Streptococcus equi subsp. equi Infection (Strangles)
Ashley G. Boyle
The highly contagious S. equi subsp. equi infections in horses, commonly referred to as strangles, were first described in early veterinary science literature by Jordanus Ruffus in 1251.1 The causative organism will be referred to as S.
equi in this section.■ Clinical Signs Strangles is characterized by sudden onset of fever followed by upper respiratory tract catarrh, as evidenced by mucopurulent nasal discharge and acute swelling with subsequent abscess formation in submandibular and retropharyngeal lymph nodes (Fig. 31.24). The term strangles was coined because affected horses sometimes suffocated as the lymph nodes became enlarged and obstructed the airway. Strangles is currently a reportable disease in many U.S. states.
Fever is the first clinical sign and remains as lymphadenopathy develops and abscesses mature. Pharyngitis makes swallowing painful, and affected animals may become anorectic or reluctant to eat and stand with the neck extended.
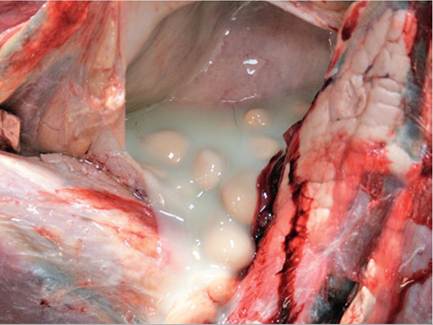
FIG. 31.25 Guttural pouch Streptococcus equi empyema with chondroids at postmortem. (Courtesy Dr Julie Engiles, University of Pennsylvania, New Bolton Center, Kennett Square, Penn.)

FIG. 31.26 Horse with the unique presentation of periorbital abscessation with concurrent ocular discharge that cultured positive for Streptococcus equi. (Courtesy Dr. Erica Koch, Wentworth Equine Veterinary Services, Wolfeboro, N.H.)
Lymphadenopathy is a major clinical sign. The submandibular and retropharyngeal lymph nodes are about equally involved in S. equi infections. They usually become swollen and painful approximately 1 week after infection. Other lymph nodes of the head region (parotid, cranial, and cervical) are also frequently involved and may abscess.
Retropharyngeal lymph nodes may drain into and cause empyema of the guttural pouch (Fig. 31.25). Periorbital abscesses can cause marked swelling of the eyelids and result in ocular discharge that will culture positive for S. equi if sampled (Fig. 31.26). Abscesses of the lymph nodes at the thoracic inlet can cause severe tracheal compression, asphyxia, and death. Clinical severity and progression varies greatly depending on the immune status of the animal.■ Pathogenesis S. equi is of the Lancefield group C streptococcal diseases and enters via the mouth or nose and attaches to cells in the crypt of the lingual and palatine tonsils and to the follicular-associated epithelium of the pharyngeal and tubal tonsils. There is no evidence of colonization before penetration. After a few hours, the organism is difficult to detect on the mucosal surface but is visible within cells of the epithelium and subepithelial follicles. Translocation to the mandibular and suprapharyngeal lymph nodes that drain the pharyngeal and tonsillar region occurs in a few hours.2
Complement-derived chemotactic factors attract large numbers of polymorphonuclear neutrophils (PMNs), although gross evidence of abscessation is not visible for 3 to 5 days after S. equi enters the lymph nodes. Failure of neutrophils to phagocytose and kill the streptococci appears to be a result of a combination of the hyaluronic acid capsule, antiphagocytic SeM protein, Mac protein, and other undetermined antiphagocytic factors released by the organism. Depending on the immune status of the patient and the degree of exposure to S. equi bacterial load, clinical signs may develop 3 to 14 days after exposure.1
Although strangles involves predominantly the upper airways, including the guttural pouches and associated lymph nodes, metastasis to other locations occasionally occurs. Spread may be hematogenous or via lymphatic channels, which results in abscesses in lymph nodes and other organs of the thorax and abdomen.
This form of the disease is known as bastard strangles.Nasal shedding of S. equi usually begins 2 to 3 days after onset of fever and persists for 2 to 3 weeks in most animals. Some animals never shed. In others, nasal shedding may last at least 6 weeks after purulent discharges have stopped. Persistent guttural pouch infection may result in intermittent shedding for years.3,4 Systemic and mucosal immune responses are evident 2 to 3 weeks after infection and coincide with mucosal clearance.
As long as they were not treated with antimicrobials, approximately 75% of horses develop a waning immunity to strangles that lasts about 5 years after recovery from the disease. A small percentage of these horses become susceptible to a second attack of the disease within months, which probably represents a failure to produce or maintain an adequate level of the appropriate mucosal and systemic antibodies. Older horses with residual immunity have limited susceptibility and develop a mild form of strangles often called catarrhal strangles. These animals shed virulent S. equi that will produce severe disease in more susceptible, often younger horses. Colostral antibodies ingested during the first 24 hours of life have also been shown to recirculate to the nasopharyngeal mucosa, thus providing an additional source of protection to the foal during its first weeks. Foals that suckle immune mares are usually resistant to S. equi infection until weaning.1
■ Epidemiology
TRANSMISSION. Outwardly healthy horses that still shed organisms are a source of infection when introduced into a new population of horses. Definitive determination of carrier status requires endoscopic examination of the guttural pouches as well as PCR testing of guttural pouch lavage fluid.1,5,6 S. equi may originate from outwardly healthy horses such as the following:
• Horses that are incubating the disease and go on to develop signs themselves
• Horses that are recovering from recent disease but that continue to harbor the organism after full clinical recovery for some weeks
• Horses that are fully recovered from the disease but continue to be potentially infectious for prolonged periods through periodic shedding of S.
equi (carriers)ENVIRONMENTAL PERSISTENCE OF STREPTOCOCCUS EQUI. Currently there is a lack of definitive field-based evidence for prolonged environmental persistence. S. equi is known to be sensitive to bacteriocins from environmental bacteria and does not readily survive in the presence of other soil-borne flora. Modeled environmental field conditions revealed that the organism was found to persist for less than 4 days, but moist environments (e.g., water buckets) may allow the organism to persist for extended periods (up to 34 days) when protected by cold conditions.7,8
■ Diagnosis Early definitive diagnosis is essential for containing this highly infectious disease. Sampling may be unsuccessful during the incubation and early clinical phases. S. equi is normally not present on the mucosa until at least 24 to 48 hours after the onset of fever, so infection in horses monitored by daily measuring of rectal temperatures during an outbreak may be recognized early and isolated to limit transmission of S. equi. Samples can be obtained via nasopharyngeal swab, nasopharyngeal wash, and guttural pouch wash. A comparison of S. equi sample type is found in Table 31.8.1 Cytologic evaluation reveals gram-positive extracellular cocci in long chains, supporting a general diagnosis of a β-hemolytic streptococcus organism. Common hematologic findings of horses with S. equi are hyperfibrinogenemia, neutrophilic leukocytosis, and mild anemia.9
■ TABLE 31-8
Comparison of Sample Type for Diagnosis of Streptococcus equi1
S. equi Sample
Pros
Cons
| Aspirate of mature abscessed High yield of bacterial organisms lymph node Moistened rostral nasal swaba Ease of sampling Moistened nasopharyngeal swaba Ease of sampling | Requires this stage of disease Animal needs to have active mucopurulent discharge False negatives possible in early febrile state (not shedding yet) False negatives possible due to intermittent shedding from guttural pouch |
| Nasopharyngeal wash Ease of sampling | False negatives possible in early febrile state (not shedding yet) |
| Sampling more surface area | False negatives possible due to intermittent shedding from guttural pouch |
| Was found to be more sensitive than nasopharyngeal swab9 Guttural pouch lavageb Best for detection of carrier animals | Special equipment needed Experience needed entering the guttural pouch More time consuming False negative if lymph nodes have not yet ruptured into the pouch |
aSynthetic microfiber flocked swabs have not shown increased detection rates over traditional rayon or cotton swabs.
bThe committee recommends guttural pouch lavage quantitative polymerase chain reaction (qPCR) for the detection of carriers with concurrent visual inspection of the guttural pouch via endoscopy. To limit the contamination of the environment and the veterinarians, we recommend collection directly from the guttural pouch, rather than via free catch from the nasal passage.
CULTURE. Culture is the preferred method on aspirates of mature abscesses, but it takes a minimum of 24 hours to obtain results. Culture is inexpensive, sensitive, and accurate for samples that have large numbers of bacteria, such as those collected from animals with obvious disease. Unfortunately, up to 40% of samples can be falsely negative on culture, especially in patients sampled too early in the course of disease or during convalescence.10
POLYMERASE CHAIN REACTION. Multiple gene targets are available for the detection of S. equi via quantitative polymerase chain reaction (qPCR), and this technique has been shown to be more sensitive than culture as a diagnostic tool.1,9-12 Nasopharyngeal washes (Fig. 31.27) are preferable to nasopharyngeal swabs due to a larger sampling area,1 but guttural pouch sampling is 50 times more likely to detect carrier animals.1 Absence of obvious guttural pouch pathology on endoscopic evaluation combined with negative guttural pouch lavage qPCR is recommended to remove a horse from quarantine.1 To prevent contamination of the environment, it is recommended to aspirate the sample via polyethylene tubing through the instrument channel of a 1-meter endoscope.5,6 The endoscope should be sterilized after and between sampling of suspect horses.
SEROLOGY. Serologic testing involves the use of ELISA to detect the SeM protein. Serology is useful for detecting recent but not current infection; assessing the need for vaccination; identifying horses that may be predisposed to purpura hemorrhagica; and diagnosing S.
equi-associated purpura hemorrhagica and metastatic abscessation (SeM titers often are = 1 : 12,800 but have been seen as low as 1 : 3200 and 1 : 6400 in confirmed cases).1,10 It has been suggested that horses with high serum SeM-specific antibody titers (≥1 : 3200) may be predisposed to developing purpura hemorrhagica when
FIG. 31.27 Infusing 50 mL of 0.9% saline for a nasopharyngeal wash on a sedated horse with a uterine pipette. The pipette is punctured through one side of the rectal sleeve.
vaccinated against S. equi.1 A 2009 study reported safely vaccinating horses with SeM titers of 1: 160013 or less with the Pinnacle® I.N. (Zoetis, Parsipanny, N.J.) vaccine. A 2017 study suggested that horses should be tested with the SeM serology for 1 year after a strangles outbreak to determine when it is safe to vaccinate.14
The Animal Health Trust in the United Kingdom has developed a combined serologic test that detects two surface antigens, Antigen A (SEQ_2190 N-Terminal Fragment) and Antigen C (SeM N-Terminal Fragment), and has similar sensitivity but greater specificity when compared to the whole SeM antibody titer.15 This test can be used to identify unvaccinated horses with strangles exposure as recent as 2 weeks previously and to identify animals without clinical signs that may be carrying S. equi for the purposes of isolation and further evaluation via endoscopic guttural pouch examination.1,15,16
VACCINATION. Most horses develop a solid immunity during recovery from strangles, which persists but wanes in more than 75% of animals for up to 5 years as long as the animal was not treated with antimicrobials during the primary infection. This indicates that stimulation of a high level of immunity is biologically feasible given appropriate presentation of protective immunogens. There is evidence that immunity in horses resistant to reinfection is mediated at the mucosal level and functions to block entry of S. equi. However, systemic immunity after parenteral inoculation of avirulent live S. equi is also protective. Together these findings indicate that optimum immunity may require both systemic and mucosal responses.
Vaccine should be administered only to healthy nonfebrile animals free of nasal discharge. Although controversial, vaccination should be considered only in horses with no known contact with animals with strangles during an outbreak.1 The American Association of Equine Practitioners (AAEP) Infectious Disease Committee does not recommend vaccination during an outbreak due to the increased risk of purpura hemorrhagica.
USE OF EXTRACT VACCINES. Extract vaccines (Strepvax II [Boehringer Ingelheim Vetmedica, Inc., St. Joseph, Mo.]) are given intramuscularly and elicit serum antibody responses 7 to 10 days later. Naive horses and foals require a schedule of two or three doses at an interval of 2 weeks. Booster doses are given once annually. Pregnant mares may be boostered a month before the expected date of foaling. Extract vaccines have been associated with cases of purpura hemorrhagica.17
USE OF ATTENUATED LIVE INTRANASAL VACCINE. Attenuated live vaccine (Pinnacle I.N. [Zoetis, Parsipanny, N.J.]) is given in a schedule of two doses at 2- to 3-week intervals. Annual booster doses are recommended. The mode of application should be such that an adequate amount of vaccine reaches the pharyngeal and lingual tonsils but does not enter the trachea. Careful handling of live vaccine is recommended to prevent inadvertent injection intramuscularly via either the vaccine directly or contamination of other vaccines given at the same time. A temporary pharyngitis is possible secondary to administration of this vaccine, and it is not recommended in horses younger than 1 year of age because of the possibility of them developing vaccine-associated clinical disease.18
FUTURE VACCINES. It is likely that more effective and safer vaccines will be developed based on genomic sequence information from S. equi and other Streptococcus species, and there is a need for vaccines that are DIVA (differentiating infected from vaccinated animals) in order to identify recently infected horses from those already vaccinated via serology. Recent experimental trials in Europe have evaluated the use of recombinant multicomponent subunit vaccines that may be promising for broader clinical applications in the future.19,20
CONTROL OF OUTBREAKS. Most outbreaks are thought to originate from introduction of an infected horse to a naive population. All new horses should be isolated for 3 weeks and monitored for any signs of disease, including fever. Many farms with repeated infections have resorted to screening for infection via a single endoscopic evaluation and PCR testing of guttural pouch lavages, a procedure considered by many as the “gold standard” for carrier detection.5,6 A series of three nasopharyngeal swabs, collected 1 week apart, will result in detection by a positive culture on at least one of the swabs in only 60% of carrier animals. Concurrent testing of these swabs by PCR increases the likelihood of detection to more than 90% of carrier animals.6
A practical disease-control strategy should then be agreed on and implemented. The general aims and measures for such a strategy are outlined in Table 31.9, and a flow chart is shown in Fig. 31.28.1,21
■ Treatment The goal of treating strangles is to control transmission and eliminate infection while providing future immunity to the disease. Appropriate treatment of horses with strangles usually depends on the stage and severity of the disease, and veterinary opinion as to whether to use antibiotic treatment remains markedly divided.22
HORSES WITH EARLY CLINICAL SIGNS. During an outbreak, immediate antibiotic therapy for new cases in the early acute phase with fever and depression may be curative and may prevent focal abscessation and shedding. Because abscesses have not developed at this early stage, the antibiotics have adequate access to the bacteria. Immediate treatment of horses that show the earliest clinical sign, fever, could be an effective way of controlling strangles outbreaks in racing stables or riding barns, although the disadvantages of treatment should be weighed.1
■ TABLE 31.9
Aims and Measures Used to Control Transmission of Streptococcus equi on Affected Premises
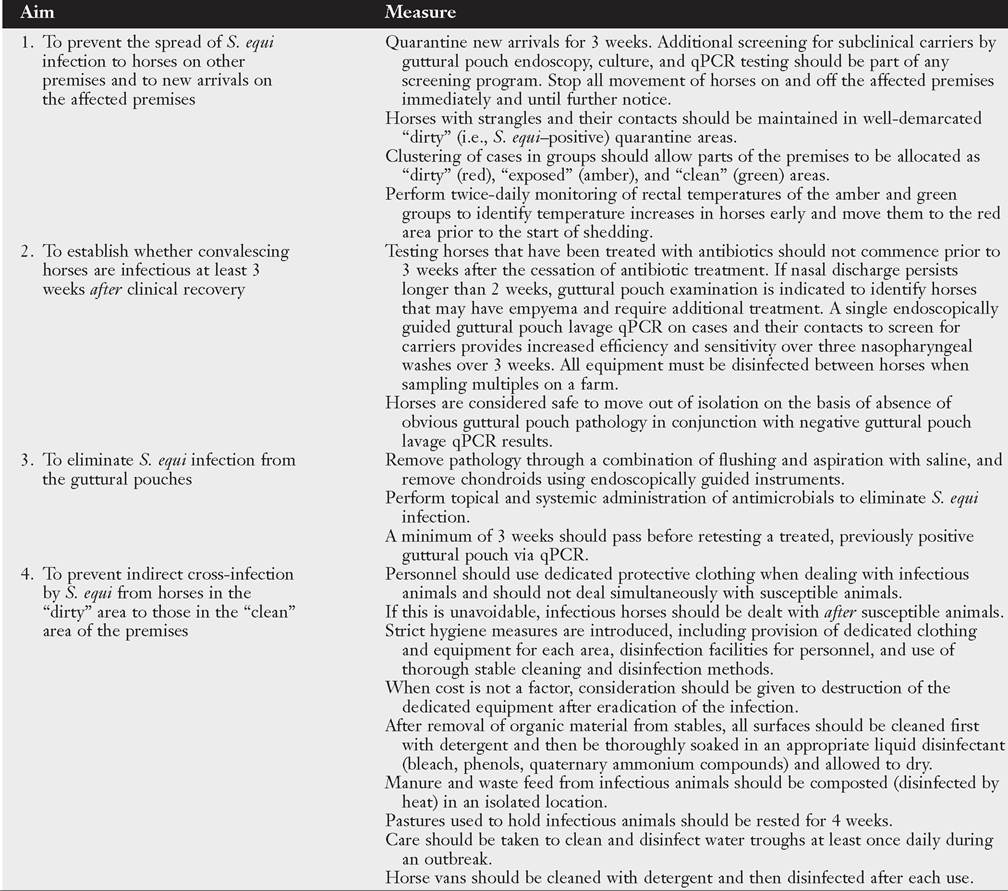
qPCR, Quantitative polymerase chain reaction.
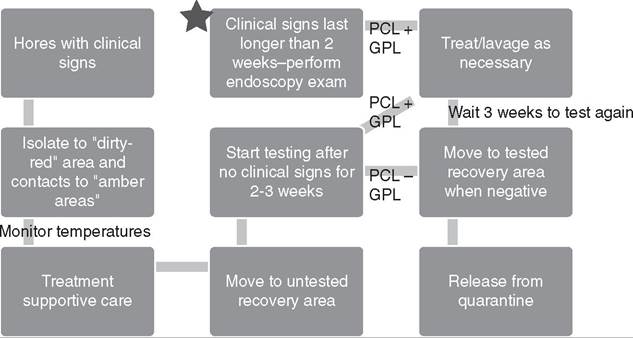
FIG. 31.28 Flow chart of recommended steps in the management of an outbreak of Streptococcus equi. Briefly, horses that present with clinical signs of strangles will be isolated to a “dirty” or “red” zone and all of these horses’ contacts should be in placed in an “amber” zone. Temperatures are monitored, and horses are moved to the “dirty” zone if the temperature is 101.3° F (38.5° C) or higher. Supportive care and treatment of affected animals should be provided. Once clinical signs have resolved in affected horses, they are moved to a recovery area for untested horses. It is recommended that guttural pouch endoscopy and S. equi polymerase chain reaction (PCR) and culture combination testing of the guttural pouch lavage (GPL) should start a minimum of 2 to 3 weeks after the resolution of clinical signs. If a horse is positive on GPL or has an abnormal endoscopy, copiously lavage the guttural pouch and treat with topical and possibly systemic antibiotics. If the GPL is negative, move the horse to a tested recovery area (“green” zone). If a horse remains clinical for longer than 2 weeks, perform a guttural pouch examination at that time to determine if the horse has significant empyema and requires lavage to remove physical contamination of the pouch in order to shorten time to resolution.20
HORSES WITH LYMPH NODE ABSCESSATION. Uncomplicated cases of strangles are often left to run their course with supportive care, providing lasting immunity. Affected horses should be isolated in a clean, dry stall and fed moist, palatable food. NSAIDs should be used judiciously to decrease swelling and promote eating. Hot compresses or topical 20% ichthammol can be used to accelerate maturation of abscessation. Mature external abscesses should be lanced to allow drainage, followed by daily lavage of open abscesses using dilute povidone-iodine solution. This speeds resolution of abscessation as well as alleviation of compression of the pharynx.
Although the use of antimicrobials for treating strangles is controversial, if the horse is febrile, depressed, anorectic, and particularly if manifesting dyspnea, antibiotic therapy is indicated to decrease abscess size and prevent complete airway obstruction. In rare cases, affected horses may require intensive supportive therapy, including IV fluids, feeding by nasogastric tube, and tracheostomy. An animal requiring a tracheostomy should be given systemic antimicrobial drugs to prevent secondary bacterial infections of the lower respiratory tract.
DRUGS OF CHOICE FOR THERAPY. Penicillin G (procaine penicillin [22,000 to 44,000 IU/kg IM q12h] or aqueous potassium penicillin [22,000 to 44,000 IU/kg IV q6h]) is considered the drug of choice for the treatment of nonpneumococcal streptococcal disease, with alternative drugs used depending on ease of administration or the site of infection. Other agents for therapy include cephalosporins and macrolides. Anecdotally, trimethoprim-sulfadiazine treatment failure has been seen, and there are no studies determining its effectiveness against S. equi.23 Use of antimicrobials during any phase of the disease may prevent the development of lasting immunity.
Complications
GUTTURAL POUCH EMPYEMA AND CARRIER STATUS. The percentage of carriers per outbreak could be as high as 10%. Endoscopic examination is required for identification of guttural pouch empyema. The SeM ELISA and the combined indirect ELISA (iELISA) do not detect empyema or carrier status.5 Elimination of guttural pouch empyema requires repeated lavage with a solution of 20% acetylcysteine in buffered saline via polyethylene tubing through an endoscope or via a Chambers catheter. Chondroids are particularly difficult to remove, possibly requiring manual removal with endoscopic equipment such as a memory helical polyp retrieval basket, repeated lavage via indwelling catheters, or surgical removal. Successful elimination of S. equi in these carriers requires local treatment of the guttural pouch with a penicillin gel after removal of the material within the guttural pouch in addition to systemic treatment with procaine penicillin or potassium penicillin for 7 to 10 days. Eradication of this disease will not be possible until the subpopulation of carriers is eliminated.24
COMPLICATIONS ASSOCIATED WITH METASTATIC SPREAD OF INFECTION. S. equi spreads hematogenously or lymphatically, resulting in metastatic abscessation that can affect any organ system in 2%25 to 20%26 of cases. Aspiration of mucopurulent discharge or hematogenous or lymphatic spread to the lungs can cause pneumonia. Abscessation in the mesentery, liver, spleen, and kidneys is common, leading to peritonitis and clinical signs of colic. Abscessation of the cranial mediastinal lymph nodes can cause tracheal compression and respiratory distress. Neurologic signs are present when abscessation occurs in the brain.1 The mortality rate of horses with strangles is less than 2%, but the presence of bastard strangles can increase the mortality rate to as high as 62%.27,28 Attempted culture and sensitivity from the affected body cavity provides direction for the appropriate antibiotic treatment, which has included penicillin, ceftiofur, chloramphenicol, and doxycycline. An average of 2.5 months of antibiotic treatment was needed for resolution.27 Some horses have been treated via surgical drainage along with systemic antibiotics.28
PURPURA HEMORRHAGICA. Purpura hemorrhagica is an aseptic necrotizing vasculitis that can occur in mature horses after repeated natural exposure to infection or after vaccination of horses that have had strangles. The actual incidence of this type III hypersensitivity response secondary to strangles or vaccination is unknown. Clinical signs range from mild to life-threatening, including pitting edema of the head, trunk, and distal limbs, as well as petechiae and ecchymoses. In some cases, antigen-antibody complexes affect other sites, including
the GI tract, muscles, lungs, myocardium, and kidneys. In addition to prolonged treatment with penicillin, cases of purpura hemorrhagica also require the use of systemic corticosteroids (dexamethasone, 0.1 to 0.2 mg/kg IV or IM q12-24h; prednisolone, 0.5 to 1 mg/kg PO q24h) for an average of 3 weeks to reduce systemic vasculitis.13 Significant rhabdomyolysis with progressive atrophy has been identified in some Quarter Horses, after exposure to S. equi, without other signs of purpura.17