THE LIVER
The liver (see also pp. 135-139) is relatively large, weighing about 450 g on average, and accounts for 3% to 4% of the body weight. It is almost entirely intrathoracic, occupying a central position with only a slight bias to the right side (Figure 14-7Z2 and Figure 14-10).
The modest asymmetry is caused by the enlargement of the caudate process beneath the last ribs, where it makes contact with the right kidney (Figure 14-11Z9). The ventral border extends across the costal arches and would be palpable were it not for the fat within the falciform ligament and the taut rectus muscles. Even so, it may be appreciated when significantly enlarged. The liver in dogs and cats is deeply divided by fissures extending from the ventral margin; the pattern, the relative extents, and the names of the lobes may be obtained from Figure 3-53.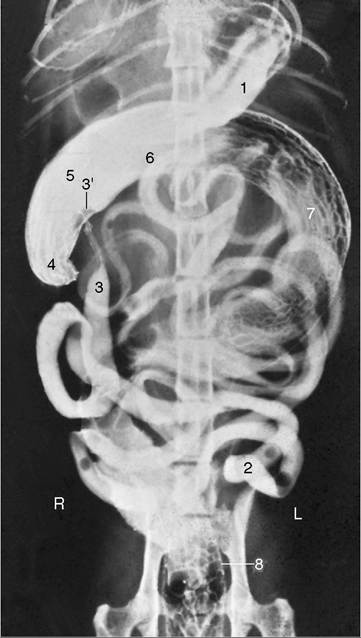
Figure 14-19 Ventrodorsal radiographic view of the feline abdomen after administration of a barium suspension. 1, Residue of barium in stomach; 2, jejunum; 3, ileum; 3', ileal papilla; 4, cecum; 5-7, colon—the long descending part (7) has curved far to the right in this animal; 8, rectum.
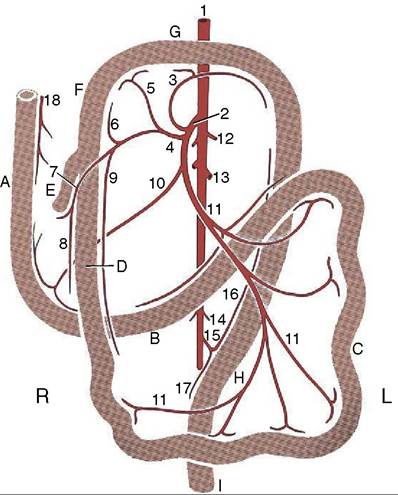
Figure 14-20 The blood supply of the intestinal tract, ventral view; schematic. A, Descending duodenum; B, ascending duodenum; C, jejunum; D, ileum; E, cecum; F, ascending colon; G, transverse colon; H, descending colon;, rectum. 1, Abdominal aorta; 2, cranial mesenteric a.; 3, middle colic a.; 4, ileocolic a.; 5, right colic a.; 6, colic branch of ileocolic a.; 7, cecal a.; 8, antimesenteric ileal branch; 9, mesenteric ileal branch; 10, caudal pancreaticoduodenal a.; 11, jejunal aa.; 12, phrenicoabdominal aa.; 13, renal aa.; 14, testicular (ovarian) aa.; 15, caudal mesenteric a.; 16, left colic a.; 17, cranial rectal a.; 18, cranial pancreaticoduodenal a.
The cranial surface conforms to the curvature of the diaphragm with which it is in extensive contact and to which it is secured by the caudal vena cava embedded in the dorsal border. The attachment to the tendinous center of the diaphragm is completed by right and left coronary ligaments caudolateral to the vein. Most of the liver can therefore be retracted at operation to expose the diaphragm. The gallbladder is sunk deeply between the lobes, just to the right of the median plane opposite the eighth intercostal space; it usually makes contact with the diaphragm and always appears at the visceral surface, although it is too short to reach the ventral border (Figure 14-10Zof less extreme conformation. Dorsal displacement of the liver, away from the abdominal floor, may be encountered in cats that are overindulged; it is due to the deposition of excessive fat within the falciform ligament.
THE PANCREAS sel and course through the pancreatic tissue to supply the gut itself. Anastomoses between these various vessels occur within the gland. Lymphatics are abundant and drain into the duodenal lymph node if present or into the mesenteric lymph nodes.
One of the most encountered problems in the pancreas of the dog is the presence of an insulin-producing tumor, an insulinoma. Thorough inspection for metastases must be performed in the liver, the duodenum, the mesentery, and the hepatic, splenic, gastric, duodenal, and cranial mesenteric lymph nodes. Resection of the part of the pancreas is difficult because the blood supply is shared with the duodenum and the spleen. Removal of the spleen is indicated when the splenic artery cannot be preserved.
The slender pancreas (see also pp. 139-140) consists of two limbs or lobes that diverge from the vicinity of the pylorus. The left lobe is directed caudomedially and crosses the median plane behind the stomach to end against the left kidney (see Figure 3-56/5). It divides the branches of the celiac artery from those of the cranial mesenteric and is enclosed within the deep leaf of the greater omentum where this passes dorsal to the transverse colon.
Its dorsal surface is crossed by the portal vein, where it makes contact with the hilus of the liver to the right of the median plane.The longer right lobe is directed caudodorsally and follows the dorsal surface of the descending duodenum within the mesoduodenum. It is related dorsally to the visceral surface of the liver and, behind this, to the ventral surface of the kidney (Figure 14-16/9). It lies lateral to the ascending colon and dorsal to the small intestine.
Two secretory ducts open into the duodenum where the two lobes diverge. The smaller and inconstant pancreatic duct joins the bile duct just before this opens on the major duodenal papilla, 3 to 6 cm distal to the pylorus. The accessory pancreatic duct, the main channel, opens on the minor duodenal papilla 3 to 5 cm farther down the gut. Both papillae can be detected with the unaided eye. The duct systems of the two lobes communicate internally. In the cat the main duct is the pancreatic duct; in a minority of cats (around 20%) an accessory duct can also be found. When present, it opens onto the minor duodenal papilla, as in dogs, some 2 cm distal to the major papilla.
The major part of the pancreas is supplied by two of the three branches of the celiac artery; only the caudal part of the right limb receives blood from the cranial mesenteric artery. The left lobe is entered by branches of the splenic artery; branches from the hepatic artery supply the body of the pancreas (gastroduodenal artery) and the cranial half of the right lobe (cranial pancreaticoduodenal artery). Duodenal branches are given off