THE ADNEXA OF THE EYE
The structures that protect and move the eyeball include the orbital fasciae, the ocular muscles, the eyelids and tunica conjunctiva, and the lacrimal apparatus; most are contained within the orbit.
This is a cone-shaped cavity on the lateral surface of the skull that is delimited externally by a bony margin (base of cone). In the carnivores and pig the bone is deficient laterally but the ring is completed by the orbital ligament (see Figure 2-31/1). The wall of the human orbit is entirely osseous, but in the domestic mammals the lateral and ventral parts are formed by the fibrous periorbita, one of the orbital fasciae (see further on).The Orbital Fasciae
The eyeball is surrounded by three roughly conical fascial layers. The most external of these is the periorbita, which has just been mentioned; internal to the periorbita are superficial and deep muscular fasciae (Figure 9-16).
The periorbita is attached near the optic foramen at the apex of the cone. It blends with the periosteum at the orbital margin and on the medial and dorsal walls
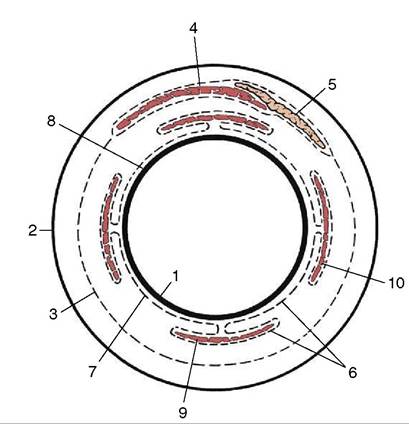
Figure 9-16 Schematic representation of the orbital fasciae: transection of orbital structures at the level of the eyeball. Part of the deep fascia (6) forms the vagina bulbi (7). 1, Eyeball; 2, periorbita; 3, superficial muscular fascia; 4, levator palpebrae; 5, lacrimal gland; 6, deep muscular fascia; 7, vagina bulbi; 8, episcleral space; 9, ventral rectus muscle; 10, lateral rectus muscle.
of the orbit. Elsewhere (mainly laterally and ventrally) it is free and forms a substantial fibrous partition between orbital and extraorbital structures (Figure 9-17/11). The periorbita splits at the orbital margin. One part is continued as the periosteum of the facial
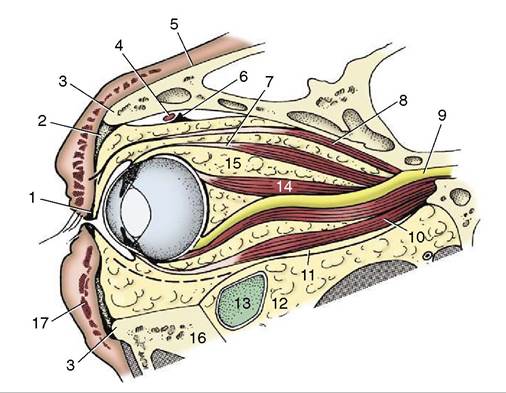
Figure 9-17 Right bovine eye cut along orbital axis, rostro- medial surface.
1, Tarsus; 2, orbital septum; 3, orbital margin; 4, dorsal oblique muscle; 5, periosteum of face; 6, trochlea; 7, dorsal rectus muscle; 8, levator palpebrae superioris; 9, optic nerve in optic foramen; 10, ventral rectus muscle; 11, periorbita; 12, extraperiorbital fat; 13, lacrimal bulla, a caudal recess of the maxillary sinus; 14, retractor bulbi; 15, intraperiorbital fat; 16, zygomatic arch; 17, orbicularis.bones; the other, the orbital septum (Figure 9-17/2), forms two semilunar folds with thickened free margins (tarsi) that stiffen the edges of the upper and lower eyelids. The trochlea (Figure 9-17/6), a flat piece of cartilage embedded in the dorsomedial wall close to the orbital margin, provides a pulley around which the dorsal oblique muscle winds to change direction by nearly 90°.
The superficial muscular fascia lies within the periorbita; it is loose and fatty and envelops the levator palpebrae superioris and the lacrimal gland (Figure 9-16/5). The deep muscular fascia is more fibrous; it arises from the eyelids and from the limbus of the eyeball, which it closely invests. It is reflected around the muscles attaching to the eyeball, providing each (and also the optic nerve) with a fascial envelope. It is known as the vagina bulbi (Figure 9-16/7) where it is applied to the eyeball, although it is separated by a narrow episcleral space. The presence of this space facilitates the movement of the eyeball against the retrobulbar fat. In enucleation (removal of the eye), advantage is usually taken of this arrangement; the eyeball is freed, and the vagina bulbi and the retrobulbar structures it covers are left in place.
The Muscles of the Eyeball
The muscles that move the eye are located behind the eyeball. All except one originate in the vicinity of the
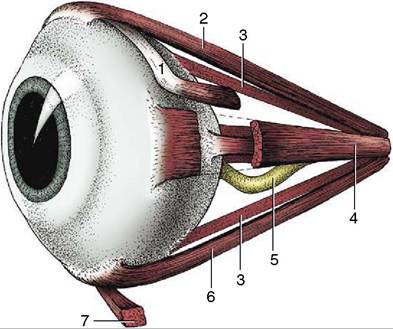
Figure 9-18 Ocular muscles. 1, Dorsal oblique m.; 2, dorsal rectus m.; 3, retractor bulbi; 4, medial rectus m.; 5, optic nerve; 6, ventral rectus m.; 7, ventral oblique m.
optic foramen at the apex of the orbital cone. There are four rectus muscles, two oblique muscles, and a retractor.
The four rectus muscles—dorsal, ventral, medial, and lateral—are inserted anterior to the equator by wide but very thin tendons (see Figure 9-7). The dorsal and ventral oblique muscles attach to the eyeball near the equator and tend to rotate the eyeball around the visual axis on contraction (Figure 9-18/7,7). The dorsal oblique muscle also arises close to the optic foramen and passes forward on the dorsomedial wall of the orbit before it is deflected around the trochlea to end on the dorsolateral surface of the eyeball beneath the tendon of the dorsal rectus muscle. A small synovial sheath protects the muscle as it passes around the trochlea, which in fact is its functional origin. If this muscle were to contract by itself, it would pull the dorsal part of the eyeball medially.
The ventral oblique muscle, uniquely, does not arise from the vicinity of the optic foramen. Instead, it takes its origin from a depression in the ventromedial wall of the orbit, passing laterally below the eyeball and the tendon of the ventral rectus muscle before inserting on the ventrolateral part of the eyeball. Its contraction, if isolated from the action of the other muscles, would rotate the eyeball around the visual axis so that the dorsal portion of the eyeball would move laterally. The retractor bulbi (Figure 9-17/74) arises from the vicinity of the optic foramen but is inserted on the eyeball posterior to the equator. It forms a nearly complete muscular cone about the optic nerve (Figure 9-19/7). The retractor is not present in ourselves, and it is still a matter of conjecture why we do not possess the ability to retract our eyes; perhaps we do not need the
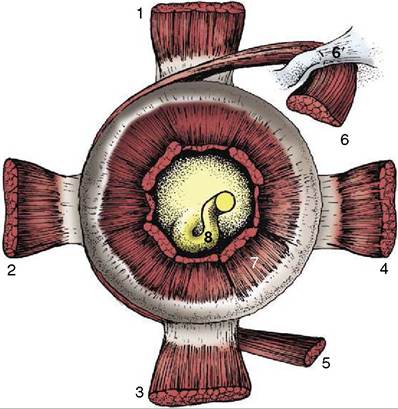
Figure 9-19 Stumps of ocular muscles viewed from behind the left eyeball. 1, Dorsal rectus m.; 2, lateral rectus m.; 3, ventral rectus m.; 4, medial rectus m.; 5, ventral oblique m.; 6, dorsal oblique m.; 6', trochlea; 7, retractor bulbi; 8, optic nerve.
additional protection provided to the more protruding eyes of animals.
The movements of the eyes are much more complex than the origins and insertions of the individual muscles suggest. As far as we know, none ever acts singly. It seems that the tonus is increased or decreased in opposing groups for smooth transition from one eye position to another. The most difficult actions to explain are those of the oblique muscles because there is no significant rotation around the visual axis in any usual movement. Their participation is required for the following reason. The rectus muscles arise slightly medioventral to the point where the visual axis, if extended caudally, would strike the skull. That is, the visual axis does not coincide with the axis of the orbital cone. As a result, the dorsal rectus muscle, as one example, would not simply elevate the cranial pole of the eyeball but would also rotate the eyeball so that its dorsal part moved slightly medially. This slight intorsion is reflexively resisted by the ventral oblique, and the result is a smooth elevation of the anterior pole. The reverse happens in depression of the eyeball when the ventral rectus and the dorsal oblique muscles are involved.
An additional striated muscle within the orbit is conveniently considered here. This is the levator palpebrae superioris (Figure 9—17/8). It does not attach to the eyeball but passes over it to enter and elevate the upper eyelid.
In addition to these striated muscles there are three sheets of smooth muscle, although they are rarely observed during routine dissection. One (m. orbitalis) consists of a sheet of circular (with regard to the visual axis) fibers applied to the internal surface of the periorbita. A ventral longitudinal sheet extends from the sheath of the ventral rectus muscle into the lower lid (as the m. tarsalis inferior) and into the third eyelid (see further on). A medial longitudinal sheet extends from the sheath of the medial rectus muscle and from the trochlea into the upper eyelid (as the m.
tarsalis superior) and into the third eyelid. Tonus in these sheets maintains the normal protruded position of the eye and retracted position of the eyelids.The Eyelids and Conjunctiva
The eyelids (palpebrae) are two musculofibrous folds of which the upper is the more extensive and more mobile. The free margins of the lids meet at the medial and lateral angles of the eye and bound an opening known as the palpebral fissure.
The eyelids consist of three layers: skin, a middle musculofibrous layer, and a mucous membrane, known as the palpebral conjunctiva, facing the eye (Figure 9-20).
The skin of the lids is thin and delicate and is covered with short hairs; it may also carry a few prominent tactile hairs.
The musculofibrous layer is formed by the orbicularis oculi, the orbital septum, the aponeurosis of the levator muscle, and the smooth tarsal muscle. The orbital septum arises from the margin of the orbit; the aponeurosis of the levator and the tarsal muscle originate in the orbit. Except for the orbicularis oculi, which lies directly under the skin and can be dissected away, the components of this layer intermingle inseparably. Toward the free margin these components are succeeded by the tarsus (Figure 9-20/2'), a platelike fibrous condensation that stabilizes the edge of the lid. The ends of the two tarsi are anchored to the orbital margin by medial and lateral palpebral ligaments that assure an elongated palpebral fissure when the eye is closed (by the orbicularis oculi). Deep to the tarsus and opening onto the edge of the lid by a row of tiny openings is a series of tarsal glands (Figure 9-20/6) that secrete a fatty material. Just in front of these glandular openings are the cilia (eyelashes), which are usually more prominent and numerous on the upper than on the lower lid; conspicuous cilia are absent from the lower lid of carnivores. Small ciliary and sebaceous glands are associated with the roots of the cilia; the common stye (hordeolum) is an inflammation of one of these glands.
The posterior surface of the lid is lined with conjunctiva, a thin, transparent mucous membrane. The palpebral conjunctiva is reflected at the base of the lids to continue on the sclera as the bulbar conjunctiva, which ends at the limbus, although the epithelium continues
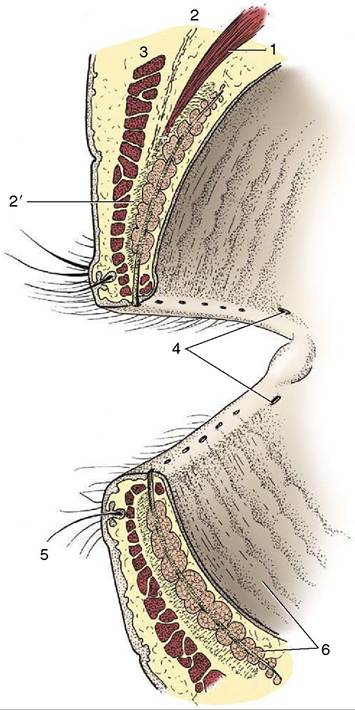
Figure 9-20 Eyelids, sectioned and viewed obliquely from behind. 1, Levator palpebrae superioris; 2, orbital septum; 2', tarsus; 3, orbicularis oculi; 4, puncta lacrimalia; 5, cilium with associated ciliary and sebaceous glands; 6, tarsal glands.
as the anterior epithelium of the cornea. The potential space between the lids and the eyeball is known as the conjunctival sac, and their dorsal and ventral extremities are the fornices (Figure 9-3/2). The transparency of the conjunctiva renders the smaller blood vessels visible, especially when they are congested in infections. Those in the bulbar conjunctiva move with this loosely attached layer; the deeper scleral vessels do not. Advantage is taken of this arrangement to distinguish inflammation of the conjunctiva from that of deeper structures. A pale conjunctiva suggests anemia, shock, or internal hemorrhage.
A slight mucosal elevation, the lacrimal caruncle, is present in the medial angle of the eye; it bears a few fine hairs in the large species (Figure 9-21/2).
Between the lacrimal caruncle and the eyeball is a dorsoventrally oriented conjunctival fold known as the third eyelid (Figure 9-21/6). Unlike a true lid, it is covered with conjunctiva on both sides and is invisible
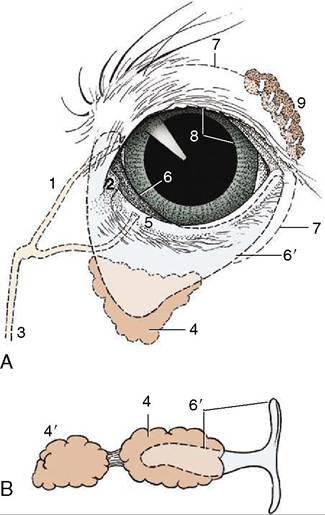
Figure 9-21 A, Left eye of dog showing third eyelid and lacrimal apparatus. B, Isolated cartilage of the third eyelid and associated glands of a pig. 1, Upper canaliculus; 2, lacrimal caruncle; 3, nasolacrimal duct; 4, gland of third eyelid; 4', deep gland of third eyelid; 5, punctum lacrimale; 6, third eyelid; 6', cartilage of third eyelid; 7, position of conjunctival fornix; 8, pupil; 9, lacrimal gland.
when the eye is closed. The third eyelid is supported by a T-shaped piece of cartilage (Figure 9-21/6') whose bar lies in the free edge of the fold and whose stem points backward into the orbit medial to the eyeball. The stem of the cartilage is surrounded by an additional lacrimal gland, the gland of the third eyelid; pigs and cattle also have a second, deeper gland. The secretion of these glands enters the conjunctival sac on the bulbar surface of the third eyelid. The third eyelid is kept retracted by smooth muscle (m. orbitalis) under sympathetic influence. It slides over the eyeball when the latter is retracted or pushed into the orbit. The lid, in conjunction with the retractor bulbi muscle, is thought to provide added protection to the protruding eyes of animals.
The Lacrimal Apparatus
This consists of the lacrimal gland proper, the gland(s) associated with the third eyelid, several small accessory glands, and a duct system that conveys the lacrimal fluid (tears), after it has washed over the eye, into the nasal cavity for evaporation. The lacrimal gland is flat and lies between the eyeball and the dorsolateral wall of the orbit (Figure 9-21/9). Its secretion is drained by many minute ducts into the dorsal fornix of the conjunctival sac, where it mixes with the secretions of the lesser glands. Blinking movements distribute the lacrimal fluid over the exposed part of the eye, which is thus kept moist; the tears carry away foreign material and supply the cornea with some nutriment. The fluid, being repelled by the fatty secretion of the tarsal glands along the edge of the lids, is normally pooled at the medial angle of the eye in the so-called lacrimal lake, a shallow depression surrounding the lacrimal caruncle, before being drawn by capillary action into the duct system through the puncta lacrimalia (Figure 9-20/4). Lacrimal fluid escapes onto the face only when produced in excessive amounts or when normal drainage is impaired.
The puncta lacrimalia are minute slits, one on the edge of each lid next to the caruncle. Each punctum leads to a short, narrow canaliculus through which the fluid flows to the much longer nasolacrimal duct (Figure 9-21/5). The beginning of the nasolacrimal duct is slightly enlarged, forming the lacrimal sac, which occupies a funnel-shaped fossa near the bony margin of the orbit. The nasolacrimal duct runs rostrally, at first within the thickness of the maxilla, then on its internal surface where it is covered by nasal mucosa. In some species it ends at the nostril, in others more deeply in the nasal cavity.
The tear film washing the eye consists of three layers. The outermost lipid layer is derived from the secretion of the tarsal glands; it helps spread the tears evenly and retards the breakup of the film. The thick middle aqueous layer is derived from the lacrimal glands; it moistens and nourishes the cornea. The innermost mucinous layer is produced by goblet cells in the conjunctiva and holds the tear film intimately to the cornea. Tear flow can be increased by drugs or reflexively after stimulation of the conjunctiva, cornea, or nasal mucosa. Weeping as an expression of emotion is a purely human phenomenon.