» The Heart (see also pp. 219-220)
The canine heart is ovoid. It forms an angle of about 45 degrees with the sternum, with the base facing Craniodorsally and the blunt apex resting near the junction of the sternum and the diaphragm, a little to the left of midline (Fig.
13.17 and 13.18). However, the aforementioned angle and the space between the apex and the diaphragm vary more considerably than suggested. The angle is greater and the shape of the heart more conical in deep-chested breeds. Because of the biased position of the heart and the intervention of only a thinner layer of lung tissue between the heart and the left thoracic wall, the heart sounds are more pronounced on the left side (see Figs. 13.10, 13.17, 13.19, and 13.23).The heart contributes about 0.7% of the body weight on average, but its weight, both absolute and relative, varies considerably. In dogs trained for hunting or racing the heart is two or three times heavier than in fat and less athletic individuals of comparable size.
The left surface presents the auricles (atria) embracing the pulmonary trunk, and below the coronary groove the ventricles are divided by the paraconal interventricular groove (see Fig. 13.14). The right surface presents the atria and the subsinuosal interventricular groove. In reality, the left surface is rotated a little more toward the sternum and the right a little more toward the vertebrae. When one reads counterclockwise from the base, the periphery of the heart shadow in a left lateral radiograph shows the right auricle, the right ventricle, the left ventricle, and the left auricle (Fig. 13.17/1—4); in a ventrodorsal radiograph the sequence is right auricle, right ventricle, left ventricle, and pulmonary trunk (Fig. 13.17/2, 3, 5, and 6). The apex is formed only by the wall of the left ventricle.
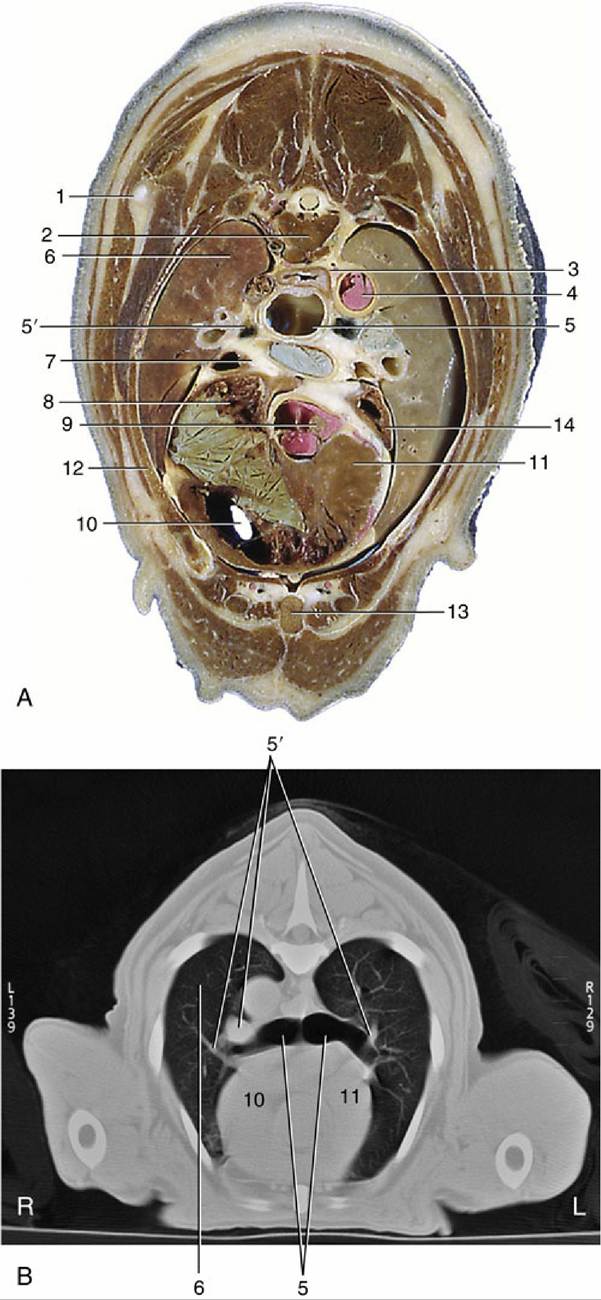
FIG.
13.13 (A) Transverse section of the canine trunk at the level of the sixth thoracic vertebra. (B) Corresponding computed tomography image at a slightly more caudal level. 1, Caudal angle of scapula; 2, sixth thoracic vertebra; 3, esophagus; 4, aorta; 5, tracheal bifurcation; 5', large blood vessels accompanying principal bronchi are likely right and left pulmonary arteries; 6, right lung; 7, tracheobronchial lymph nodes and pulmonary artery; 8, right atrium; 9, origin of aorta; 10, right ventricle;11, interventricular septum; 12, fifth rib; 13, sternum; 14, left auricle.
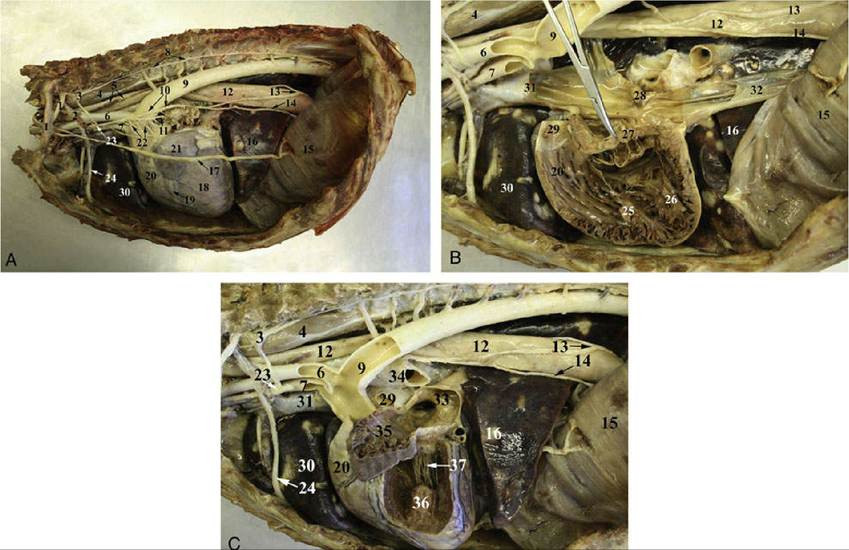
FIG. 13.14 Thoracal cavity of the dog, left side with left lung and mediastinal pleura removed (A) and left side of the heart opened (B) and left of the side of the heart removed (C). 1, T2 nerve to brachial plexus;
2, costocervical vein; 3, left cervicothoracic ganglion; 4, longus colli muscle; 5, thoracic duct; 6, left subclavian artery; 7, brachiocephalic trunk; 8, sympathetic trunk; 9, descending aorta (thoracic part); 10, vagus nerve; 11, left recurrent laryngeal nerve; 12, esophagus; 13, dorsal branch of vagus nerve; 14, ventral branch of vagus nerve; 15, diaphragm; 16, accessory lobe the right lung; 17, left phrenic nerve; 18, left ventricle of the heart; 19, paraconal interventricular artery, vein, and groove; 20, conus arteriosus of the right ventricle; 21, left auricle; 22, cardiac autonomic nerve; 23, middle cervical ganglion; 24, internal thoracic artery and vein; 25, musculus papillaris magnus; 26, musculi papillares parvi; 27, interventricular septum with the septal part of the tricuspidal valve; 28, intervenosus tubercle; 29, pulmonary trunk; 30, cranial lobe of the right lung; 31, cranial vena cava; 32, caudal vena cava; 33, pulmonary vein; 34, left primary bronchus; 35, left auricle with the pectinate muscles; 36, subauricular papillary muscle; 37,
chordae tendineae.
It is clearly important to know the relationships of the parts of the heart to external landmarks for auscultation and radiography.
The heart extends from the third rib to the sixth intercostal space, and the latter limit roughly coincides with the most cranial extent of the diaphragm (Fig. 13.17A). The projection of the base intersects the middle of the fourth rib; the most dorsal part of the heart reaches approximately to the line connecting the acromion with the ventral end of the last rib. The apex lies just to the left of the second last sternebra. In the standing dog the apex beat is palpable on both sides, low in the fifth or sixth intercostal space. The main contractions are said to be strongest in the lower third of the fourth or fifth space and to be a little more pronounced on the left.The ductus arteriosus or its replacement, the ligamentum arteriosum (p. 240), is located where the pulmonary trunk is intersected by the left vagus nerve, opposite the fourth rib (see Fig. 13.14). These details are relevant to the diagnosis and surgical treatment of persistent ductus arteriosus, the most common congenital anomaly of the canine cardiovascular system. Among other signs, a persistent ductus produces a characteristic "machine" murmur. The condition can be treated by ligation and section of the duct. It may be reached by a left lateral thoracotomy through the fourth intercostal space. The same approach provides access to the right ventricle, left auricle, pulmonary trunk, and descending aorta. (The fourth space on the right side may be used to gain access to the main part of the right ventricle, both auricles, the ascending aorta, and both the caval and the azygos veins.)
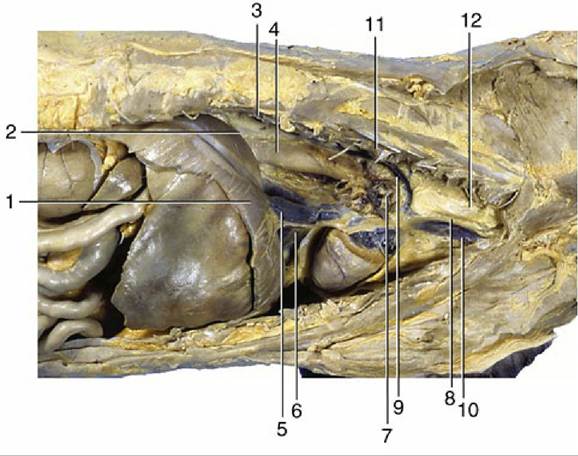
FIG. 13.15 Right lateral view of the canine thoracic cavity; the lung and much of the pericardium have been removed. 1, Diaphragm; 2, infracardiac bursa; 3, sympathetic trunk; 4, esophagus; 5, caudal vena cava; 6, plica venae cavae; 7, root of lung and phrenic nerve; 8, right vagus; 9, right azygous vein; 10, cranial vena cava; 11, longus colli; 12, trachea.
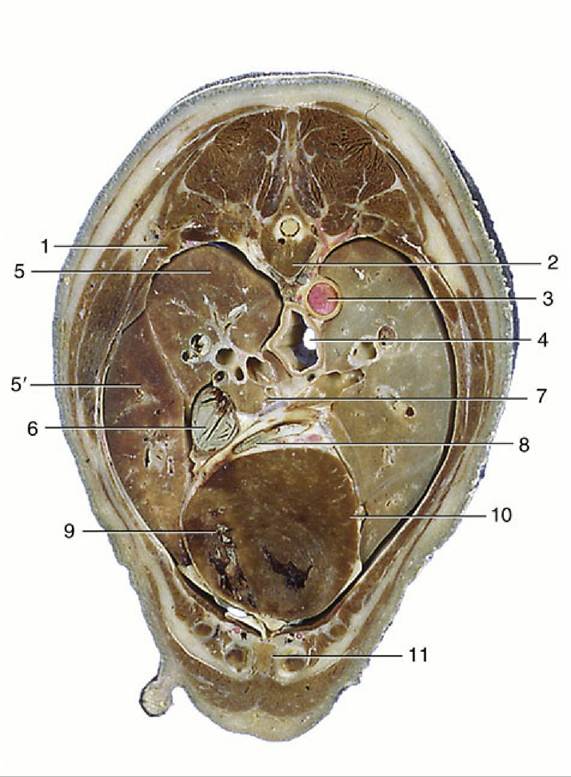
FIG.
13.16 Transverse section of the canine trunk at the level of the seventh thoracic vertebra. 1, Sixth rib; 2, seventh thoracic vertebra; 3, aorta; 4, esophagus; 5, cranial lobe; 5', middle lobe of right lung; 6, caudal vena cava; 7, pulmonary veins passing to left atrium; 8, great cardiac vein; 9, right ventricle; 10, left ventricle; 11, sternum.The heart is more easily auscultated than in the larger species because it is less covered by the forelimbs and a stethoscope can be introduced deeply into the axilla. The puncta maxima for optimal perception of the valve sounds (Fig. 13.4A-D) in the dog may be summarized as shown in Table 13.1. These findings correspond surprisingly closely with those determined at postmortem examinations of dogs diagnosed in life as having valvular lesions, despite the distorting influence of tissues on the conduction of sound.
There are no significant structural peculiarities of the canine heart, although it may be noted that the right atrioventricular valve possesses only two major cusps in many (perhaps most) dogs. No clinical significance attaches to the variation.
In North America many dogs are infested with large heartworms (Dirofilaria immitis), which occupy the pulmonary trunk and, in severe cases, the right ventricle, atrium, and caudal vena cava.
The heart of the cat extends from the third (or fourth) to the sixth (or seventh) rib. Little is covered by the forelimb in the standing animal because the triceps reaches no farther than the fourth rib. The long axis of the heart forms a more acute angle with the sternum, which results in a greater area of sternal contact than in most dogs. The contractions are strongest near the ventral ends of the fourth to sixth ribs on the left and the fifth rib on the right (Fig. 13.20). The corresponding puncta maxima are as follows: the left atrioventricular valve—in the fifth and sixth intercostal spaces, level with the shoulder joint; the pulmonary and aortic valves—low in the left second and third intercostal spaces; and the right atrioventricular valve—level with the shoulder joint in the fourth and fifth intercostal spaces. Puncture is difficult because the organ is so small; a needle inserted on either side of the right fifth costochondral junction should enter a ventricle.