THE STOMACH
The dog has a simple stomach (see also pp. 123-129) that exhibits the idealized form described on page 125 only when moderately full. The fundus and body merge smoothly and are capable of great expansion, while the cylindrical and thicker walled pyloric part is less able to enlarge.
The fundus projects dorsally to the left of the cardia, against the liver. The cardia is generally wide, and this may be related to the ease with which dogs vomit. The pylorus, on the other hand, is narrow, and pyloric stenosis is not uncommon in the young. When the organ is quite empty, the body also becomes more or less cylindrical, and the fundus then forms a bulbous dorsal enlargement. When the organ is greatly distended, all parts except the pyloric canal merge in a common sac. The capacity of the stomach ranges from 0.5 to 6.0 L with the average about 2.5 L; it is thus relatively large in relation to body size.The position and relations obviously depend on the degree of fullness; the cardia provides a fixed point opposite the ninth intercostal space. The fundus and body lie mainly to the left of the median plane, in contact with the diaphragm and liver, respectively, but the ventral part of the body crosses to the right before being continued by the pyloric part, which also lies against the liver (Figure 14-11/3,4,7); indeed, its lesser curvature is bound to the porta of the liver by the lesser omentum. The greater curvature faces mainly to the left, toward the spleen, and ventrally, where it usually lies on the ventral fringe of the liver and on the falciform ligament (Figure 14-11/d); it reaches the abdominal floor only when the stomach is greatly distended, and in these circumstances it may be palpated through the abdominal wall. Otherwise, the stomach is out of reach and aligned with the ninth to twelfth ribs of the left side (or thereabouts; Figure 14-12, A).
As the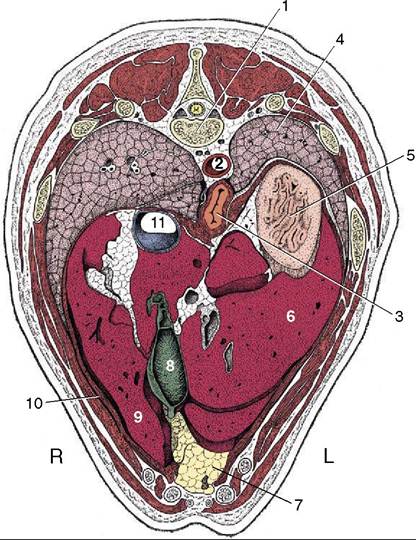
Figure 14-10 Transverse section of the canine trunk at the level of the eleventh thoracic vertebra. 1, Eleventh thoracic vertebra; 2, aorta; 3, esophagus; 4, left lung; 5, fundus of stomach; 6, left lateral lobe of liver; 7, fat-filled falciform ligament; 8, gallbladder; 9, right medial lobe of liver; 10, diaphragm; 11, caudal vena cava.
stomach expands, its ventral parts (mainly the body) move Caudoventrally into broad contact with the abdominal floor and left costal arch, displacing the jejunum from contact with the liver in the process. Excessive distention, not uncommon in this greedy species, may carry the stomach to a level behind the umbilicus. Such gross enlargement also alters its cranial relationships, pushing the liver to the right and the diaphragm forward, reducing the thoracic cavity.
Survey radiographs of the abdomen generally reveal few details of the stomach beyond the gas that naturally collects in the uppermost part of the organ—the fundus in the animal standing or in right lateral recumbency. This useful orientation feature is lost when the animal is placed in other positions. A more complete demonstration of the topography is obtained with the administration of a barium meal (Figure 14-12). The existence of the rugae may be revealed by defects in the outline of the contrast mass; the most satisfactory depiction is obtained after the evacuation of the bulk of the meal, when the residual agent clings to the mucosa and fills the spaces between adjacent rugae.
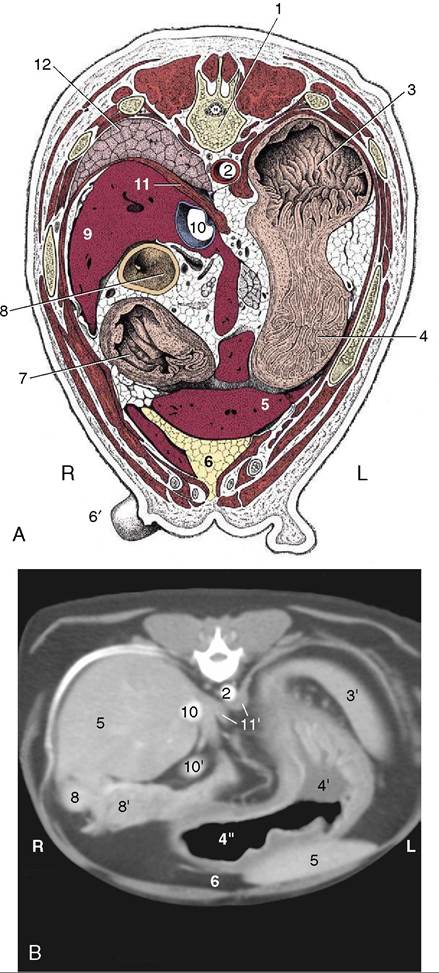
Figure 14-11 A, Transverse section of the canine trunk at the level of the twelfth thoracic vertebra. B, Corresponding computed tomographic (CT) image slightly more caudal than A; the dog was lying on its back during the CT procedure. 1, Twelfth thoracic vertebra; 2, aorta; 3, fundus of stomach; 3', spleen; 4, body of stomach; 4’, with fluid; 4", with gas; 5, liver; 6, fat-filled falciform ligament; 6', teat; 7, pyloric part of stomach; 8, descending duodenum; 8', right lobe of pancreas; 9, caudate process of liver; 10, caudal vena cava; 10', portal vein; 11, diaphragm; 11', crura of diaphragm; 12, right lung.
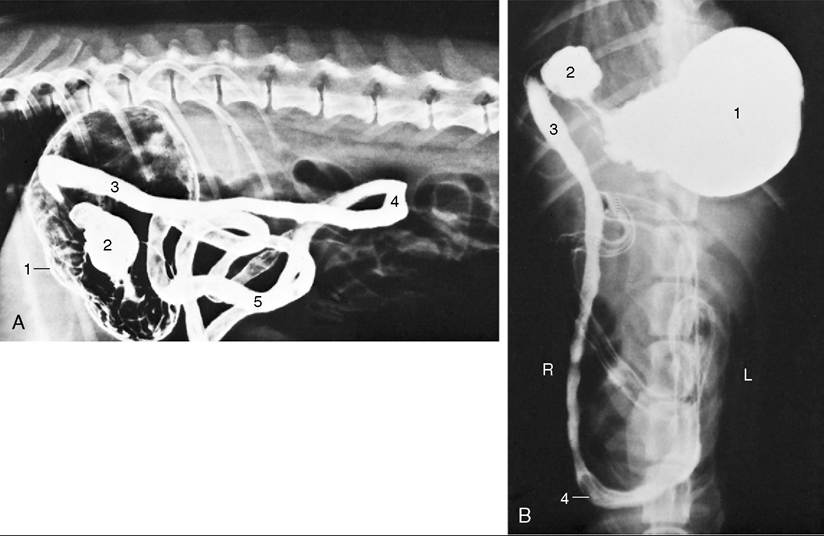
Figure 14-12 Lateral (A) and ventrodorsal (B) radiographic views of the canine abdomen after administration of a barium suspension.
1, Stomach; 2, pyloric part; 3, descending duodenum; 4, caudal flexure of duodenum; 5, jejunum.A number of structures join the stomach to neighboring parts. The fundus is directly bound to the left crus of the diaphragm (gastrophrenic ligament), while there are looser attachments between the cardia and the diaphragm, the lesser curvature and liver (lesser omentum), and the greater curvature and spleen (greater omentum). Except at these reflections, the stomach is completely covered with serosa.
The stomach receives blood from all three branches into which the celiac artery divides directly after leaving the aorta between the crura of the diaphragm. The branches to the stomach therefore approach from the right of the fundus and dorsal to the cardia (Figure 14-9). The splenic artery supplies short branches as it crosses the caudal surface of the fundus before reaching the spleen. A more substantial branch (left gastroepiploic artery; Figure 14—9/11) follows the greater curvature to an anastomosis with the right gastroepiploic artery (a branch of the hepatic artery). The left gastric artery (Figure 14—9/5) supplies the fundus, cardiac region, and a branch to the esophagus before following the lesser curvature to an anastomosis with the right gastric artery (Figure 14—9/5), a further branch of the hepatic artery. The arterial arcades that follow the curvatures supply fair-sized branches to adjacent parts of both surfaces. The arteries are mostly accompanied by satellite veins, which contribute as gastrosplenic and gastroduodenal veins to the portal vein. Gastric lymphatics drain into hepatic lymph nodes but may have passed the splenic and gastric nodes first. Large vessels are absent from the strips midway between the curvatures, which are therefore the preferred locations for incision. The parietal surface can be exposed and opened through a midline or paracostal incision (a common procedure for the recovery of foreign bodies), but the visceral surface is inaccessible unless the omental bursa is opened first (see p.
122).Gastric volvulus is relatively common, especially in large deep-chested breeds. In this mishap the distended stomach rotates about the esophagus (usually in a clockwise direction as seen from behind, between 270° and 360°), and this closes the esophagus at the cardia. The pyloric end of the stomach, less firmly held in place by the lesser omentum and bile duct, moves ventrally and to the left, which stretches the cranial part of the duodenum across the ventral surface of the cardia. The ventral leaf of the greater omentum, still attached to the greater curvature of the stomach, covers the ventral aspect of the displaced stomach and is visible when entering the abdominal cavity at the time of surgery. The rotation compresses the veins, which causes congestion of the stomach and engorgement of the spleen. The position of the spleen varies depending on the degree of volvulus, and it may even rotate on its own pedicle.
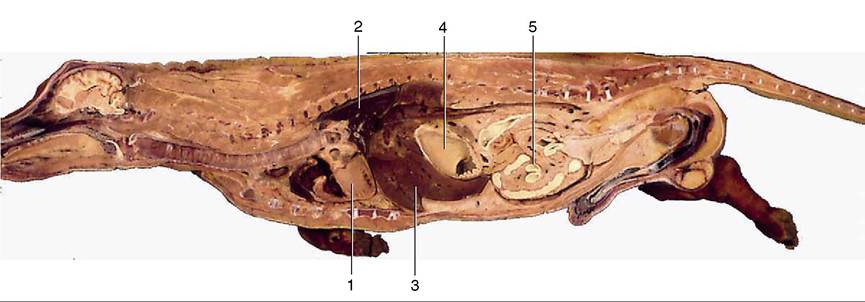
Figure 14-13 Median section of canine trunk, providing overview of viscera. 1, Heart; 2, lung; 3, liver; 4, stomach; 5, intestine.
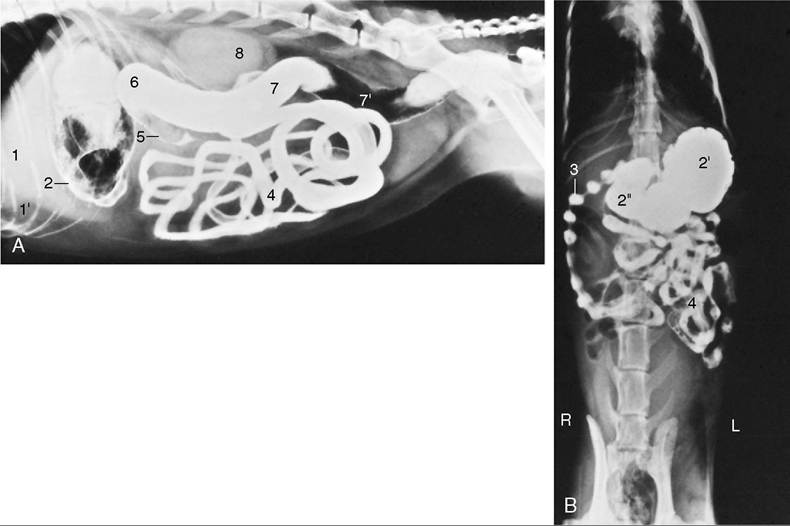
Figure 14-14 Lateral (A) and ventrodorsal (B) radiographic views of the feline abdomen after administration of a barium suspension. 1, Liver; 1', fat-filled falciform ligament elevating the liver; 2, gas and barium in stomach; 2’, fundus; 2", pyloric part of stomach; 3, descending duodenum—the striking "string-of-pearls" appearance (characteristic of cats) is due to segmental peristalsis; 4, jejunum; 5, ascending colon; 6, transverse colon; 7, descending colon; 7, gas in descending colon; 8, kidneys (superimposed).
Counterclockwise rotation of the stomach is possible to a maximum of 90°; the pylorus and antrum move dor- sally along the right abdominal wall, and in this case, there is no displacement of the omentum over the ventral surface of the stomach.
The stomach of the cat is more sharply flexed on itself, and the pyloric part reaches little, if at all, into the right half of the abdomen. Gross distention is also less common in cats, which tend to moderate their appetites better than dogs. The cat’s stomach is generally similar to that of the dog; its topography and that of the intestines are shown in the radiographs of Figures 14-13, 14-14, and 14-6). The rugae in the stomach as seen in contrast radiographs are conspicuously fewer and proportionately smaller in cats than in dogs. Pyloric stenosis caused by hypertrophy of the pyloric circular smooth muscle can be encountered in Siamese cats.