INTESTINES (See also pp. 129-135.)
Because the general features of the intestinal tract have been described, it is now appropriate to concentrate on its relationships to other organs and to external landmarks and on its attachments and blood supply.
The small intestine is relatively short, perhaps three or four times the body length. Of this, the duodenum contributes, on average, only 25 cm. The short cranial part of the duodenum passes dorsally and to the right, against the visceral surface of the liver, roughly opposite the ninth intercostal space. It is continued caudally beyond the porta as the descending duodenum, which follows the right abdominal wall to reach a point somewhere between the fourth and sixth lumbar vertebrae (Figure 14-7, BZ7'). In its passage it is related dorsally to the right lobe of the pancreas, ventrally to the jejunal mass, and medially to the ascending colon and cecum (Figure 14-15Z5). The mesentery of the descending duodenum begins by being relatively long but shortens toward the caudal flexure, where the gut is closely anchored to the abdominal roof. An additional (duodenocolic) fold with a free caudal border attaches the duodenum to the descending mesocolon at this level. The ascending duodenum (Figure 14-15Z6), which begins at the caudal flexure, is more tightly tethered than the preceding segment and runs forward, close to the midline, between the descending colon on the left and the root of the mesentery. It turns ventrally at the cranial limit of the root to be continued by the jejunum. Other relations of this part are the medial border of the left kidney dorsally and the jejunal mass ventrally (Figure 14-8, A, and Figure 14-12, B).
The jejunum and short ileum form a mass occupying the ventral part of the abdomen between the stomach and the bladder (Figures 14-5, 14-6, 14-16, and 14-17). The coils of the jejunum are quite mobile, and at first sight their disposition appears to be haphazard; closer inspection shows that there is some pattern to the arrangement.
The mainly sagittal coils of the proximal part lie largely cranial to the more transverse coils of the distal part (Figure 14-8, A). The suspending mesentery is relatively long and imposes little restraint, which allows the gut to slip freely over the floor in response to respiratory and other movements. This feature enables the surgeon to exteriorize much of the jejunum to improve the exposure of more dorsal organs. Dorsally, the jejunal mass extends to the descending duodenum on the right and the kidney and sublumbar muscles on the left. The jejunal coils are generally entirely related to the folded greater omentum ventrally; cranially only the deep leaf intervenes between them and the stomach. The ileum arises at the caudal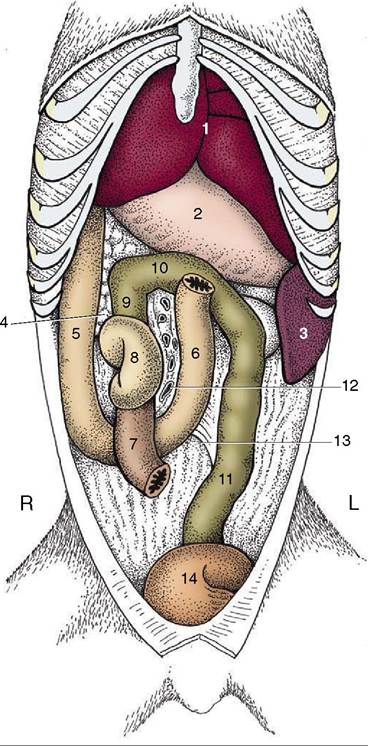
Figure 14-15 The canine duodenum, cecum, and colon in situ; ventral view. 1, Liver; 2, stomach; 3, spleen; 4, pancreas; 5, descending duodenum; 6, ascending duodenum; 7, ileum; 8, cecum; 9, 10, 11, ascending, transverse, and descending colon; 12, vessels in root of mesentery; 13, duodenocolic fold; 14, bladder.
end of the mass and passes forward and to the right to open into the ascending colon below the first or second lumbar vertebra.
Small patches of aggregate lymph nodules of varying sizes are present throughout the small intestine; the largest are said to be in the ileum.
In life the intestine is not uniformly full, and at any moment most parts are flattened and molded by the pressures of adjacent viscera. The lumen may be locally obliterated, and when a passage is retained, it is more often than not reduced to a narrow channel along one margin—a “keyhole” section. This explains the narrow streaks that are the common representation of the small intestine in radiographs obtained after the administra-
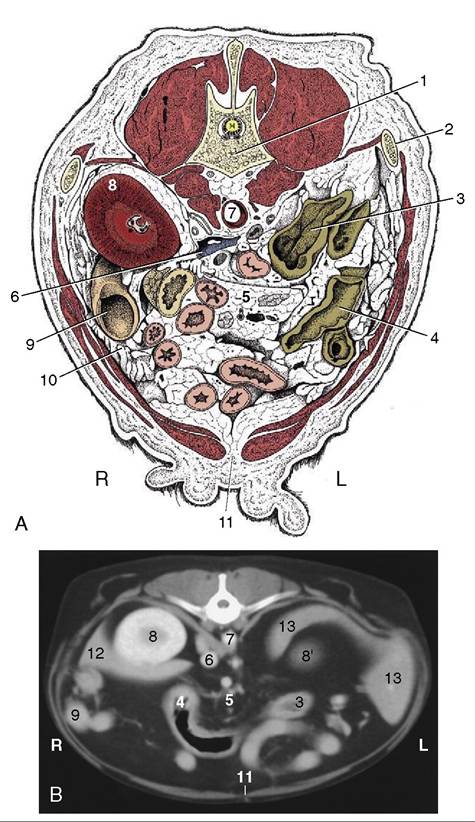
Figure 14-16 A, Transverse section of the canine abdomen at the level of the first lumbar vertebra.
B, Corresponding computed tomographic (CT) image slightly more caudal than A; the dog was lying on its back during the CT procedure. 1, First lumbar vertebra; 2, last rib; 3, descending colon; 4, transverse colon; 5, lymph nodes and blood vessels in mesentery; ventral to them is the jejunum; 6, caudal vena cava; 7, aorta, between crura of diaphragm; 8, right kidney; 8', cranial pole of left kidney; 9, descending duodenum and pancreas; 10, greater omentum; 11, linea alba; 12, liver; 13, spleen.tion of a barium meal. Segmental and peristaltic movements continually alter the configuration in life. After the administration of a contrast medium, the duodenum of the cat often displays segmental contractions that are sufficiently pronounced to divide the gut content into a linear series of globular expansions separated by (more or less) empty regions; this creates the very striking “pearl necklace” effect (Figure 14-14, B). A similar
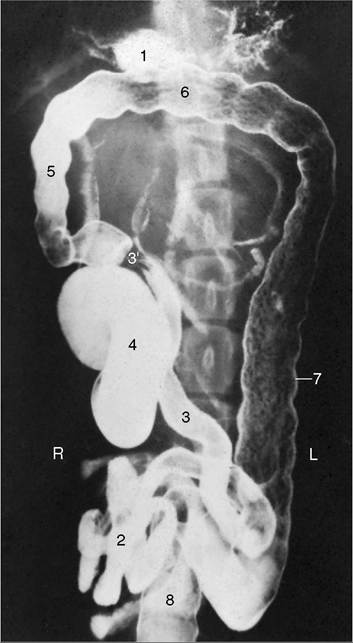
Figure 14-17 Ventrodorsal radiographic view of the canine abdomen after administration of a barium suspension. 1, Residue of barium in stomach; 2, jejunum; 3, ileum; 3,, ileocolic junction; 4, cecum; 5-7, ascending, transverse, and descending colon; 8, rectum.
appearance in other regions of the cat’s bowel, or in the duodenum of the dog, is probably evidence of abnormality.
The ileocecocolic junction is peculiar in that the ileum and colon are in line and form a continuous tube that is joined by the cecum to one side. (In the other species it is the cecum and colon that meet end-to-end.) The cecum is short, although it is of varying length, and twisted (Figure 14-15ZSurprisingly, it can be located on palpation by reference to the firm ileoce- cocolic junction at the level of the fourth lumbar vertebra. The firmness can be mistaken for a tumor or intussusception (Figure 14-19Z√).
The colon, 65 cm long on average, is only slightly wider than the small intestine.
It is easily recognized by its course cranial to the root of the mesentery and its nearly straight descent on the left toward the pelvis, which it enters dorsal to the bladder (and uterus) (see Figure 3-45 and Figure 14-17). The short ascending part lies to the right, between the descending duodenum and the root of the mesentery, and generally makes contact with the pyloric part of the stomach. Its narrow mesocolon permits it little mobility. The transverse colon runs from right to left, cranial to the root of the mesentery and ventral to the left lobe of the pancreas (see Figure 14-15). It is more loosely attached and sinks within the abdomen; usually it is the lowest part of the colon when depicted in lateral radiographs. The free attachment sometimes allows it to fold on itself to appear as no more than a flexure connecting the ascending with the descending colon. The descending colon is by far the longest segment. It passes caudally, to the left of the mesenteric root, to reach the pelvic cavity, where it continues as the rectum (Figure 14-7, AZb). It is related dorsally to the left kidney and sublumbar muscles and ventrally to the jejunal mass; it may lie against the left abdominal wall (Figures 14-13Z√ and 14-18Z√). The descending colon is the only segment of the large intestine of the dog that may easily be palpated. No part of the colon lies retroperitoneal.The prominence of the cecum and colon in plain radiographs of the canine abdomen is determined by the amount of gas and the nature and volume of the digestive residues present (see Figure 14-17). The cecum almost always contains sufficient gas to provide a reminder of the twisted course of its lumen. This convenient identifying feature is not found in cats, in which the simpler conformation rarely allows gas to be retained; see Figure 14-19, which also depicts the cat’s colon.
The blood supply of the intestines comes mainly from the cranial and caudal mesenteric arteries; in addition, a part of the duodenum is supplied by the cranial pancreaticoduodenal branch of the gastroduodenal artery (from the celiac artery).
The details are shown in Figure 14-20. The descending colon and rectum receive blood from the caudal mesenteric artery that, in both cats and dogs, branches off the aorta near the fifth lumbar vertebrae. The veins form the portal vein, with the exception of those from the caudal rectum that are directed toward the caudal vena cava.Several colic lymph nodes lie within the curvature of the ascending and transverse colon. The more prominent jejunal nodes lie high in the root of the mesentery;
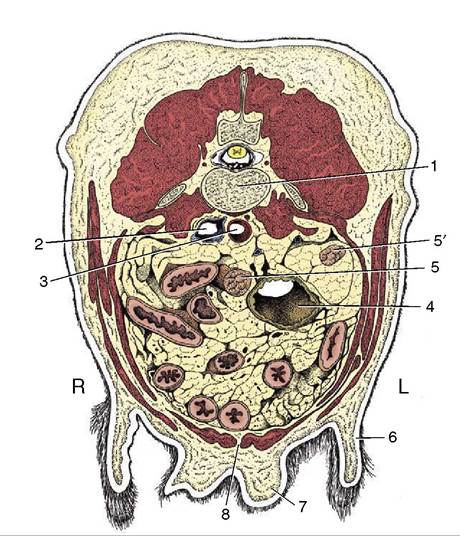
Figure 14-18 Transverse section of the canine abdomen at the level of the fourth or fifth lumbar vertebra. 1, Lumbar vertebra; 2, caudal vena cava; 3, aorta; 4, descending colon; 5, 5', right and left uterine horns; 6, flank fold; 7, mammary gland; 8, linea alba.
one, surprisingly large (perhaps 10 cm in the beagle), accompanies the jejunal arteries (Figure 14-16Z5). Several smaller caudal mesenteric nodes lie within the descending mesocolon, scattered about the branches of the caudal mesenteric artery.