THE ANATOMY OF RECTAL EXPLORATION
Exploration per rectum is an important diagnostic technique in the horse. A hand can very easily be introduced into the rectum and descending colon and then be passed in various directions to examine the pelvic and caudal abdominal wall, the pelvic contents, and a variable amount of the abdominal contents (Figure 22-23/7).
Rectal examinations are not free from risk of injury to the mucosa or even, in extreme cases, of perforation of the intestinal wall—a mishap most likely to occur when invasion of the rectum induces straining. The novice should not attempt the procedure without appropriate supervision. Some organs can always be identified with certainty and others less consistently, for the results of the investigation depend not only on the relative sizes of the investigator and patient but also on the condition of the organs. It is one thing to palpate an organ through the gut wall and quite another to recognize enough of its nature to be confident of identification. The greater part of the pelvic skeleton can be identified with absolute certainty, although the part of the floor about the symphysis may be made inaccessible by overlying organs. The caudal part of the abdominal wall is also within reach, although it rarely reveals much of interest other than the caudal margin of the internal oblique muscle bordering the deep inguinal ring and the vaginal ring (Figure 22-24/1) within that opening. The vaginal ring can be recognized most easily in the stallion, in which the deferent duct may be picked up where it lies on the bladder and traced to its disappearance.Of the viscera, the small colon is the most easily recognized because its identity is betrayed by the chain of sacculations that are usually filled with firmish feces; even when empty, this part of the gut can be distinguished by single tenia following the free border (the tenia along the opposite mesenteric border is not normally palpable).
Although the small colon has a mobile disposition, a mass of coils is generally found just in front of the pelvic inlet and mainly to the left. A considerable part of the ascending colon is also within reach. The pelvic flexure, the part most easily identified, is usually found immediately before or even within the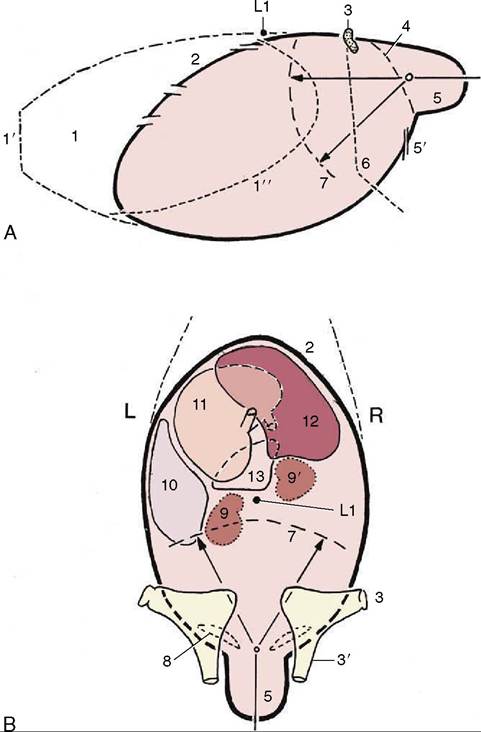
Figure 22-23 Drawings of the abdominal and pelvic cavities in left lateral (A) and dorsal (B) outline, indicating the scope of rectal exploration. The dorsal outline encloses a ring of the relatively fixed organs (9, 9', 10, 11, 12) with the pancreas (13) in the center. 1, Thoracic cavity; 1', thoracic inlet; 1", costal arch; 2, diaphragm; 3, coxal tuber; 3', shaft of ilium; 4, terminal line; 5, pelvic cavity; 5', inguinal canal; 6, thigh and stifle; 7, approximate range in rectal palpation in the median plane (A) and directly ventral to the kidneys (B); 8, deep inguinal ring; 9, 9', left and right kidneys; 10, spleen; 11, stomach; 12, liver; 13, pancreas.
pelvic cavity. Most often it lies just to the left of the median plane but it may cross to the right. The adjoining parts of the left ventral and dorsal parts of the ascending colon can be followed for some distance. They are most easily recognized when gas-filled, as this emphasizes the contrast between the sacculations of the wide ventral part and the smooth surface of the narrower dorsal part. Although the names of these parts are indicative, it must not be assumed that they necessarily lie directly one above the other. The dorsal dia-
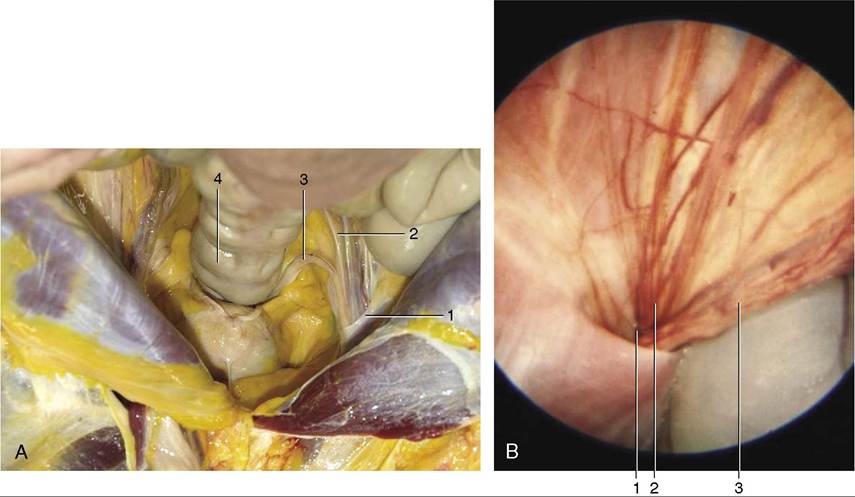
Figure 22-24 A, Dissection showing the vaginal ring. B, Endoscopic view of the ring. 1, Vaginal ring 2, testicular artery and vein 3, deferent duct; 4, descending colon.
phragmatic flexure and right parts of the colon are out of reach of even the longest arm, although sometimes it is just possible for the fingertips to touch and trace the junction of the ascending and transverse parts of the colon.
The base and the dorsal part of the body of the cecum are consistently within reach; however, unless they are inflated, little beyond position exists to identify them. The cranial mesenteric artery, adherent to the left face of the cecal base, may sometimes be identified when thickened by reaction to nematode larval invasion. Even in the most favorable circumstances it is barely within reach.Although much of the small intestine is accessible, it is usually impossible to identify it with certainty; the exception is the firmer terminal part of the ileum, which may be picked up as it approaches the medial aspect of the cecal base. Identification is easiest when it is impacted. When distended with gas the caudal flexure of the duodenum may be identified as it crosses the root of the mesentery.
A small horse and a long arm are the prerequisites if any of the contents of the cranial part of the abdomen are to be reached. The caudal pole of the left kidney may usually be felt, and it is theoretically possible to trace both ureters over the abdominal roof; in practice, healthy ureters cannot be identified. The caudal margin of the spleen is also accessible, although it may not always be appreciated; a greater part of this organ may be brought within reach when the stomach is distended.
An emergency means of euthanasia, of little relevance today, is available in transection of the abdominal aorta per rectum.
The bladder is invariably identifiable, regardless of its degree of filling and despite the fact that it is partly overlain by reproductive organs. In the mare, the vagina is distinguishable as a rather lax organ interposed between the rectum and the bladder; if followed forward, it leads to the somewhat firmer cervix. Beyond the cervix, the body of the uterus may be traced to its bifurcation, and the horns may then be followed laterally toward the ovaries. The dimensions and the texture of the uterus vary greatly with its state, and the experienced equine clinician can date an early pregnancy with quite remarkable precision by palpating the uterus. The ovaries are among the easiest organs to identify because they have a very characteristic shape and consistency. They are rather movable and are not always found exactly where expected. Only the largest follicles may be appreciated individually.
The pelvic urethra of the stallion is easily identified as a wide slack tube, although its outline is partly concealed by the associated glands (see Figure 22-20). The bulbourethral glands at the pelvic exit, the smooth pearshaped vesicular glands, the more knobby prostate, and the fusiform enlargements of the ampullae of the deferent ducts are almost always individually distinctive. Manipulation may stimulate the urethral muscle, which may firm the urethra and cause it to exhibit rhythmic contractions.