Acute Respiratory Distress Syndrome and Acute Lung Injury (Acute Bronchointerstitial Pneumonia)
Bettina Dunkel
■ Definition and Pathophysiology Acute respiratory distress syndrome (ARDS) describes a condition of severe pulmonary dysfunction and respiratory failure caused by physical or chemical injury or an exaggerated pulmonary immune response.
In human medicine, the current definition, the so- called Berlin definition, defines ARDS as respiratory distress that is acute in onset (within a week of a known insult) and combined with the presence of bilateral pulmonary opacities and respiratory failure not fully explained by cardiac failure or fluid overload. Based on the degree of hypoxemia, measured by the ratio of partial arterial oxygen pressure (PaO2) to fraction of inspired oxygen (FiO2), three severities of ARDS are differentiated: mild (PaO2ZFiO2 >200 and ≤300 mm Hg), moderate (>100 and ≤200 mm Hg) and severe (≤100 mm Hg).1-3In the first definition from 1994, the term acute lung injury (ALI) was used to describe a less severe form of the disease, now corresponding to the mild form of ARDS.4 This term is no longer used in human medicine. It still features in the current definitions for veterinary acute lung injury (VetALI) and veterinary acute respiratory distress syndrome (VetARDS) that were developed during a consensus meeting predating the Berlin definition (Box 31.1).5 Due to lack of available data, no species-specific definitions were established, but the physiologic differences in arterial oxygenation in foals younger than 1 week of age were addressed by introducing different inclusion criteria for this age-group (Table 31.10). The consensus definition also acknowledged the disease presentation in neonatal foals, with presumed pulmonary surfactant deficiency (called neonatal equine respiratory distress syndrome) secondary to very early gestational age, induction of parturition, or cesarean section as an entity distinct from VetALI and VetARDS.5
■ BOX 31.1
Veterinary Acute Lung Injury (VetALI) and Veterinary Acute Respiratory Distress Syndrome (VetARDS)
At least one each of the first four criteria must be met; criterion 5 is recommended but optional (Wilkins et al., 2007).
1. Acute onset (1 quadrant/lobe)
b. Bilateral dependent density gradient on computed tomography
c. Proteinaceous fluid within the conducting airways
d. Increased extravascular lung water
4. Evidence of inefficient gas exchange (any one or more of the following):
a. Hypoxemia without PEEP or CPAP and known FiO2
i. PaO2ZFiO2 ratio
1. ± 2.7 mm Hg
■ Clinical Signs and Differential Diagnoses Clinical signs include profound depression, fever and respiratory distress with tachycardia, tachypnea, nostril flare, and cyanotic mucous membranes. Auscultation of the lungs can reveal a variety of abnormal sounds or complete silence over nonventilated areas. Clinically it is almost impossible to differentiate foals with VetALI and VetARDS from foals with severe bacterial, chiefly advanced R. equi, pneumonia, particularly as the syndrome can be triggered by an underlying bacterial infection.
■ Clinical Pathology and Necropsy Findings Laboratory findings include severe hypoxemia with hypocapnia or hypercapnia and, depending on the underlying disease process, leukocytosis or leukopenia and hyperfibrinogenemia. Abnormal coagulation parameters may be observed, and signs of disseminated intravascular coagulation were present in two foals with VetALI and VetARDS in one report.21 Transtracheal lavage fluid demonstrates neutrophilic inflammation with or without signs of infection, depending on the underlying cause.
Thoracic radiographs show a diffuse, dense bronchointerstitial pattern often coalescing to a focal or diffuse alveolar pattern with prominent air bronchograms. The initial radiographic appearance of the lungs may worsen dramatically within hours due to rapid progression of pulmonary edema. On the other hand, absorption of the alveolar fluid may result in impressive improvement of the radiographic appearance within days.21,22 A thoracic sonogram is useful in foals that cannot be safely transported to a radiography unit and reveals multiple coalescing comet-tail artefacts predominately in the caudodorsal lung field.On gross pathologic examination, the affected lungs are wet and firm and fail to collapse, and airways contain variable amounts of pink, foamy liquid. Histologically, necrosis of alveolar and terminal bronchial epithelium is observed with extensive filling of the alveolar spaces with neutrophils, macrophages, hemorrhage, protein-rich edema fluid or hyaline membranes. Occasionally microthrombi can be detected in interstitial capillaries. In more chronic cases, diffuse proliferation of cuboidal pneumocytes and fibroblasts and beginning fibrosis may be present.19-22
■ Diagnosis The diagnosis can be established if the criteria outlined in Box 31.1 and, depending on the age, Table 31.10 are met, cardiac disease is absent, and the extent of the respiratory distress cannot be attributed solely to a primary disease process (e.g., almost complete destruction of the pulmonary parenchyma by a primary disease process). CT has been described in heathy foals and will allow more detailed assessment of lung pathology.33,34 However, risks and benefits of the procedure need to be carefully assessed in these precarious patients. Presence of bacterial or viral pneumonia does not rule out concurrent VetALI or VetARDS.
■ Treatment and Prognosis A recent reduction in mortality in human ARDS has largely been attributed to more widespread use of lung-protective ventilation with lower tidal volumes (6 mL/kg) and airway pressures and conservative fluid therapy.35 Antiinflammatory, antioxidant, anticoagulant, and surfactant therapy and treatment to enhance alveolar edema removal (aerosolized or intravenous β-adrenergic agonists such as salmeterol, terbutaline, or epinephrine to stimulate active transepithelial ion transport) have largely failed to improve survival.7 A recent meta-analysis showed promise for antiplatelet drugs, including clopidogrel, but whether this will be confirmed in future studies remains to be seen.36 However, considering that, in contrast to human medicine, most equine patients die as a direct result of respiratory failure, some of those therapeutic options may still benefit the equine patient.
Because mechanical ventilation is, with few exceptions,37 feasible only in neonates, the most important treatment remains intranasal insufflation of humidified oxygen via unilateral or bilateral intranasal cannulas. Large-bore tubing systems minimize the resistance to airflow, and FiO2 as high as 70% and 75% has been measured at the carina in adult horses and foals, respectively, using bilateral flow rates of 15 L/min (10 L/ min in foals; combined 30 L/min in adults or 20 L/min in foals).38,39 Alternatively, use of intratracheal oxygen insufflation has been described, achieving results similar to high bilateral intranasal flow rates.40 Administration of methylprednisolone at 1 to 2 mg/kg/day is much debated but still frequently used in acute cases of human ARDS for up to 2 weeks, followed by a gradual decrease of the dose. Considering that ventilation is rarely an option and that in two reports all but two foals surviving ARDS received corticosteroids, anecdotal evidence is in favour of steroid administration (IV prednisolone sodium succinate or methylprednisolone at 1 to 2 mg/kg/day divided in 2 to 4 doses). Antimicrobial treatment, if required, should be directed against the underlying disease process. Bronchoconstriction is not a prominent feature of ARDS, and therefore bronchodilators are most likely of limited use. Care should be taken when administering bronchodilators, as they can induce sudden worsening of V/Q mismatching and can lead to acute decompensation of the severely hypoxic patient. Judicious IV fluid therapy may be necessary in dehydrated patients, but overhydration or rapid changes in circulating blood volume should be avoided, as capillary hydrostatic pressure is the main determinant of pulmonary edema formation when endothelial and epithelial permeability is increased. On the other hand, a suboptimal hydration status decreases cardiac output and worsens oxygen delivery to the peripheral tissue. Measurement of central venous pressure may aid in determining the patient's hydration status. If foals are too depressed to nurse or eat, nutritional support is essential.Based on the limited information available, the prognosis for survival and future athletic performance is guarded, with survival rates ranging from 60% to 69% in two clinical reports.21,22 It is difficult to extrapolate long-term outcomes of pulmonary function from human patients due to the extensive use of mechanical ventilation with associated injury and the frequent presence of preexisting morbidities such as smoking.41 Experimental induction of ARDS in horses did not result in any lasting histologic changes or fibrosis despite severe clinical signs.30 The few long-term reports of equine survivors have so far suggested little noticeable lasting respiratory compromise, and successful careers as racehorses have been reported even in severely affected animals. More information is clearly needed to determine the long-term effects of severe pulmonary injury in horses.
Interstitial Pneumonia and Endogenous and Toxic Conditions
■ BOX 31.2
Causes of Interstitial Pneumonia in Horses
Acute
Infections (systemic viral, bacterial, parasitic)
Inhaled chemicals
Oxygen (FiO2 >50%)
Smoke
Ingested toxins or precursors
Perilla mint (Perilla frutescens), Crofton weed (Eupatorium adenophorum), Crotalaria spp., Senecio spp.
Adverse drug reactions
Uncertain
Hypersensitivity
Acute hypersensitivity pneumonitis
Endogenous metabolic or toxic conditions
Shock—particularly endotoxic (acute respiratory distress syndrome, or ARDS)
Disseminated intravascular coagulation (DIC)
Uremia
Idiopathic or cryptogenic
Chronic
Infections (systemic viral, bacterial, parasitic)
Inhaled inorganic dust (pneumonoconioses)
Silicosis
Hypersensitivity
Hypersensitivity pneumonitis
Ingested toxins or precursors
Perilla mint (P frutescens), Crofton weed (E. adenophorum), Crotalaria spp., Senecio spp.
Collagen-vascular disorders
Uncertain
Idiopathic or cryptogenic

FIG.
31.29 Cut section of lung from a horse with equine multinodular pulmonary fibrosis (EMPF). Note the large areas of fibrous tissue within the pulmonary parenchyma. (Courtesy Dr. Fabio Del Piero, Louisiana State University, Baton Rouge, La.)be associated with a nodular form of interstitial pneumonia of horses characterized by pulmonary interstitial fibrosis, suggesting that these rather unusual cases may have an underlying infectious etiology.9-11 This disease has been called equine multinodular pulmonary fibrosis (EMPF) by the authors describing the pathology of the disease (Fig. 31.29). Horses affected generally have a history of fever, cough, and weight loss accompanied by exercise intolerance and finally respiratory distress. They can present as acutely affected animals or as having a more chronic, progressive problem. Typical radiographs reveal multiple discrete to coalescing nodular densities overlying a diffuse interstitial pattern. Histologic appearance is diagnostic of this disease (Fig. 31.30). EHV-5 has been identified in both BAL fluids and lung biopsy samples from affected patients by
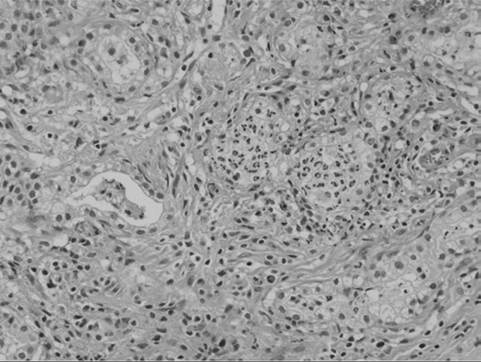
FIG. 31.30 Postmortem histopathology specimen from a horse with severe equine multinodular pulmonary fibrosis (EMPF). This is the histologic appearance of one of the fibrotic nodules. The alveoli are constricted within dense neoformed fibrotic tissue. Alveoli have an abnormal cuboidal epithelium (type 2 pneumocytes), and the lumen contains macrophages, sloughed epithelial cells, and neutrophils. Denser and diffuse fibrotic areas are present. (Courtesy Dr. Fabio Del Piero, Louisiana State University, Baton Rouge, La.)
both PCR and IHC. Influenza infection resulting in severe, fatal interstitial pneumonia in unvaccinated or naive horses and foals has been described in single case reports and as outbreaks.12-14 There is a single report of a fatal pneumonia in a young horse secondary to EHV-1 infection.15 Both adenovirus and equine arteritis virus have been described as causes of severe bronchointerstitial or interstitial pneumonia in foals and adult horses.16-19
In some horses with bronchointerstitial pneumonia of unknown cause, bacterial agents have been isolated from the lung. The usual distribution of bacterial bronchopneumonia in the horse is cranioventral, frequently associated with transportation, whereas the distribution in interstitial pneumonia is diffuse. In the latter cases the bacteria may be either opportunistic or primary pathogens and may not represent the primary causative agent.20,21 An exception is R. equi pneumonia of foals, which can cause ARDS in older foals. R. equi has been cultured from foals with severe, acute bronchointerstitial pneumonia with a diffuse pulmonary distribution.22 Interstitial pneumonia associated with P carinii has been described in the foal, and Mycoplasma spp. have been isolated from the respiratory tract of adult horses.23-25 The significance of the Mycoplasma isolates remains a matter of debate.25 P carinii pneumonia is thought to occur primarily in immunocompromised foals as a complication of some other serious disease, such as infectious pneumonia or SCID. It is characterized by a plasmacytic, lymphocytic interstitial pneumonia with flooding of alveoli with foamy acidophilic material.
Parasitic pneumonia, an uncommon cause of chronic bronchointerstitial pneumonia, usually occurs in young foals secondary to migration of Parascaris equorum larvae through the pulmonary parenchyma.26
INGESTED CHEMICALS. Ingested chemicals rank second only to infectious agents as potential causes of interstitial pneumonia in horses. Ingestion of pyrrolizidine alkaloids from a variety of plants (mostly genera Crotalaria, Trichodesma, and Senecio) can cause interstitial pneumonia in horses.27 This toxicity is associated with production of a toxic metabolite activated in the liver that then circulates to the lung. The toxic alkylating agents damage capillary endothelial cells, although the amount of alkyloid required to damage the lung is generally less than that required for hepatotoxicity. Crofton weed (Eupatorium adenophorum), a poisonous plant found primarily in Australia and Hawaii, produces interstitial pneumonia in horses.28 Toxicity is associated with ingestion of the flowering plant, but the nature of the toxin is not known. Perilla ketone, derived from the plant Perilla fructans, produces acute respiratory distress within 1 week of ingestion in ponies.29 The lesions include diffuse alveolitis and Type II pneumocyte proliferation with sparing of the bronchioles. Toxicity depends on additional metabolism of the 3-substituted furan by the mixed function oxidase system, which occurs directly in the lungs of the horse.
INHALED CHEMICALS. Direct pulmonary injury by inhaled chemicals is an uncommon cause of interstitial pneumonia in horses. In humans this type of pneumonia is primarily related to occupational exposure. Smoke inhalation causes acute, diffuse interstitial pneumonia in horses, frequently followed within a few days by opportunistic bacterial pneumonia.30 Oxygen toxicity can theoretically produce interstitial pneumonia and alveolar Type II cell proliferation. This problem is more likely to be seen in neonatal foals mechanically ventilated with increased levels of oxygen (FiO2 >50%) for several days, although this may in fact be a form of ventilator-associated lung injury (VALI) related to mechanical stretch of the airspaces. Damage is thought to be due to production of reactive oxygen metabolites, which attack a lung that may already have been injured by barotrauma, resulting from a ventilator-driven increase in airway pressure. Agrichemicals or herbicides, such as paraquat, may cause acute interstitial pneumonia (AIP) in horses and should be considered in horses with a history of possible exposure.31 Silicosis is a specific chronic granulomatous pneumonia of horses associated with inhalation of silicon dioxide crystals.32 This syndrome has been described in horses originating from the Carmel Valley region of California. The inhaled particles are ingested by alveolar macrophages and result in lysis of the macrophage, chronic alveolitis, and fibrosis. Multiple granulomas are present, and submicron intracytoplasmic crystalline particles can be identified in macrophages.
HYPERSENSITIVITY REACTIONS. In the most specific sense, hypersensitivity pneumonitis refers to pulmonary disease caused by inhalation of organic antigens. Lymphocytic, plasmacytic bronchitis and bronchiolitis, combined with lymphocytic interstitial pneumonia, characterize the disease in the horse lung. Granuloma formation and fibrosis can be observed. Chicken dust and fungi have been implicated as a cause of severe, chronic bronchointerstitial pneumonia, but the syndrome itself is quite rare.
ENDOGENOUS METABOLIC AND TOXIC CONDITIONS. A variety of conditions cause acute pulmonary injury with inflammatory edema or severe alveolar wall damage and serofibrinous exudation similar to that described for AIP. Acute uremia, shock, burns, and trauma can produce an acute pulmonary injury called acute lung injury (ALI) or acute respiratory distress syndrome (ARDS), depending on severity. Although endotoxin does not directly injure the lung, endotoxemia in the horse initiates inflammatory and metabolic cascades that can lead to pulmonary injury. Activation of these pathways produces vasoactive and chemoattractant molecules that increase vascular permeability, activate complement, produce proinflammatory cytokines, and release neutrophil enzymes that can adversely affect the lungs of horses. Horses, as a species, are quite sensitive to the negative effects of endotoxemia, and their lungs are particularly sensitive, perhaps due to the presence of intravascular macrophages, which further amplify the inflammatory cascade. Both ALI and ARDS have been defined for veterinary patients but require updating.33
■ Pathophysiology Interstitial pneumonia progresses through four phases.7,11,34 During the first phase, the initial insult causes parenchymal injury and alveolitis. This is followed by a proliferative phase characterized by cellular and parenchymal alterations in tissues of the lung. Chronic cases progress to the development of interstitial fibrosis, and the final stage results in end-stage irreparable fibrosis of the lung.
The structural changes that occur in the lung reduce the number of functional alveoli, adversely affecting ventilatory function of the lung and altering V/Q relationships. There is reduced lung compliance associated with the loss of distensible alveoli, presence of pulmonary edema, and fibrosis. Total and vital lung capacity are decreased in association with the loss of functional gas exchange units and reduced lung compliance. The work of breathing is increased, resulting in exercise intolerance and difficulty breathing. Pulmonary hypertension and cor pulmonale may present as complications of interstitial pneumonia and fibrosis. Although the origin of pulmonary hypertension is unclear, hypoxic vasconstriction and generation of vasoactive compounds (such as endothelin-1) that alter pulmonary vascular resistance acutely, and vessel anatomy chronically, may play a role.
■ Clinical Signs Horses affected with interstitial pneumonia frequently present with fever, cough, weight loss, nasal discharge, exercise intolerance, severe dyspnea, cyanosis, and a restrictive breathing pattern. A “heave line” may be present; nostril flare and an anxious expression are usual. The history can be acute or chronic. Although affected foals are frequently depressed and anorectic, adults may be bright and alert with a variable appetite. The disease proceeds toward death in many cases, with progressive respiratory compromise, although some may also slowly improve with time. More than one foal at a farm may be affected.
■ Diagnosis In older horses, the primary differential diagnosis of RAO may be excluded by the leukocytosis and hyperfibrinogenemia that commonly occurs in horses with interstitial pneumonia and fibrosis but does not occur in horses with heaves. However, these abnormal features are common in horses with infectious bronchopneumonia, and thoracic radiography is of paramount importance in establishing a definitive diagnosis. Typically, thoracic radiographs reveal extensive interstitial and bronchointerstitial pulmonary patterns (Fig. 31.31). Nodular infiltrates, either large or miliary, may be present but are always diffusely distributed.
Culture of transtracheal or BAL aspirates often yields no significant growth of viral, bacterial, or fungal pathogens. Cytologic evaluation of tracheal or BAL fluid shows increased numbers of neutrophils and macrophages. If P carinii is involved, BAL fluid may reveal trophozoites or intracystic bodies with special stains, such as toluidine blue or methenamine silver. Using PCR, EHV-5 has been found in BAL fluid from horses with EMPF.9 EHV-5 PCR has been found to be closely associated with EMPF in BAL fluid or a combination of whole blood and nasal secretions.35
Histologic examination of a transthoracic lung biopsy specimen is the definitive diagnostic test for chronic interstitial pneumonia and fibrosis and for EMPF (see Fig. 31.30). Care must be taken to ensure that the biopsy is obtained from a representative area, and ultrasound guidance has been useful in the hands of the author. Clinically important complications from this technique are uncommon but can occur. Biopsy can both define the causative agent and confirm the clinical diagnosis in EMPF when evaluated for EHV-5.
Additional diagnostics could include arterial blood gas analysis, abdominocentesis, and thoracocentesis to rule out metastatic neoplastic disease; pulmonary function testing; viral isolation; serologic testing for antibody to fungi and chicken serum if hypersensitivity pneumonitis is suspected; and immunohistochemical evaluation of lung tissue for suspected infectious agents. A complete cardiac evaluation should also be conducted, as pulmonary hypertension and cor pulmonale are not uncommon sequelae.
■ Treatment Treatment of these cases is often unrewarding. Therapeutic goals are (1) treatment of any underlying or secondary infection; (2) suppression of inflammation; (3) maintenance of tissue oxygen delivery within appropriate limits; (4) relief of any associated bronchoconstriction; and (5) prevention or treatment of complications. Environmental management, with appropriate temperature and humidity control and good ventilation, is beneficial.
Parenteral corticosteroid therapy is the mainstay of treatment, with early and aggressive therapy providing the best long-term outcome, particularly in foals. In one report of 23 foals affected with acute bronchointerstitial pneumonia, 9 of 10 treated with corticosteroids survived, whereas none of those not receiving steroid treatment lived.4 Foals with a diagnosis of ARDS have the best prognosis when treated with corticosteroids and antimicrobial therapies as indicated by diagnostics.36
Broad-spectrum antimicrobial treatment should be instituted initially, particularly in foals, as described for the treatment of infectious bronchopneumonia. The choice of antimicrobial and duration of therapy should be dictated finally by the culture and sensitivity results from the transtracheal aspirate and by the patient's clinical course. Anecdotally, horses with EMPF have responded to treatment with acyclovir or other antiviral agents and corticosteroids. The course of therapy is generally prolonged, 6 to 12 weeks; clinical and radiographic improvement has been noted in a few cases to date.
Foals, in particular, and adults with severe respiratory distress may benefit from nasal insufflation of humidified oxygen, with flow rates of 5 to 15 L/min for foals and 15 L/min for adults.37 If necessary, as determined by persistent hypoxemia in the face of intranasal insufflation at the rates given, a second nasal canula can be placed in the opposite nostril to increase the FiO2. Care must be taken to avoid obstruction of the nasal passages. Alternatively, intratracheal or transtracheal insufflation can be considered to further increase FiO2 and improve oxygenation (see Fig. 31.31).38
Systemic bronchodilator therapy may or may not be indicated in these cases. If used, bronchodilators may worsen V/Q inequalities. Thus bronchodilator therapy should be accompanied by supplemental oxygen, and the effects should be monitored with serial blood gas measurements and discontinued if hypoxemia worsens. Nebulized or aerosolized bronchodilator therapy may be more judicious, and beneficial effects are evident in some foals with respiratory distress. Aminophylline and theophylline should not be used due to their narrow therapeutic range. Furosemide may be appropriate for its bronchodilator effect and its effect on reducing pulmonary artery pressure, particularly if cor pulmonale develops.
■ Prognosis The prognosis of interstitial pneumonia in horses is generally poor to guarded. Affected foals, when treated early and aggressively with corticosteroid and antimicrobial therapy, have the best outlook for life. The disease is usually progressive in adults and eventually results in the demise of the horse, although the occasional horse recovers sufficiently to return to previous performance levels. A fair number of adult horses, with continuous intense management, will live for a period but be severely compromised,. Exceptions to the poor prognosis may be seen in cases of P. carinii and parasitic pneumonia in foals if they are treated early and aggressively and, possibly, also in cases of idiopathic interstitial pneumonia/ EMPF in adult horses that are treated early with corticosteroids and antivirals. A trial of treatment for peracute interstitial disease for 48 hours is warranted, and chronic interstitial pneumonia should be treated for a minimum of 6 weeks before discarding the possibility of recovery.