Fungal Infections of the Equine Respiratory Tract
AUison Jean Stewart
■ Definition and Etiology Fungi are eukaryotic organisms with a definitive cell wall made up of chitins, glucans, and mannans. Within the fungal cell wall, the plasma membrane contains ergosterol, a cell membrane sterol that is frequently targeted by antifungal agents.
There are more than 70,000 species of fungi, but only 50 species are known to cause disease in people or animals. Pathogenic fungi can be divided into three groups: multinucleate septate filamentous fungi, non- septate filamentous fungi, and yeasts. Dimorphic fungi are able to interchange between forms depending on environmental conditions. Examples of dimorphic organisms include Blastomyces dermatitidis, Histoplasma capsulatum, and Coccidioides immitis, which exist in yeast form in vertebrate host tissue and in hyphal or mycelial form in vitro. In soil and decaying matter, the mycelial form usually is present and is composed of a collection of hyphae. The mycelia produce infective spores that are capable of inoculating vertebrate tissue.Fungal infections in horses are relatively uncommon, although geographic prevalence is highly variable. Fungi are ubiquitous, and their constant aerosol exposure to respiratory tissue is inevitable. Upper respiratory and pulmonary disease caused by fungi is frequently acquired by the inhalation route, with the sporular diameter small enough to allow penetration into the distal airways and alveoli. In most samples of stable air, more than 90% of particles visible under a light microscope are spores of fungi or actinomycetes.1 One study found that if a horse stood quietly in its stable without access to hay, the mean concentration of dust was very low (approximately 12 particles∕cm3 [of particles less than 5 mm in diameter]). When the bedding was disturbed during the normal “bedding down” operation, the concentration of respirable dust increased sixfold.2 Systemic fungal infections and some cases of fungal pneumonia are thought to arise through a compromised GI tract, by inhalation, or via open wounds.
Tissue invasion of pulmonary tissue usually occurs in the immunocompromised host, although on occasion the normal individual may be affected. Important predisposing factors for fungal pneumonia include (1) qualitative and especially quantitative granulocyte abnormalities and (2) the presence of devitalized tissue. In most cases of upper respiratory tract fungal granuloma, there are no obvious predisposing causes.
Primary pathogenic fungi such as B. dermatitidis, H. capsu- latum, C. immitis, Cryptococcus neoformans, and Conidiobolus coronatus usually infect immunologically normal horses. However, in a report of cryptococcosis in seven horses, five had a history of illness that may have predisposed them to cryptococcosis.3 A separate group of fungal pathogens tends to infect only those equine patients with abnormal host defenses. Opportunistic fungi, including Aspergillus spp., Candida spp., Fusarium spp., Emmonsia crescens, and P. carinii (renamed P jiroveci in humans), have caused fungal disease in horses that are immunocompromised or neutropenic; have neoplasia, colitis, enteritis, or bacterial pneumonia; or have been treated with corticosteroids.4-15 In vitro studies support the critical role of phagocytic cells in host defense against opportunistic fungi.
■ Clinical Signs Mycotic granulomas have been found in nasal passages, paranasal sinuses, nasopharynx, guttural pouch, trachea, bronchioles, lungs, and mediastinum of infected horses. The most common clinical signs of upper respiratory tract fungal infection include unilateral or bilateral serosanguineous or mucopurulent nasal discharge, as well as inspiratory or expiratory noise. Other clinical signs include coughing, facial deformation, and dyspnea caused by partial blockage of nasal passages by granulomatous masses. Differentials for fungal granulomas of the respiratory tract include ethmoidal hematoma, squamous cell carcinoma, amyloidosis, and exuberant granulation tissue.
Fungal plaques in the guttural pouch often are located over the arterial blood supply. Horses with guttural pouch mycosis usually present with episodic serosanguineous nasal discharge that may progress to potentially fatal epistaxis if there is erosion into an artery. The duration of clinical signs can vary from days to many months. Guttural pouch mycosis is discussed in detail later in this chapter.
Pulmonary fungal infections causing granulomas, diffuse pneumonia, or pleuropneumonia can present with signs similar to those of bacterial infection. There may be cough, nasal discharge, tachypnea, respiratory distress, hemoptysis, and, if chronic, weight loss. Radiographic appearance of fungal pneumonia may reveal virtually any infiltrative pattern. Although miliary patterns are occasionally seen, the most common initial finding is a patchy bronchopneumonia. Multiple focal sites are common, and lesions tend to be peripheral in distribution. Differentials include bacterial pneumonia, equine asthma, silicosis, equine pulmonary nodular fibrosis (associated with EHV-5), granulomatous disease complex, and neoplasia.
Systemic infections can have variable clinical signs depending on the location and extent of the infection. Fungal infections can affect multiple organ systems and body cavities. Weight loss, colic, or diarrhea can often occur with infection within the abdominal cavity.
■ Diagnostic Sampling Lesions in the nasal passages, nasopharynx, guttural pouch, trachea, and bronchioles usually can be observed directly during endoscopic examination. Masses in paranasal sinuses and lungs may be observed radiographically. CT or MRI provide detailed imaging of the equine skull (and thorax, depending on the size of the animal and gantry) and can be used to determine the extent of lesions and bony invasion. An 8- to 20-mm trephine (Michelle 8-mm trephine or 14- to 20-mm Galt trephine [Jorgensen Laboratories, Inc., Loveland, Colo.]) can be drilled into the nasal or maxillary sinus, through which a sterile rigid arthroscope or flexible endoscope can then be passed to directly view some lesions within the paranasal sinuses.
For nasal and nasopharyngeal lesions, specimens for cytology, histopathology, and culture can be obtained by using an endoscopically guided biopsy instrument; however, these samples tend to be small, superficial, and often nondiagnostic. Mucosal contaminants may overgrow the organism of interest. Larger biopsy samples from the nasal passages or nasopharynx often can be obtained by using a uterine biopsy instrument (Jorgensen Laboratories, Inc., Loveland, Colo.) passed nasally with visual guidance from a flexible endoscope. Excisional biopsy or surgical debulking may be performed through a sinus flap or via laryngotomy.
Fungal pneumonia may be diagnosed from samples obtained by tracheal wash or bronchoalveolar lavage fluid, or via a lung biopsy. Lung biopsy is associated with significant risk if a large pulmonary vessel is accidentally punctured. The biopsy should be performed ideally after radiographic evaluation or with concurrent ultrasound guidance and should be obtained from the periphery of the lung; however, some horses have experienced fatal hemorrhage associated with puncture of a vessel only 2 cm from the periphery. The lung is rich in plasminogen, so bleeding complications may be severe. Spring-loaded biopsy needles (4-gauge ? 20-cm biopsy needle [Temno Products Group International, Lyons, Colo.] or Magnum biopsy needle) are safer for lung biopsy compared with Tru-Cut biopsy instruments (Cardinal Health, Dublin, Ohio).16 Ultrasound evaluation can be used to monitor for bleeding after the procedure.
CYTOLOGY. Fungal hyphae may be identified in airway fluid or in impression smears obtained from biopsied masses. Clinicians must be careful in attributing significance to presence of fungal elements in a transtracheal aspirate. Fungal hyphae are often present either free or in large mononuclear cells in tracheal aspirates from healthy horses.17 A study of healthy Thoroughbred racehorses showed that 70% had fungal elements detected in their tracheal aspirates without evidence of fungal pneumonia.18 Barn fungus such as Alternaria spp.
are nonpathogenic and rarely incite an inflammatory response in the host. The organisms often have a blocklike appearance and may be colored (Fig. 31.18). A normal predominance of macrophages, lymphocytes, and nondegenerate neutrophils (the expense, or the poor prognosis.Prevention of invasive fungal pneumonia is difficult. It is impossible for the horse to avoid large inhaled inocula, given its environmental conditions. Improving ventilation and minimizing exposure to inspired spores are most beneficial in immunocompromised patients. The most important methods of disease prevention are treating predisposing illnesses promptly and effectively and judiciously avoiding overuse of corticosteroids and broad-spectrum antibiotics.
ANTIFUNGAL THERAPEUTICS (Table 31.6)
Amphotericin B. Amphotericin B deoxycholate is a polyene antibiotic that combines with ergosterol in the fungal cell membrane, resulting in an increase in cell permeability. Intravenous amphotericin B can cause nephrotoxicity and phlebitis. Other possible side effects include anorexia, anemia, cardiac arrhythmias, hepatic and renal dysfunction, and hypersensitivity reactions.36 Amphotericin B also has been used successfully to treat histoplasmosis and pulmonary aspergillosis and cryptococcosis.25,26,37 A high dose of oral amphotericin B successfully treated mucormycosis caused by Absidia corym- bifera.3 Topical amphotericin B has been successful in treatment of nasopharyngeal C. coronatus.y9^n
Azoles. Benzimidazole derivatives in the class azoles, such as miconazole, enilconazole, ketaconazole, itraconazole, fluconazole, and voriconazole, destroy fungi by inhibition of ergosterol biosynthesis in the fungal cell membrane. Azole antifungals inhibit cytochrome P450-dependent 14 α-sterol demethylase, which is essential for the formation of ergosterol. Topical 2% miconazole was used in the resolution of four cases of guttural pouch mycosis43 and as part of successful multimodal therapy against nasopharyngeal Pseudallescheria boydii.4 Enilconazole is not commercially available in the United States but has been used topically in the successful treatment of guttural pouch mycosis.45-47 Aerosolization of 1.2 mg/kg enilconazole q12h in 125 mL saline resolved Scopulariopsis pneumonia.28 Ketoconazole is absorbed poorly in the nonacidified form29 but can be acidified for better absorption (30 mg/ kg via nasogastric tube q12h mixed with 0.2 normal HCl).28
Itraconazole (Sporanox solution [Janssen, Titusville, N.J.]) is absorbed well orally (bioavailability 60%).
A dose of 5 mg/ kg PO q24h maintains concentrations above mean inhibitory concentration (MIC) for susceptible yeasts (Histoplasma spp.■ TABLE 31.5
Characteristic Morphologic Features and Availability of Serologic Tests for Fungal Organisms Reported to Cause Fungal Granulomas in Horses (March 2018)
| Serologic Test | |||
| Cytologic Appearance | Veterinary | ||
| Agent | Tissue Form | Method | Laboratory |
| Cryptococcus | Round, thin-walled, yeastlike fungus (5-10 μm) with a large | Capsular antigen ELISA | $41.00 UT |
| neoformans | heteropolysaccharide capsule (1-30 μm in diameter) that does | (antigen) or latex | $27.00 CU |
| not take up common cytologic stains. Capsule is best stained | agglutination | $23.00 CSU | |
| using Mayer’s mucicarmine stain. Organisms show narrow- | (antigen)26,58,61 | $18.00 UGA | |
| based budding and lack endospores. | $29.50 NMDA $33.00 MDL | ||
| Conidiobolus | Broad, thin-walled, highly septate, irregularly branched hyphae | Immunodiffusion is highly | Serologic |
| coronatus | (5-13 μm in diameter).53,56 Often surrounded by acidophilic | sensitive and specific. | testing not |
| staining glycoprotein antigen-antibody complex known as | Decreasing titer is | widely | |
| Splendore-Hoeppli material. | correlated to disease resolution in horses.51,55 | available. | |
| Pseudallescheria | Hyaline, nonpigmented, septate, randomly branched hyphae | ||
| boydii | (2-5 μm in diameter) with regular hyphal contours. Asexual form has nonbranching conidiophores with terminal conidia. Sexual form in culture has cleistothecium (large, round body) and ascospores.44 | ||
| Cocadioides | Spherules have a double-contoured wall, are variable in size, but | AGID (antibody) for IgM | $27.00 UT |
| immitis | can be large (20-80 μm, up to 200 μm). The mature spherules | and IgG27,77,80,81 | $20.00 CSU |
| (sporangia) contain endospores (sporangiospores) 2-5 μm in | MVista Quantitative EIA | $21.00 CU | |
| diameter. In the environment, mycelium are thick walled with | (antigen) | $43.00 NMDA | |
| barrel-shaped arthroconidia. | $60.00 MDL | ||
| Aspergillosis spp. | Broad (2-4 μm in diameter) septate hyphae with parallel sides | Platelia Aspergillus | $60.00 MDL |
| and acute right-angled branching. | Galactomannan EIA | $27.00 UT | |
| (sandwich immunoassay) | $20.00 CSU | ||
| Some reactivity to | $21.00 CU | ||
| Penicillium, Alternaria, | $48.00 NMDA | ||
| and Paecilomyces. | $105.00 UT | ||
| AGID (antibody) Aspergillosis fumigatus only Aspergillus spp. panel | (send out) | ||
| Blastomyces | Yeasts are spherical (15-17 μm in diameter) with basophilic | AGID (antibody)23 | $27.00 UT |
| dermatitidis | protoplasm and unstained, uniformly shaped refractile walls. | MVista Quantitative EIA | $20.00 CSU |
| Unilateral, broad-based budding is characteristic. Yeasts are often located within multinucleated giant cells. | (antigen) | bgcolor=white>$21.00 CU||
| Histoplasma | Yeasts (2-4 μm in diameter) have a thin, clear halo surrounding a | AGID (antibody)74 | $27.00 UT |
| capsulatum | round or crescent-shaped basophilic cytoplasm. | MVista Quantitative EIA | $20.00 CSU |
| (antigen) | $21.00 CU | ||
| Antigen | $48.00 NMDA $60.00 MDL $80.00 UT | ||
| Acremonium | Mononuclear cells contain single, spherical, intracytoplasmic | ||
| strictum | encapsulated spores 3-5 μm in diameter.5 | ||
| Candida spp. | Ovoid budding yeast cells (2-4 μm in diameter) with thin walls, | ||
| or they can occur in chains that produce septate pseudohyphae when blastospores remain attached after budding division. Filamentous, regular, true hyphae also may be visible. | |||
| Pneumocystis | Trophozoite (yeast form) is a 2- to 5-μm in diameter ameboid | ||
| carinii | with filopodia that attach to the surface of type I pneumocytes. Sporangia (cystic form) are encapsulated spores (4 to 6 μm in diameter) containing 8 uninucleate spores (intracytic bodies).14,15,20,85 | ||
| Fungal serology | Antibody to Histoplasma, Blastomyces, Coccidioides, Aspergillus | $69.00 CU | |
| panel | (AGID) | $68 CSU | |
| The CU panel also includes Cryptococcus antigen | $48.00 NMDA | ||
| Fungal culture | $52.00 CU $30 CSU | ||
| Fungal | Per isolate | $73.00 CU | |
| susceptibility | $168 UT | ||
AGID, Agar gel immunodiffusion; ELISA, enzyme-linked immunosorbant assay; Ig, immunoglobulin.
CSU, Colorado State University, P (970) 297-1281, F (970) 297-0320, http://csu-cvmbs.colostate.edu/vdl/Pages/default.aspx; CU, Cornell University, Animal Health Diagnostic Center, P (607) 253-3900, F (607) 253 3943, http://ahdc.vet.cornell.edu/; MDL, Miravista Diagnostics Laboratory, Indianapolis, Ill., P (317) 856-2681, F (317)-856-3685, http://miravistalabs.com/fungal-infection-diagnostic-testing/; NMDA, New Mexico Department of Agriculture Veterinary Diagnostic Services, P (505) 383- 9299, http://www.nmda.nmsu.edu/vds/; UGA, University of Georgia, College of Veterinary Medicine, P (706) 542-5812, F (706) 583-0843, http://www.vet.uga.edu/idl/tests; UT, University of Tennessee, College of Veterinary Medicine, P (865) 974-5639 (mycology) or 974-5643 (serology), http://www. vet.utk.edu/diagnostic/index.php.
■ TABLE 31.6
Pharmacokinetic Studies of Antifungal Drugs Performed in Horses
| Drug and Relative Cost | Dosage | Source | Susceptible Organisms, Equine Reports, Comments |
| Ketoconazole | 30 mg/kg q12h mixed | LH | Scopulariopsis,28 Coccidioides, Cryptococcus, Candida, |
| $ = Moderate | with 0.2 normal HCl via nasogastric intubation29 | Tablets (200 mg) (Nizoral [Janssen, Raritan, N.J.]) | Malassezia, Histoplasma, Sporothrix, Microsporum, Trichophyton |
| Itraconazole | 5 mg/kg/day solution PO31 | Sporonox solution (10 mg/ | Aspergillus,45,68 Histoplasma, Bastomyces, Coccidioides, |
| $ = Very | (bioavailability 60%, | mL oral or injectable | Cryptococcus, Candida, Paracoccidioides, |
| expensive | compared to 12% for capsules) | solution) Sporanox capsules (100 mg) (Janssen, Raritan, N.J.) | Paecilomyces, Scopulariopsis, Sporothrix, Alternaria, Sporotrichum, Prototheca. Not active against Fusarium, Mucor, Rhizopus. Very unstable and lipophilic, therefore compounded substances are not recommended. |
| Fluconazole | 14 mg/kg PO loading | LH | Histoplasma, Bastomyces, Coccidioides,27 |
| $ = Inexpensive | followed by 5 mg/kg/ day PO30 | Injectable solution (2 mg/ mL) (Bedford Labs, Bedford, Ohio) Tablets (200 mg) (Pfizer, New York, N.Y.) Generic available Powder (100 g) (Spectrum Chemicals, New Brunswick, N.J.) | Cryptococcus,60,61 Mucor, Rhizopus, Candida,12 Conidiobolomycosis,54,56 Parracoccidia, Paecilomyces, Scopulariopsis, Sporothrix, Alternaria, Sporotrichum, Prototheca. Minimal activity against Aspergillus and Fusarium. |
| Voriconazole $ = Very expensive | 4.0 mg/kg/day PO32-34 | Vfend (Bedford Labs, Bedford, Ohio) Tablets (200 mg) | Drug of choice for invasive Aspergillus,67 Candida, Cryptococcus, Scedosporium apiospermum, Bipolaris, and Fusarium species in human patients that are unable to tolerate or are refractory to other therapeutic agents. |
HCl, Hydrochloride; LH, local wholesaler; PO, by mouth.
and Blastomyces spp.) and Aspergillus spp., with no detectable side effects.31 The use of compounded itraconazole is not recommended. It is very unstable (requires low pH), and owing to its lipophilic nature it is difficult to formulate in aqueous solution.
Oral fluconazole at a loading dose of 14 mg/kg, followed by 5 mg/kg q24h, yields concentrations in plasma, cerebrospinal fluid (CSF), synovial fluid, aqueous humor, and urine above the MIC reported for several equine fungal pathogens.30 Fluconazole, however, reportedly has minimal activity against filamentous fungi (Aspergillus spp. and Fusarium spp.). Low-dose oral fluconazole (1 mg/kg PO q24h) for at least 10 to 15 days anecdotally has been successful in treatment of fungal keratitis. Compounded fluconazole formulations are very stable. The cost of fluconazole has been markedly reduced since the availability of generic products.
Voriconazole, a broad-spectrum triazole antifungal agent, was approved for use in human medicine in 2002. It is now considered the drug of choice for initial treatment of invasive aspergillosis, candidiasis, cryptococcosis, Bipolaris hawaiiensis, and serious fungal infections caused by Scedosporium apiospermum and Fusarium spp. in patients that are unable to tolerate or are refractory to other therapeutic agents.46-49 An initial singledose pharmacokinetic study in horses recommended a dose of 4 mg/kg PO q24h.32 Voriconazole distributes widely into body fluids and reached therapeutic concentrations in peritoneal, synovial, and cerebrospinal fluids; aqueous humor; periocular tear film; epithelial lining fluid; and urine.33-34
SYSTEMIC IODIDE THERAPY. The exact mode of action of iodides is unknown; however, they seem to have a beneficial effect on the granulomatous inflammatory process. Iodides have very little if any direct in vitro antibiotic effect.50 Although several successful cases are reported in which iodides were used as primary or adjunctive therapy, overall efficacy is considered limited at best. Treatment is inexpensive, but iodide toxicity can occur and is characterized by excessive lacrimation, nonproductive cough, increased respiratory secretions, and dermatitis.50 The recommended dose of 20% sodium iodide is 20 to 40 mg/kg/day IV for 7 to 10 days.39,42,51,52 Orally administered iodine is available in two forms. Inorganic potassium iodide (10 to 40 mg/kg/day) is available only as a chemical grade and is unstable in the presence of light, heat, and excessive humidity.42,52 Organic ethylenediamine dihydriodide (EDDI) (0.86 to 1.72 mg/kg of EDDI is equivalent to 20 to 40 mg/ kg/day of the 4.57% dextrose powdered form [Butler Co., Columbus, Ohio]) is commercially available.52 Administration of iodine in the diet of pregnant mares may cause congenital hypothyroidism in foals and thus should be avoided.
ETIOLOGIC AGENTS
Conidiobolomycosis. Conidiobolus coronatus is a saprophytic fungus that causes granulomatous lesions of the upper respiratory tract in horses. Single to multiple granulomatous lesions in the nasal passages, trachea, or soft palate can be observed endoscopically (Fig. 31.19). Histologic appearance of conid- iobolomycosis is similar to that of pythiosis and of basidiobo- lomycosis. Hyphae of C. coronatus are thin-walled, highly septate, and irregularly branched (see Table 31.5).53 The lesions typically have large numbers of eosinophils and fewer macrophages, neutrophils, plasma cells, and lymphocytes surrounding hyphae. Definitive diagnosis is based on microbiological culture, immunodiffusion, or PCR.54 Detection of serum antibodies by immunodiffusion is considered highly sensitive and spe- 5155 55
cific51,55 and can be used to monitor response to treatment.55
Conidiobolomycosis lesions can be treated with surgical excision, laser therapy, cryotherapy, or long-term administration of iodides or antifungals.39,51,54 Amphotericin B has been
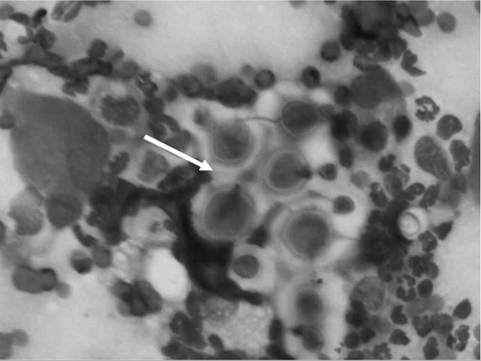
FIG. 31.20 Photomicrographs of an impression smear from a biopsy of a mass in the nasal passage of a horse. The smear is extremely cellular with abundant neutrophils and macrophages. Round yeast cells with large nonstaining capsules and occasional narrow-based budding consistent with cryptococcal organisms (arrow) are shown. (Modified Wright stain, ?100.) (Courtesy Elizabeth Welles, Auburn University, Auburn, Ala.)

FIG. 31.19 Endoscopic image of mycotic granulomas caused by Conidiobolus coronatus in the nasopharynx of a horse.
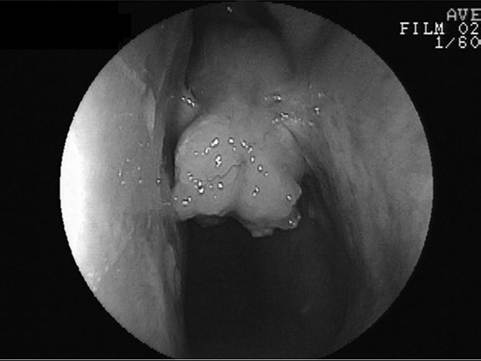
FIG. 31.21 Endoscopic image of a Cryptococcus granuloma in the nasal passages of a horse.
administered intralesionally or topically in combination with dimethyl sulfoxide (DMSO) to treat C. coronatus.39-42 It is important to remember that long-term therapy and reevaluation are essential, as recurrence can occur.42 Oral fluconazole would be considered the drug of choice for the treatment of conid- iobolomycosis, with treatment length varying between 4 and 16 weeks based on endoscopic reevaluation.56 A vaccine using C. coronatus antigen from broth cultures was unsuccessful in treating seven horses with conidiobolomycosis.54
Cryptococcosis. Cryptococcosis is caused by Cryptococcus neoformans (var. neoformans and var. gattii) and is a ubiquitous, saprophytic, round, basidiomycetous yeastlike fungus with a large heteropolysaccharide capsule that does not take up common cytologic stains (see Table 31.5; Fig. 31.20). The capsule forms a clear halo when stained with India ink. The capsule is immunosuppressive and antiphagocytic. A relatively high frequency of equine cryptococcosis occurs in Western Australia.3,57,58 There is an epidemiologic relationship between C. neoformans var. gattii and the Australian river redgum tree (Eucalyptus camaldulensis), whereas C. neoformans var. neoformans has historically been associated with bird (particularly pigeon) excreta.3 Cytologic or histopathologic identification is very reliable for diagnosis because of the characteristic morphology.59 Serologic testing with latex agglutination to identify cryptococcal capsular antigen is useful, with resolution of lesions correlated with declining serum titers.26
Cryptococcosis in horses is associated primarily with pneumonia, rhinitis (Fig. 31.21), meningitis, and abortion. Pulmonary Cryptococcus has been successfully treated with daily intravenous infusions of amphotericin B over 1 month.26 However, four more cases from the same institution were recently successfully treated with oral fluconazole for 7 to 18 months, with declines in cryptococcal antigen titers corresponding to disease resolution.58 Sinonasal cryptococcosis was successfully treated in two horses after extensive surgical debridement and long-term treatment with oral fluconazole.60,61
Cryptococcosis should be treated with fluconazole, amphotericin B, or voriconazole (Table 31.7).
Pseudallescheriosis. Pseudallescheria boydii is a saprophytic ascomycete. Infection most commonly involves the extremities, and in human patients it is known as Madura foot. Hyphae within tissue cannot be differentiated from Fusarium spp. or Aspergillus spp. unless cultured. P boydii cultured from the nasal cavity and sinus of a horse with chronic, malodorous nasal discharge was susceptible in vitro to miconazole, keta- conazole, natamycin, and clotrimazole. After debriding and flushing the plaque, miconazole cream was infused twice daily for 4 weeks through lavage tubing that had been passed into the nasal passage through a hole drilled in the frontal bone and sinuses. Adjunctive iodide therapy was also administered and the lesions resolved.44
Nasal mycosis caused by P boydii has been reported in two other horses, both of which were euthanized.62,63 P boydii has also been isolated from the pharynx of 2 of 60 normal donkeys.64
Aspergillosis. Aspergillus spp. have broad septate hyphae with parallel sides and acute right-angled branching (see Table 31.5). They have a propensity for vascular invasion. Definitive diagnosis is by culture or staining by immunohistochemistry or immunofluorescence. Aspergillus spp. are very common in the environment, especially in moldy feed and bedding.37 They are opportunistic pathogens and often cause disease in horses that are immunosuppressed from debilitating disease such as enterocolitis, septicemia, neoplasia, Cushing's disease, and equine protozoal myeloencephalitis (EPM); that have undergone surgery; or that have been treated with immunosuppressive drugs4,6,8-10 (Fig. 31.22).
Infection is by inhalation of an overwhelming number of spores, resulting in fungal proliferation and invasion of the
■ TABLE 31.7
Treatment of Common Fungal Infections in Humans and Horses
| Infection | Recommended Treatment in Humans87 | Treatments Tried in Horses | Comments |
| Cryptococcosis | Induction with amphotericin B 0.7-1 mg/kg, plus 5-fluorocytosine 100 mg/kg/ day for 2 weeks then consolidation with fluconazole 400 mg/day for >10 weeks. | Daily infusions of amphotericin B (initially 0.35 mg/kg, increasing over 8 days to 0.5 mg/kg in 1 L 5% dextrose in water over 1 h IV for 1 month) successfully used to treat pulmonary cryptococcosis. Flunixin meglumine (0.25 mg/kg IV) was administered before each treatment.26,61 Successful treatment with long-term fluconazole (14 mg/kg loading then 5 mg/kg PO q24h) for sinonasal cryptococcosis after surgical debridement60,61 and pulmonary infection.58 | Reported dosages range from 0.3-0.9 mg/kg in saline IV over 1 h. Long-term oral fluconazole is recommended as sole treatment or after 2 weeks of IV amphotericin B. |
| Histoplasmosis Blastomycosis | Amphotericin B 0.7-1.0 mg/kg/ day for 2 weeks then itraconazole 200-400 mg/day for 4-18 months. Amphotericin B 0.7-1.0 mg/kg/ day to 1.5-2.5 g total or to 0.5 g total then itraconazole 200-400 mg/day | Successful treatment of histoplasmosis in a filly using amphotericin B (0.3-0.6 mg/kg eod IV infused over 1 h) with a total cumulative dose of 6.75 mg/kg administered over 1 month. After each treatment the filly became lethargic for 18-24 h. Polyuria and polydipsia occurred during the fourth week, but urine-concentrating ability was maintained and azotemia did not occur.25 | In vitro susceptibility to fluconazole is poor. |
| Aspergillosis | 1. Voriconazole 200-400 mg PO | Voriconazole 4 mg/kg PO q24h. Successful | Fluconazole has |
| (invasive | q12h, 3-6 mg/kg IV q12h | treatment of a neonatal foal with pulmonary | limited efficacy. |
| pulmonary) | 2. Amphotericin B 1.0-1.5 mg/ kg/day until desired response, then itraconazole 400 mg/day when disease progression slows | aspergillosis after lung lobe resection.67 | Oral itraconazole or voriconazole would be the drugs of choice, possibly after 2 weeks of IV amphotericin B. |
| Candidiasis | 1. Amphotericin B 0.7-1.0 mg/ kg/day for 2 weeks 2. Fluconazole 6 mg/kg for 2 weeks 3. Caspofungin 70 mg ?1, then 50 mg/day for 2 weeks 4. Voriconazole | Two foals were treated with IV amphotericin B for 8 days (total dose 2.6 mg/kg) and 29 days (total dose 10.3 mg/kg), respectively. Fluconazole (5.5 mg/kg PO q24h) for 6 weeks and (4 mg/kg PO q24h) for 28 days was used to treat two other foals.12 | Fluconazole is generally considered the drug of choice against Candida spp., although Candida krusei is resistant to fluconazole. |
| Pneumocystis | 1. TMS 2. Pentamidine isethionate 3. Trimetrexate | TMS (25-30 mg/kg PO q12h) is the treatment of choice.86 Dapsonea (3 mg/kg PO daily for 2 months) was used to successfully treat a foal with Pneumocystis carinii that developed Salmonella enterocolitis after treatment with TMS.24 | Lacks ergosterol, therefore antifungals are not effective. |
aJacobus Pharmaceutical Co. Inc., Princeton, N.J.
eod, Every other day; IV, intravenous; PO, by mouth; TMS, trimethoprim-sulfamethoxazole.
small airways, or by translocation of organisms across an inflamed GI tract leading to lesions centered around large blood vessels as a result of hematogenous spread. In two retrospective studies of invasive pulmonary aspergillosis, 41 of 49 cases were associated with enterocolitis.4,6 Aspergillus spp. pneumonia is almost uniformly fatal, often with no or mild respiratory signs. Antemortem diagnosis of pulmonary aspergillosis is made rarely. In a retrospective study of 30 cases of Aspergillus spp. pneumonia, only 2 cases were diagnosed or suspected antemortem.6 Transtracheal aspirates or bronchoalveolar lavages may not be helpful because hyphae and spores are often present extracellularly or within macrophages in aspirates and lavages from healthy animals.4 False-negative results also can occur. Cytologic examination of a transtracheal wash specimen obtained from the foal shown in Fig. 31.22, A 2 days prior to euthanasia failed to identify Aspergillus spp. hyphae. Serologic diagnosis occasionally has been useful,65 but it is often unreliable because many horses have titers to Aspergillus spp. Development of a commercially available ELISA is promising.8,37
In human medicine, 50% to 90% of patients with invasive aspergillosis die despite treatment. Amphotericin B has been the mainstay of treatment for invasive aspergillus for decades, but it is associated with nephrotoxicity in about 50% of human patients. Nephrotoxicity is reduced with the use of liposomal amphotericin B. Voriconazole, an azole antifungal, is now considered the drug of choice against human aspergillosis, and caspofungin (in the new class of echinocandin antifungals)

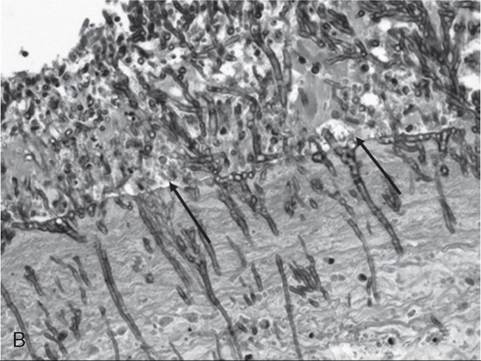
FIG. 31.22 One-month-old foal with Escherichia coli septicemia and secondary Aspergillus pneumonia. A, Dyspneic foal being supported with intranasal oxygen. The foal had eight septic joints and severe pneumonia and was subsequently euthanized because of the guarded prognosis. B, Photomicrograph of the pleural surface of the lung (black arrows) with extensive superficial and deep fungal growth. Aspergillus spp. characteristically have parallel-sided, regular septate hyphae with acute-angled dichotomous branching. They are seen reasonably well with hematoxylin and eosin stain. C, Aspergillus spp. hyphae within pulmonary parenchyma stained metachromatic with specific fungal stain (Gridley stain). (Courtesy Calvin Johnson, Auburn University, Auburn, Ala.)
shows promising results in patients with refractory infections.66 Oral voriconazole and itraconazole are currently the treatments of choice for aspergillosis in horses. In human medicine, itraconazole has shown comparable response rates to those of amphotericin B.66 Aspergillus spp. are usually resistant to fluconazole. There are limited reports of horses surviving pulmonary aspergillosis.37 A neonatal foal with pulmonary aspergillosis was successfully treated by lung lobe resection followed by treatment with systemic voriconazole.67
Treatment of mycotic aspergillus rhinitis and sinusitis in horses has been more successful. It is important, however, to rule out concomitant invasive pulmonary aspergillosis. Oral itraconazole,68 topical natamycin (flushed via an endoscope or indwelling catheter placed into the sinus), nystatin powder (insufflated up the nostril), and topical enilconazole have been curative.69,70
Blastomycosis. Blastomycosis is caused by inhalation of conidiae of the thermally dimorphic saprophytic fungus Blastomyces dermatitidis. Blastomyces yeasts can be identified on cytologic examination, often within multinucleated giant cells. They are spherical, with basophilic protoplasm and unstained, uniformly shaped refractile walls. Unilateral, broad-based budding is characteristic (see Table 31.5).
Blastomycosis was reported to cause pyogranulomatous pleuropneumonia, pulmonary abscessation, peritonitis, and abscesses in a 5-year-old horse.23 B. dermatitidis was positively identified from transtracheal wash fluid by use of a DNA probe, and serologic testing was strongly positive. The horse was euthanized without treatment.23 Disseminated blastomycosis was diagnosed in a miniature horse with subcutaneous infections associated with a chronic pectoral wound. The pony had pulmonary consolidation and pleural effusion. Yeasts were observed histologically in many tissues, and B. dermatitidis was cultured after 6 weeks.71 Disseminated blastomycosis was diagnosed in a mare with unresponsive mastitis that progressed to subcutaneous lesions on the ventrum.72
Treatment with amphotericin B, itraconazole, or fluconazole is recommended (see Table 31.7).
Histoplasmosis. Histoplasmosis is caused by the saprophytic, dimorphic fungus Histoplasma capsulatum and is most prevalent in moist soil containing bird or bat waste. Yeast organisms are 2 to 4 μm in diameter, with a thin clear halo surrounding a round or crescent-shaped basophilic cytoplasm. H. capsulatum has been reported in fewer than 10 equine cases,25 and thus horses are considered to be relatively resistant to disease. H. capsulatum may occur in an enteric, pulmonary, or disseminated form.25 H. capsulatum was identified in pulmonary granulomas in a horse dying of chronic Yersinia colitis.73 It has also been associated with abortions and severe granulomatous pneumonia in neonatal foals (Fig. 31.23) and a yearling.74 Successful treatment with amphotericin B was reported in a filly with pulmonary histoplasmosis diagnosed by cytologic identification of the organism on a tracheal wash smear and from a lung aspirate.25 Treatment with amphotericin B or itraconazole is recommended (see Table 31.7).
Epizootic lymphangitis is caused by Histoplasma capsulatum var. farciminosum. It was eradicated from a number of European and Asian countries by slaughter, but it is still considered an
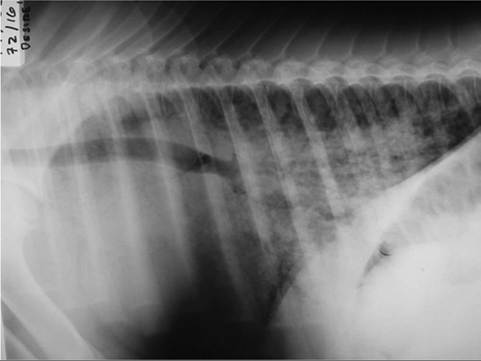
FIG. 31.23 Lateral thoracic radiographs from a foal with Histoplasma pneumonia. (Courtesy Carol Clark, Peterson and Smith Equine Hospital, Ocala, Fla.)
economically important disease in Ethiopia, Senegal, South Africa, Chad, and Gambia, and it is likely still endemic in other African countries and parts of the Middle and Far East.75 Although four forms of the disease—ocular, cutaneous, respiratory, and asymptomatic—are described, they are not distinct clinical entities, and combinations can occur.75 The respiratory form can involve nodules in the mucous membranes of the nares and extend up the nasal passages, down the trachea, and into the pulmonary parenchyma. There is often a mucopurulent nasal discharge, with stertorous noise during respiration in advanced stages. This form causes cough, progressive weakness, and weight loss and is difficult to differentiate clinically from glanders. Control of the disease is gained usually by destroying infected horses and through application of strict hygiene practices to prevent spread of the organism. Organisms can be identified cytologically and definitively diagnosed by culture, but the organism is slow growing, and overgrowth by contaminants is common. Culture on Sabouraud dextrose agar supplemented with glycerol and chloramphenicol is recommended.75 There is a skin test known as the “Histofarcin” test that is useful for field diagnosis, with a sensitivity of 90.3% but a specificity of only 69%; however, the false-positives may be due to subclinical disease.76 Serologic tests were developed but are not commercially available. PCR testing shows promise but is currently not very practical in the field.75 Treatment with systemic iodides, surgical excision, and topical treatment with amphotericin B is variably successful. A cost-effective and currently recommended protocol in impoverished areas consists of lancing all visible nodules under sedation and flushing with 4% tincture of iodine daily; in addition, oral potassium iodine (30 g for a 200- to 250-kg horse by stomach tube or orally in feed is administered daily for 5 days, then every other day for 3 to 4 weeks). This protocol is effective in early cases, but would be unlikely to resolve pulmonary disease.75 Fluconazole would likely be effective, but would be economically prohibitive in most cases.
Coccidiomycosis. Coccidioides immitis is a soil saprophyte
77
that grows in semiarid areas with sandy, alkaline soils." Inhaled arthroconidia enlarge to form nonbudding spherules, which incite an inflammatory reaction in the lungs and lymph nodes.78 Horses infected with this fungus have weight loss, fever, abdominal pain, and signs of respiratory disease. Localized, recurring nasal granulomas also have been reported.79 Diffuse infections, with granulomas in the lungs, liver, kidney, or spleen, have a grave prognosis.78 Przewalskfs horses may be more susceptible.79
C. immitis is difficult to culture, and spherules may not be observed histologically from antemortem lung biopsies. However, serology is very useful for diagnosing infection, and decreasing titers are associated with clinical improvement.27,77 Serum antibodies are detected rarely in healthy horses.80 Higher serologic antibody titers are associated with a poorer prognosis for survival.81 Horses with disseminated disease and pneumonia with thoracic effusion usually have severe clinical disease and frequently die (19 of 21 cases).81 Antifungal agents successful in treating infected horses include itraconazole and fluconazole.27
Scopulariopsis. Scopulariopsis pneumonia was diagnosed by culture of bronchoalveolar lavage fluid in a 2-year-old Quarter Horse filly with pleuropneumonia. The infection resolved following multimodal therapy with ketaconazole and aerosolization of enilconazole.28
Adiaspiromycosis. Adiaspiromycotic miliary fungal pneumonia caused by the saprophytic soil mold Emmonsia crescens was diagnosed in a horse by percutaneous lung biopsy. Euthanasia was performed without treatment.11
Acremonium strictum. A diagnosis of interstitial fungal pneumonia caused by Acremonium strictum was made based on cytologic evaluation, culture, and PCR testing of bronchoalveolar lavage fluid in a 10-year-old horse. The horse made an uneventful recovery with supportive treatment that included 1 month of fluconazole.5 In general, fluconazole has been shown to have poor activity against A. strictum in vitro.82 The isolate cultured from the horse was found to be resistant to fluconazole based on in vitro sensitivity testing that was performed after the course of treatment. It is therefore uncertain if the fluconazole assisted in disease resolution.5
Candidiasis. In human medicine, candidemia is the most common fungal infection in burn patients, neutropenic patients with malignancies, patients undergoing complex abdominal surgery, and patients receiving total parenteral nutrition and long-term corticosteroid therapy.67 In humans, Candida spp. account for 8% to 10% of all blood culture isolates and rank fourth in the list of most frequently isolated pathogens from blood cultures.67 The mortality rate in patients with candidemia is 40% to 75%.67 More than 60% of isolates are Candida albicans6 Fluconazole is generally considered the drug of choice against Candida spp., although Candida krusei is resistant to fluconazole. Itraconazole, amphotericin B, caspofungin, and voriconazole are alternative antifungal agents (see Table 31.7).67
Systemic candidiasis was diagnosed and successfully treated in four neonatal foals. Each foal had prior sepsis attributable to gram-negative bacteria that had been aggressively treated with numerous antibiotics and parenteral nutrition. C. albicans was cultured from a transtracheal wash from one of the foals. Three of the foals had Candida glossitis, and one had panophthalmitis and fungal keratitis. Two of the foals were treated with intravenous amphotericin B, and oral fluconazole was used on the other two foals.12
Superficial Candida spp. infections of the mucous membranes (thrush)83 can occur in isolation or as part of a systemic infection, and further microbiological culturing of the blood, tracheal wash, urine, or joint fluid may be indicated to rule out systemic infection.12 Candida spp. glossitis can be treated by rinsing the mouth either with potassium permanganate (0.025% q24h) or nystatin (0.3 g in 10 mL of water q8h).
Pneumocystosis. Pneumocystis carinii (renamed P. jiroveci in humans) has been reclassified from a protozoan to a saprophytic fungus based on the DNA sequence of its 16S-like RNA subunit, but some researchers consider it to be a plant because it lacks ergosterol, the major fungal sterol.84 It exists as an ameboid yeast or as a cystic sporangia. P. carinii cannot be cultured, and diagnosis is based on the cytologic identification of characteristic morphologic features using specimens obtained by bronchoalveolar lavage rather than tracheal wash. A fluorescent in situ hybridization method with an oligonucleotide

FIG. 31.24 Horse with retropharyngeal lymphadenopathy resulting in head and neck extension characteristic of Streptococcus equi infection.
probe that targets the 18S ribosomal RNA has been developed recently to detect P. carinii in histologic sections.21 Immunohistochemistry also can be used.20
P. jiroveci is the most common organism to cause opportunistic infection in people with HIV, and people undergoing immunosuppressive therapy after organ transplantation are predisposed. P carinii causes diffuse interstitial pneumonia, especially in immunocompromised patients such as Arabian foals with SCID.13 It also has been diagnosed in immunocompromised adult horses,14,15 as well as in an immunocompetent foal.20 TMS (25 to 30 mg/kg PO q12h) is the treatment of choice (see Table 3 1.7).85,86 Dapsone (3 mg/kg PO daily for 2 months; Jacobus Pharmaceutical, Princeton, N.J.) was used to successfully treat a foal that developed Salmonella enterocolitis after treatment with TMS.24