a bony union at the stylohyoidectomy site. An alternate technique is ceratohyoidectomy, which eliminates the lever arm that drives movement of and pressure on the temporohyoid joint. Cera- tohyoidectomy is technically simpler to perform than partial stylohyoidectomy, avoids the complications of that procedure, and may be performed prophylactically or in cases in which fracture of the petrous temporal bone has occurred.9,10
In horses with THO, the prognosis for survival is good and for return to athletic function is fair.1,7 Surgical management appears to result in better neurologic outcomes and reduced treatment times compared with medical management.7 Improvement in neurologic function may continue for up to 2 years, but auditory loss appears to be permanent,7 and facial nerve dysfunction also commonly persits.1 The most common secondary complication of THO is corneal ulceration on the affected side due to poor eyelid tone and decreased lacrimation resulting in exposure keratitis. The majority of these horses should recover fully, but healing time may be protracted.1