THE BLADDER AND FEMALE URETHRA
(See also pp. 181-184.)
Although the neck of the canine bladder extends a little way into the pelvic cavity, the bulk of the organ is visible as soon as the floor of the abdomen is removed, as it is not covered by the greater omentum (Figure 15-6).
Its size varies greatly and when excessively distended, as in house-trained animals denied opportunity for relief, it may reach to or even beyond the umbilicus (see Figure 15-27). In dogs allowed freedom, the bladder is rarely very large because the frequent discharge of urine performs a social (scent-marking) as well as eliminative function. The bladder may be identified on abdominal palpation when moderately (or more greatly) distended. Unless handled with care, a grossly distended bladder may rupture when compressed through the abdominal wall to induce micturition. The oblique passage of the ureters through the bladder wall normally affords protection against reflux of urine to the kidneys, but even cautious compression, if too long maintained, may overcome this protection and may cause the introduction of contamination from an infected bladder. A moderate increase in bladder size is not accompanied by increased tension, and radiographs obtained with the (contrasted) bladder in this state show its contours molded to those of adjacent organs (Figure 5-30). The organ is globular when the thick detrusor muscle is fully contracted.The peritoneal covering, which extends onto the cranial part of the urethra, is reflected into the usual lateral and ventral folds.
The bladder receives its blood supply through the cranial vesical artery, a branch of the umbilical artery, and the caudal vesical artery, an indirect branch of the internal iliac artery. The hypogastric nerve supplies the sympathetic innervation, the pelvic nerve (S1-S3) supplies the parasympathetic innervation, and the pudendal nerve (S1-S3), the somatic innervation.
The female urethra is relatively long. It originates within the cranial part of the pelvis and follows the symphysis to open on the floor of the vestibule, immediately caudal to the vestibulovaginal junction. In the bitch, the orifice is raised on a tubercle that continues some way over the vestibular floor, flanked by well- marked depressions. Although blind catheterization is difficult in small subjects, the procedure is less troublesome in larger bitches, in which a finger may be introduced to locate the tubercle and guide the instrument.
The bladder of the cat is more cranially placed than that of the dog and lies wholly within the abdomen at all times. As a result, the urethra is unusually long and some authors have been tempted to interpret the intraabdominal part as a curiously drawn-out bladder neck (Figure 15-7). The urethra of the queen is more or less uniformly wide (unlike its counterpart in the tom) and makes a more discrete entry into the vestibule than that of the bitch.
The male urethra of both species is considered with the reproductive organs.
The urachus, which connects the bladder with the allantoic sac of the fetus, normally closes at birth, but sometimes there is leakage at the umbilicus for a time. A more important anomaly is the persistence of part of the urachus as a diverticulum of the bladder, as this seems to predispose to recurrent bladder infections.
Congenital urinary incontinence in dogs and cats is most often caused by ectopic ureters, those which terminate at a site other than the normal one at the trigone of the bladder. Sometimes they take an unusual course through the bladder wall, and sometimes they bypass the organ to enter a more distal part of the urogenital tract.
Acquired urinary incontinence occurs most often after the spaying of bitches and is caused by urethral sphincter incompetence, for which a number of explanations, some likelier than others, have been suggested:
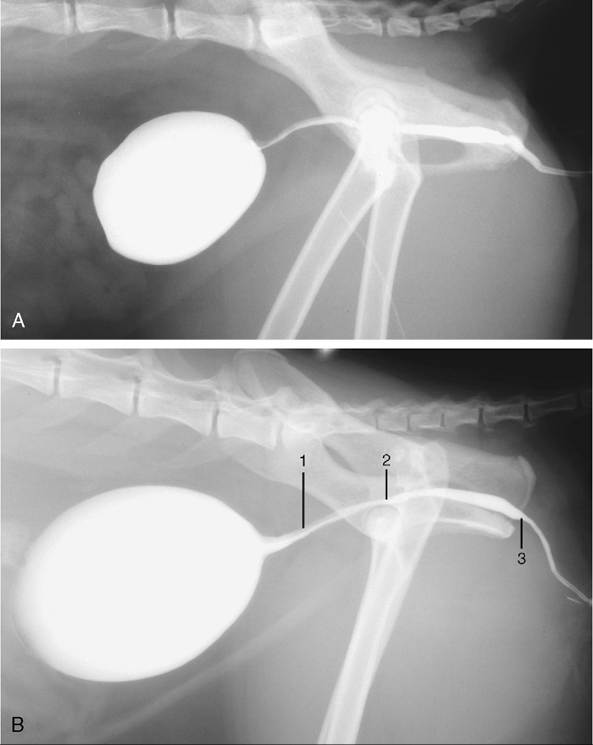
Figure 15-7 Radiographs of the feline bladder when moderately (A) and markedly (B) full. 1, Preprostatic urethra: the upper gray part is the urethral crest, the lower white part is the lumen filled with contrast medium; 2, slight dorsal dip marks the seminal colliculus; 3, isthmus, narrowing of lumen.
low urethral pressure, a short urethra, estrogen deficiency, or an intrapelvic position of the bladder. This type of incontinence is most often associated with relaxation or recumbency, particularly at night. Several surgical techniques have been developed to relocate the bladder neck to an intraabdominal position with the use of the prepubic tendon as an anchor.