Surgical Disorders of the Small Intestine
John F. Marshall • Anthony T. Bhkslager
■ Simple Obstruction Simple intestinal obstruction is a physical obstruction of the lumen without obstruction of

FIG.
32.64 Section of small intestine from a foal with chyloabdomen and a Rhodococcus equi abdominal abscess (arrow). Mesenteric lymphatic channels are distended with white chyle, as are serosal lymphatic channels. (Courtesy Dr. MJ. Murray.)mesenteric vascular flow (i.e., nonstrangulating obstruction). The most common causes are intraluminal masses composed of feed material (e.g., ileal impaction) and accumulation of parasites (e.g., ascarid impactions). Other instances in which the bowel is obstructed without associated compromise of blood supply include extraluminal compression by a mass or band of tissue in horses with intraabdominal adhesions and IFEE lesions. The large volume of fluid entering the small intestinal lumen on a daily basis1,2 causes the obstructed intestine to become distended. Therefore although the mesenteric blood supply is not directly involved in simple obstructions, progressive and marked distention can result in decreased mural blood flow3,4 and eventual necrosis of tissues.5
ASCARID IMPACTIONS. Impactions caused by Parascaris equorum typically occur in weanling foals (median age, 5 months; range, 4 to 24 months) that have been on a poor deworming program and that are administered an anthelmintic when they have a heavy parasite burden.6 Products that cause sudden ascarid paralysis or death, including piperazine, organophosphates, and pyrantel pamoate, have been incriminated.7 However, any effective broad-spectrum anthelmintic, such as the avermectins, probably has the same effect. Clinical signs include variable onset of colic after administration of an anthelmintic (usually within 1 to 5 days) and signs compatible with small intestinal obstruction, including nasogastric reflux.6 The onset of the disease varies according to the degree of obstruction.7 Diagnosis may be tentatively based on the history in a foal that appears unthrifty, has been recently dewormed, and has signs referable to small intestinal obstruction.
The presence of dead ascarids in nasogastric reflux raises the index of suspicion of this particular form of obstruction.6 Abdominal radiographs or ultrasonography may indicate the presence of multiple loops of distended small intestine, but neither imaging study is needed if clinical signs indicate the need for immediate surgery. Surgical treatment typically involves an enterotomy made over the intraluminal impaction and removal of ascarids.Although simple intestinal obstruction tends to carry a favorable prognosis for survival, ascarid impaction is a notable exception. The mortality rate in these cases is high (up to 92% in one study) as a result of severe intestinal compromise, peritonitis, and development of adhesions. The severe intestinal compromise is almost entirely attributable to the duration of impaction, which, for unknown reasons, is not as readily recognized in foals as it is in adults. Reasons for this could include failure of the owner or farm manager to recognize colic in foals or failure on the part of the owner or veterinarian to recognize the implications of colic in foals. Although foals readily display signs of colic, other medical causes of colic such as gastric ulcer disease or enteritis might be more significant in the differential diagnosis than for adults. Second, the size of a foal may make episodes of colic appear more manageable than in adults, in which colic-induced trauma, especially to the head, may force the issue of referral and surgery at an earlier stage. This is speculative, but early intervention in foals with ascarid impaction would probably result in dramatic reductions in the reported mortality rate.6 Improved survival rates have, in fact, been reported: For example one case series indicated that 12 (80%) of 15 horses studied survived to discharge, and 6 (60%) of 10 for which follow-up data were available survived for at least 1 year.8 This improvement was related to changing the surgical technique to manually evacuating ascarids into the cecum rather than performing an enterotomy or resection and anastomosis.8 However, many cases have multifocal and marked impaction by ascarids that are large and difficult to manipulate.
The need for an enter- otomy or resection probably relates to the initial severity of disease, and not all cases may be amenable to manual evacuation into the cecum.ILEAL IMPACTION. Ileal impactions occur most commonly in adult horses in the southeastern United States. Although feeding of coastal Bermuda hay has been implicated in the regional distribution of this disease, it has been difficult to separate geographic location from regional hay sources as risk factors.9 However, a study from the southeastern United States showed that the feeding of coastal Bermuda hay and failure to deworm with an anthelmintic with efficacy against tapeworms are significant risk factors for ileal impaction.10 Furthermore, in a study performed in the United Kingdom, horses with evidence of tapeworm infection were at risk for developing ileal impaction.11
Typical signs in an adult horse with small intestinal obstruction include onset of moderate to severe colic and loops of distended small intestine rectally palpable as the condition progresses. Because the ileum is the most distal aspect of the small intestinal tract, nasogastric reflux may take a considerable time to develop and is found in only approximately 50% of horses requiring surgical correction of ileal impaction.12,13 The diagnosis is usually made at surgery, although an impacted ileum may be palpated rectally.14 However, multiple loops of distended small intestine frequently make the impaction difficult to palpate. Nonetheless, clinicians working in the southeastern United States who evaluate horses with cases of mild or moderate colic that have a history of eating coastal Bermuda hay, and in which distended loops of small intestine can be detected adjacent to the cecum, should strongly suspect ileal impaction.
Ileal impactions may resolve with medical treatment. In particular, horses with clinical signs compatible with obstruction of the small intestine and normal abdominal fluid should be treated medically unless pain is unmanageable or subsequent abdominal fluid samples indicate intestinal compromise.
In cases in which surgery becomes necessary, fluids (2 to 3 L) can be directly infused into the mass, which allows the surgeon to break down the impaction. However, extensive small intestine distention and intraoperative manipulation of the ileum frequently leads to postoperative ileus (POI).15 Therefore some surgeons now elect to perform an enterotomy and to flush the contents from the intestinal lumen with minimal manipulation. Although early studies indicated a guarded prognosis,13 a more recent study indicated that the prognosis is excellent for both medically and surgically managed ileal impactions.16ILEAL HYPERTROPHY. Ileal hypertrophy is a disorder in which the muscular layers (both circular and longitudinal) of the ileum enlarge for unknown reasons. Parasitism has been implicated, particularly parasites that tend to localize to the ileum (such as tapeworms),17 but this has never been proven. In some cases the jejunum may also be hypertrophied, either alone or in combination with the ileum.18 It is clear from these findings that initial functional obstruction initiates this syndrome, causing the musculature of the intestine to hypertrophy in order to push intestinal contents aborally, but there is no evidence as to the mechanisms of this disease. Clinical signs include chronic intermittent colic as the ileum hypertrophies and gradually occludes the lumen. In one study, partial anorexia and chronic weight loss (1 to 6 months) were documented in 45% of affected horses.19 The diagnosis is usually made at surgery, although in some cases the hypertrophied ileum may be palpated rectally or visible on ultrasonographic evaluation of the abdomen.19 Treatment involves an ileocecal or jejunocecal anastomosis to bypass the hypertrophied ileum. Without surgical bypass, intermittent colic persists, and the thickened ileum may ultimately rupture. According to one report of 11 horses with hypertrophy of the ileum, only 1 horse survived, which indicates a poor prognosis.
The most common reason for euthanasia was spontaneous ileal rupture.18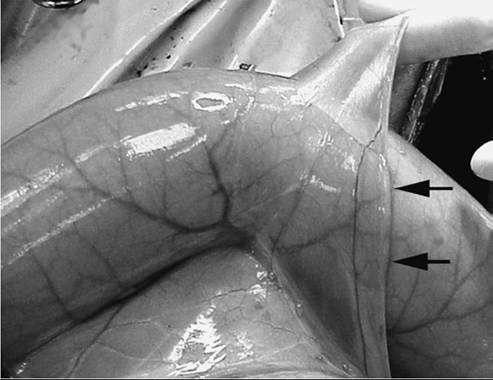
FIG. 32.65 Jejunal mesodiverticular band. This anomaly was an incidental finding during exploration of the horse’s abdomen. Intestine may become entrapped within the mesenteric pocket formed by the attachment of the ventral to the dorsal mesentery (arrows).
MECKEL DIVERTICULUM. A Meckel diverticulum is an embryonic remnant that may become impacted. The diverticulum arises from the vitelloumbilical duct, which fails to atrophy completely and becomes a blind pouch projecting from the antimesenteric border of the ileum.20,21 An associated mesodiverticular band occasionally extends from the diverticulum to the umbilical remnant and serve as a point around which small intestine may become strangulated. Mesodiverticular bands may also originate from the embryonic ventral mesentery and attach to the antimesenteric surface of the bowel, thereby forming a potential space within which intestine may become entrapped (Fig. 32.65).22 Clinical signs range from chronic colic for an impacted Meckel diverticulum to acute severe colic if a mesodiverticular band strangulates intestine. The diagnosis is made at surgery, and treatment entails resection of the diverticulum and any associated bands.23
IDIOPATHIC FOCAL EOSINOPHILIC ENTERITIS. IFEE is a relatively recently described condition of the small intestine of horses. Since 2000, the condition has been reported in the United Kingdom and the United States, and although its diagnosis appears to be increasingly common, no causative agent or other etiology has been described.24,25,26 The clinical presentation of horses with this condition is consistent with that of nonstrangulating small intestinal obstruction, and horses younger than 5 years of age are at increased risk.26 IFEE is diagnosed during exploratory celiotomy when palpably thickened serosal plaques or circumferential constricting bands are identified in the jejunum.
Multiple plaques or bands may be present throughout the jejunum. Early reports of surgical resection of the affected intestine revealed a fair prognosis; in one, 7 of 10 surgically treated horses survived to discharge.24 In cases in which abnormal portions of small intestine has been resected, the diagnosis can be confirmed by histologic examination, which reveals severe transmural eosinophilic enteritis. However, pathologic and histologic examinations have not identified the cause of these lesions, and helminths have not been associated with them.24 Although surgical treatment of this condition (resection and anastomosis) is frequently required, the majority of cases are treated by manual evacuation of impacted feed material into the cecum and parenteral administration of corticosteroids. An epidemiologic study of IFEE in the northwest of England revealed a seasonal pattern of the disease: The risk was highest between July and November.26■ Strangulating Obstruction Strangulating obstruction of the intestine is characterized by simultaneous occlusion of the intestinal lumen and its blood supply. Although strangulation of the intestinal lumen results in clinical signs similar to those of simple obstruction, occlusion of the blood supply results in a more rapid deterioration of the intestinal mucosa and subsequent onset of endotoxemia. Therefore clinical signs (including pain, heart rate, mucous membrane color, and capillary refill time) are typically more severe, and the prognosis is less favorable.
A great deal of work has been done to characterize mucosal 27 28 29
injury that occurs during strangulation, and reperfusion.29 In general, the lesion that develops during strangulation is severe: the small portion of bowel left viable is vulnerable to further injury during reperfusion.30 The severity of the ischemic lesion is partly attributable to the fact that in most cases, initial occlusion of veins and partial occlusion of arterial blood supply during strangulation induces a hemorrhagic lesion. This results in extensive congestion and mucosal degeneration (Fig. 32.66).27 Bowel peripheral to the strangulating lesion may also become injured as a result of distention.31 In addition, distended small intestine that remains viable after surgical correction of strangulation may be subject to postoperative reperfusion injury through the generation of reactive oxygen metabolites.32 Although attempts at reducing mucosal injury in a horse with antioxidants have met with some success,33 their clinical use is limited.
The prognosis for survival in horses with SISO is generally poorer than those of most other types of colic. In a number of studies, rates of short-term survival of horses with SISO were between 55% and 84%. A large single-center study that included 147 horses with small intestinal disease demonstrated that short-term survival rate was significantly lower among horses with SISO (54.8%) than among those with a simple obstruction (79.6%).34 In contrast, however, a review of 74 horses revealed no significant difference in short-term survival rate between horses with SISO (84%) and those with a simple obstruction (91%).35 The importance of early referral and diligent assessment of intestinal viability was highlighted by a case series of 35 horses with strangulating small intestinal lesions that were managed without resection and anastomosis; the reported rate of survival to discharge was 100%.36 It is important to discuss with owners the potential postoperative complications and long-term survival rates. Studies in which horses were monitored after discharge from the hospital have revealed significantly lower survival rates after 12 months, ranging from 47% to 68%.37-39
Episodes of colic are the most frequently reported complication after discharge38,40 and are significantly more common in horses with small intestinal obstruction than in those with large colon disease.38 A significant reason for repeated episodes of colic and reduced long-term survival in patients that have had small intestinal surgery is intraabdominal adhesions (Fig. 32.67). For example, in one study, 22% of horses undergoing small intestinal surgery required further surgery or were euthanized because of adhesions, and only 25% of horses that had a clinical problem with adhesions survived.41 A more recent study of 99 horses requiring repeat celiotomy demonstrated that intraabdominal adhesions were the most common pathologic finding.42 In that study, however, horses with small intestinal lesions were not more likely to develop adhesions than were those with large colon lesions, and horses with adhesions were no less likely to survive than those without.42
EPIPLOIC FORAMEN ENTRAPMENT. The epiploic foramen is a potential opening (because the walls of the foramen are usually in contact) to the omental bursa located within the right cranial quadrant of the abdomen. It is bounded dorsally by the caudate process of the liver and caudal vena cava and
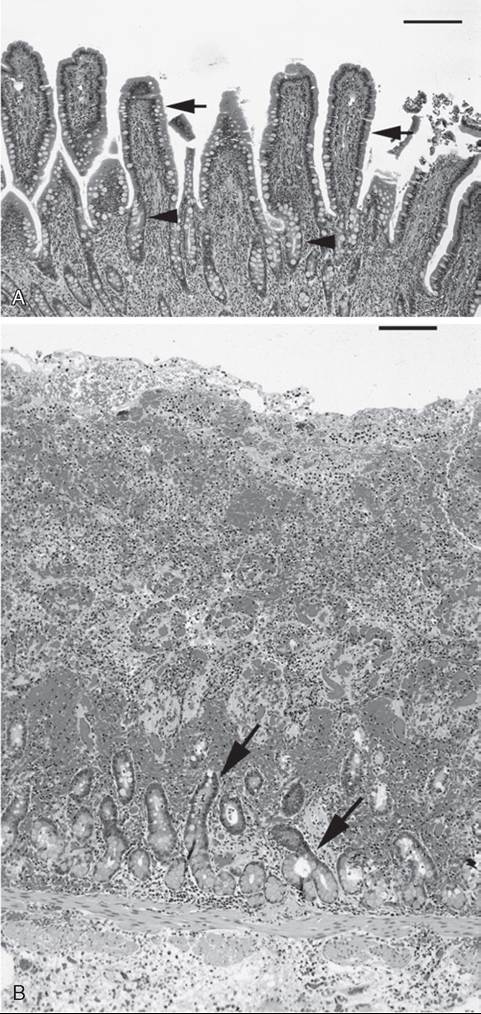
FIG. 32.66 Histologic appearance of normal and strangulated jejunal mucosa. A, Normal equine jejunal mucosa, with extensive villi (arrows) and mucosal crypts (arrowheads). B, Hemorrhagic strangulating lesion of the jejunum, with complete loss of villi and extensive hemorrhage. Note the presence of crypts (arrows), which remain relatively undamaged. (Scale: 1 cm = 100 μm.)
ventrally by the pancreas, the hepatoduodenal ligament, and the portal vein.43,44 Clinical signs include acute onset of severe colic, and examination findings are compatible with small intestinal obstruction. Although the condition was reportedly more prevalent in older horses, studies have not revealed an age predilection.45 However, a seasonal pattern for this disease has been detected. Specifically, more horses appear to suffer from epiploic foramen entrapment during the fall and winter months, which may reflect management practices.46 An additional factor associated with epiploic foramen entrapment is

FIG. 32.67 Intraabdominal adhesion in a foal. Note the presence of a mature fibrous adhesion between two segments of jejunum (arrows) that resulted in kinking and partial obstruction of the affected intestine.
crib-biting. One possible reason for this association is the development of negative intrathoracic pressure during cribbing, which might then result in cranial movement of intestine into the vicinity of the epiploic foramen. The association between crib-biting and epiploic foramen entrapment has been shown in separate studies performed in the United Kingdom and the United States.47
The diagnosis is definitively made at surgery, although ultrasonographic findings of distended loops of edematous small intestine adjacent to the right middle body wall are suggestive of epiploic foramen entrapment.43 Entrapped small intestine may enter the foramen from the visceral surface of the liver toward the right body wall or in the opposite direction. In most cases, however, the intestine enters the foramen in a left-to-right direction.43,47 Small intestine entrapment may be limited to a portion of the intestinal wall (parietal hernia).49 In addition, the large colon may become entrapped within the epiploic foramen.50 In the treatment of epiploic foramen entrapment, the epiploic foramen must not be enlarged either by blunt force or with a sharp instrument because the vena cava or portal vein may be ruptured and fatal hemorrhage may occur. In addition, excessive force used to extract entrapped bowel during surgery may also result in rupture of a mesenteric branch of the cranial mesenteric artery. In some cases of epiploic foramen entrapment, intraabdominal hemorrhage found before surgery may result from compromise of the mesenteric blood supply rather than the major blood vessels that border the epiploic foramen. The prognosis has substantially improved since the 1990s, with short-term survival rates (discharge from the hospital) ranging from 74% to 95% in the most recent studies.43,51,52
STRANGULATION BY MESENTERIC PEDUNCULATED LIPOMA. Lipomas form between the leaves of the mesentery as horses age, and mesenteric stalks develop as the weight of the lipoma tugs on the mesentery. The stalk of the lipoma and a loop of small intestine or small colon may become intertwined and lead to strangulation (Fig. 32.68). Strangulating lipomas should be suspected in mature horses (>10 years old) with acute colic referable to the small intestine.53 In addition, geldings and

FIG. 32.68 Strangulating lipoma of the ileum. A lipoma, together with its mesenteric stalk (arrows), has become intertwined with a loop of the ileum, which resulted in a hemorrhagic strangulating obstruction.
ponies appear to be at risk for developing strangulating lipomas,54 possibly because of differences in fat metabolism. One study documented a case of strangulating lipoma in a much younger patient, which indicates that although the aging process is associated with development of lipomas, this diagnosis cannot be ruled out preoperatively on the basis of age alone.55,56 The diagnosis is usually made at surgery.
Treatment involves surgical resection of the lipoma and strangulated bowel, although strangulated intestine is, on occasion, viable. Studies indicate that approximately 60% to 78% of horses are discharged from the hospital after surgical treatment.53,57,58
SMALL INTESTINAL VOLVULUS. A volvulus is the twisting of a segment of small intestine more than 180 degrees along the axis of the mesentery. Small intestinal volvulus is theoretically initiated by a change in local peristalsis, but the mechanisms of this disease are unclear.59 It is reportedly one of the most commonly diagnosed causes of small intestinal obstruction in foals.60 It has been theorized that young foals may be at risk for small intestinal volvulus because of changing feed habits as they adapt to a forage-based adult diet. However, a report of 115 cases of small intestinal volvulus found that 74% of the affected animals were aged 3 years or older.61 Onset of acute, severe colic, a distended abdomen, and radiographic or ultrasonographic evidence of multiple loops of distended small intestine in a young foal are suggestive of small intestinal volvulus. However, volvulus cannot be differentiated preop- eratively from other causes of small intestinal obstruction.
In adult horses, volvulus frequently occurs in association with another disease process, during which small intestinal obstruction results in distention and subsequent rotation of the small intestine around the root of the mesentery (e.g., in horses that have strangulation caused initially by a pedunculated lipoma). Although any segment of the small intestine may be involved, the distal jejunum and ileum are most frequently affected, probably because the mesentery is longer in the more distal portion of the bowel. The diagnosis is made on palpation of a twist at the origin of the cranial mesenteric artery during surgical exploration. Treatment includes resection of devitalized bowel, which may not be an option because of the extent of small intestinal involvement. For example, if complete volvulus of the small intestinal tract occurs, the only option would be to untwist the intestine and hope that the bowel was sufficiently viable to survive the disease process. This would in turn depend on the duration of disease and the extent of intestinal ischemia (i.e., how tightly the intestine twisted as the volvulus developed). Prognosis is based on the extent of small intestine involved and its appearance after surgical correction of the lesion.62 For example, the degree of sepsis may be related to the surface area of devitalized tissue. In addition, the length of the time it takes to complete the surgery can become problematic, particularly in patients with sepsis, in which it is difficult to maintain adequate arterial blood pressure. Nonetheless, survival in patients with extensive small intestinal resection may not be related to the absolute length of intestine resected.63 The prognosis for short-term survival is good; one study suggested that 80% of horses are discharged after surgery.34
INGUINAL HERNIA. Inguinal hernias are more common in Standardbred and Tennessee Walking horses, which tend to have congenitally large inguinal canals. Inguinal hernias may also occur in neonatal foals, but they differ from hernias in mature horses in that they are typically nonstrangulating. Typical historical findings in mature horses with inguinal hernias include acute onset of colic in a stallion that has recently been used for breeding. A cardinal sign of inguinal herniation is coolness and enlargement of one testicle.64,65 This is attributable to occlusion of the testicular blood supply in most cases rather than strangulated intestine within the scrotum itself. Inguinal hernias can also be detected on rectal palpation, and ultrasonography of the testicle is very helpful in determining the diagnosis, particularly of testicular torsion. The nature of the hernia (direct versus indirect) is determined by the integrity of the parietal vaginal tunic. In horses in which the bowel remains within the parietal vaginal tunic, the hernia is said to be indirect because the bowel remains within the peritoneal cavity. Direct hernias are those in which the bowel ruptures through the parietal vaginal tunic and occupies a subcutaneous location, followed by strangulation. Direct hernias most commonly occur in foals and should be suspected when a congenital inguinal hernia is associated with colic, swelling that extends from the inguinal region of the prepuce, and intestine that may be palpated subcutaneously.66,67 Although most congenital indirect inguinal hernias resolve with repeated manual reduction or application of a diaper, or both, surgical intervention is recommended in foals with congenital direct hernias in order to reduce the hernia, as well as repair the parietal vaginal tunic.
In stallions with indirect inguinal hernias, the hernia is typically surgically reduced via combined inguinal and midline ventral abdominal incisions to allow visual inspection of the small intestine and, if necessary, resection and anastomosis. However, in many cases taken to surgery the short segment of herniated intestine improves markedly in appearance once it has been manually or surgically reduced, and in some cases the affected intestine can be left unresected. In these cases, subsequent laparoscopic closure of the internal vaginal ring is recommended to prevent recurrence and simultaneously retain the associated testicle.68 In cases of nonreducible hernias, the affected testicle is congested because of vascular compromise within the spermatic cord, and although it may remain viable, it is recommended that it be resected and the external inguinal ring closed. If the testicle is retained, the inguinal canal should be partially closed at surgery to prevent recurrence, but the risk that this procedure will reduce spermatic cord vasculature is another problem. The prognosis in adult horses is good; 76% of horses in one study were alive 6 months after discharge.65 Horses that have been unilaterally castrated during surgical treatment of inguinal hernias may be used for breeding. In these horses, the remaining testicle has increased sperm production, although an increased number of sperm abnormalities will be noticed after surgery because of edema and increased temperature of the scrotum.
STRANGULATING UMBILICAL HERNIAS. Whereas umbilical hernias are common in foals, strangulation of herniated bowel is rare. In one study, 6 (4%) of 147 horses with umbilical hernias had incarcerated intestine.69 The hernia sac is warm, swollen, firm, and painful in association with signs of colic. The affected segment of bowel is usually the small intestine, but herniation of the cecum or large colon has also been reported.70 In rare cases, a hernia involves only part of the intestinal wall and is referred to as Richter hernia. In foals that have Richter hernia, an enterocutaneous fistula may develop. In one study, all 13 foals with strangulating umbilical hernias survived to discharge, although at least 3 died because of 70
long-term complications.70
DIAPHRAGMATIC HERNIAS. Herniation of intestine through a rent in the diaphragm is uncommon in horses, accounting for 0.3% of all cases of colic in a large multicenter study.34 Any segment of bowel may be involved, although the small intestine is most frequently herniated.71 Diaphragmatic rents may be congenital or acquired, but acquired hernias are more common. Congenital rents may result from incomplete fusion of any of the embryonic components of the diaphragm: pleuroperitoneal membranes, transverse septum, and esophageal mesentery. In addition, abdominal compression of the foal at parturition may result in a congenital hernia. Acquired hernias are presumed to result from trauma to the chest or a sudden increase in intraabdominal pressure, as might occur during parturition, distention of the abdomen, a sudden fall, or strenuous exercise.72 In one study, of 40 horses diagnosed with diaphragmatic hernia, 19 (48%) had a history of recent trauma.72 Hernias have been found in several locations, although large congenital hernias are typically present at the most ventral aspect of the diaphragm, and most acquired hernias are located at the junction of the muscular and tendinous portions of the diaphragm. In addition, a peritoneal-pericardial hernia has been documented in at least one horse.73
The clinical signs are usually associated with intestinal obstruction rather than respiratory embarrassment. However, careful auscultation may reveal an area of decreased lung sounds in association with obstructed intestine and increased fluid within the chest cavity. Such signs may prompt thoracic radiography or ultrasonography, both of which can be used to make a diagnosis. In one review, of 40 horses reported in the literature with diaphragmatic hernia, 7 (18%) had dyspnea.72 Auscultation may also reveal thoracic intestinal sounds, but it is typically not possible to differentiate these from sounds referred from the abdomen. In another report, two of three horses with small intestinal strangulation by diaphragmatic hernia had respiratory acidemia, attributable to decreased ventilation.74 Because of the difficulties in correcting diaphragmatic hernias and the associated complicating factors such as pneumothorax, these cases are generally considered to have a poorer prognosis than are other causes of colic. Reports of 31 and 44 cases demonstrated that 46% and 27%, respectively, of affected horses undergoing surgical treatment survived to discharge, and the overall success rates were only 23% and 16%, respectively.75,76
INTUSSUSCEPTIONS. An intussusception involves a segment of bowel (intussusceptum) that invaginates into an adjacent aboral segment of bowel (intussuscipiens). The reason for such invagination is not clear, but it may involve a lesion at the leading edge of the intussusception, including small masses, foreign bodies, or parasites. In particular, tapeworms (Anop- Iocephala perfoliata) have been implicated.77 Ileocecal intussusceptions are the most common intestinal intussusceptions in horses and typically affect young animals. For example, in one evaluation of 26 cases of ileocecal intussusception, the median age of the horses was 1 year.78 Acute ileocecal intussusceptions are those in which the duration of colic is less than 24 hours, and they involve variable lengths of intestine that ranged in one study from 6 cm to 457 cm long. In acute cases the involved segment of ileum typically has a compromised blood supply. Chronic ileocecal intussusceptions typically involve short segments of ileum (up to 10 cm long), and the ileal blood supply is frequently intact.
Abdominocentesis results are variable because strangulated bowel is contained within the adjacent bowel. There is often evidence of obstruction of the small intestine, including nasogastric reflux and multiple distended loops of small intestine on rectal palpation. Horses with chronic ileocecal intussusceptions have mild, intermittent colic, often without evidence of small intestinal obstruction. A mass may be palpated in the region of the cecal base in approximately 50% of cases. Transabdominal ultrasonography may be helpful in discerning the nature of the mass. The intussusception has a characteristic target appearance on cross-section/9
Other segments of the small intestine, including the jejunum, may also be intussuscepted. In one study on 11 jejunojejunal intussusceptions, the length of bowel involved ranged from 0.4 to 9.1 m.80 Attempts at reducing intussusceptions at surgery are usually futile because of intramural swelling of affected bowel. Jejunojejunal intussusceptions should be resected. For acute ileocecal intussusceptions, the small intestine should be transected as far distally as possible and a jejunocecal anastomosis created. In cases of particularly long intussusceptions (lengths up to 10 m has been reported), an intracecal resection may be attempted. For horses with chronic ileocecal intussusceptions, a jejunocecal bypass without small intestinal transection should be performed.
In one study of the survival of horses with ileocecal intussusceptions, all 7 horses with chronic intussusceptions survived long term (>4 months), whereas only 5 (42%) of 12 horses with acute intussusceptions survived long term.78 In a separate study of survival in horses with jejunojejunal intussusceptions, 6 (54%) of 11 horses were discharged from the hospital after surgery, and 4 (36%) of 11 horses survived long term (>16 months).80
OTHER SMALL INTESTINAL STRANGULATIONS. Entrapment of the small intestine may occur through rents in the mesentery or in internal ligaments such as the gastrosplenic ligament,81 the broad ligament, and the proximal aspect of the cecocolic ligament.82 Entrapments may also occur through trauma-induced body wall hernias. For all of these conditions it is often necessary to enlarge the rent or hernia to allow reduction of entrapped small intestine. In the case of body wall hernias, the defect should be closed with suture or patched with mesh. Entrapment of small intestine within mesenteric rents can be particularly problematic because they can be difficult to reduce and the rents are often difficult to close. Mesenteric rents have been associated with an unfavorable prognosis, possibly because large lengths of intestine may become strangulated and because the mesenteric vasculature is frequently compromised to the extent that intraabdominal hemorrhage has been noted in some cases.83 However, a case series involving 38 Thoroughbred broodmares with small intestinal mesenteric rents reported short-term survival rates of 76% overall and 88% among horses that recovered from anesthesia.84 The inability to close the rent at surgery was associated with increased likelihood of colic after hospital discharge but did not affect overall survival. This study probably highlights the benefits of prompt referral before significant lengths of intestine are strangulated and the importance of making every effort to close the rent at surgery.
■ Nonstrangulating Infarction Nonstrangulating infarction occurs secondary to cranial mesenteric arteritis caused by migration of S. vulgariS8 and has become rare during surgery since the advent of broad-spectrum anthelmintics. Although thromboemboli have been implicated in the pathogenesis of this disease, careful dissection of naturally occurring lesions has not revealed the presence of thrombi at the site of intestinal infarctions in most cases. These findings suggest that vasospasm plays an important role in this disease.85 Clinical signs are highly variable, depending on the extent to which arterial flow is reduced and the segment of intestine affected. Any segment of intestine supplied by the cranial mesenteric artery or one of its major branches may be affected, but the distal small intestine and large colon are more commonly involved. There are no clinical variables that can be used to reliably predict or differentiate this disease from strangulating obstruction. In some cases massive infarction results in acute, severe colic. In other cases intermittent colic develops as smaller emboli are released into the colonic blood supply. An abnormal mass and fremitus are occasionally detected on palpation of the root of the cranial mesenteric artery on rectal palpation. This disease should be considered part of the differential diagnosis in horses with a history of inadequate anthelmintic treatment and the presence of intermittent colic that is difficult to localize. Although fecal parasite egg counts should be performed, they are neither indicative of the degree nor specific for the type of parasitic infestation.
In addition to routine treatment of colic, dehydration, and endotoxemia, medical treatment may include aspirin (20 mg/ kg q24h) to decrease the risk of thrombosis. Definitive diagnosis requires surgical exploration. Surgical treatment depends on the distribution of infarction. Unfortunately, these cases are difficult to treat because of the patchy distribution of the lesions and the possibility that lesions extend beyond the limits of surgical resection. In addition, further infarction may occur after surgery. The prognosis is fair for horses with intermittent mild episodes of colic that may be amenable to medical therapy, but horses that require surgical intervention have a poor prognosis.85