THE LARGE INTESTINE
In its most elementary form the mammalian large intestine is a short tube, little wider than the small intestine from which it arises to pursue a direct course to the anus. The canine large intestine is somewhat more complicated, though still simple if compared with that of herbivores (Figure 3-45).
As in most species, it is clearly divided into cecum, colon, and rectum, while the colon is itself differentiated into ascending, transverse, and descending parts (Figure 3—45/3,4,5). The cecum is a blind-ending piece of gut that arises at the junction of the ileum and colon. The division of the colon follows from the rotation of the embryonic gut imposing a conformation on the adult organ that resembles a question mark (when viewed from below; Figure 14-15).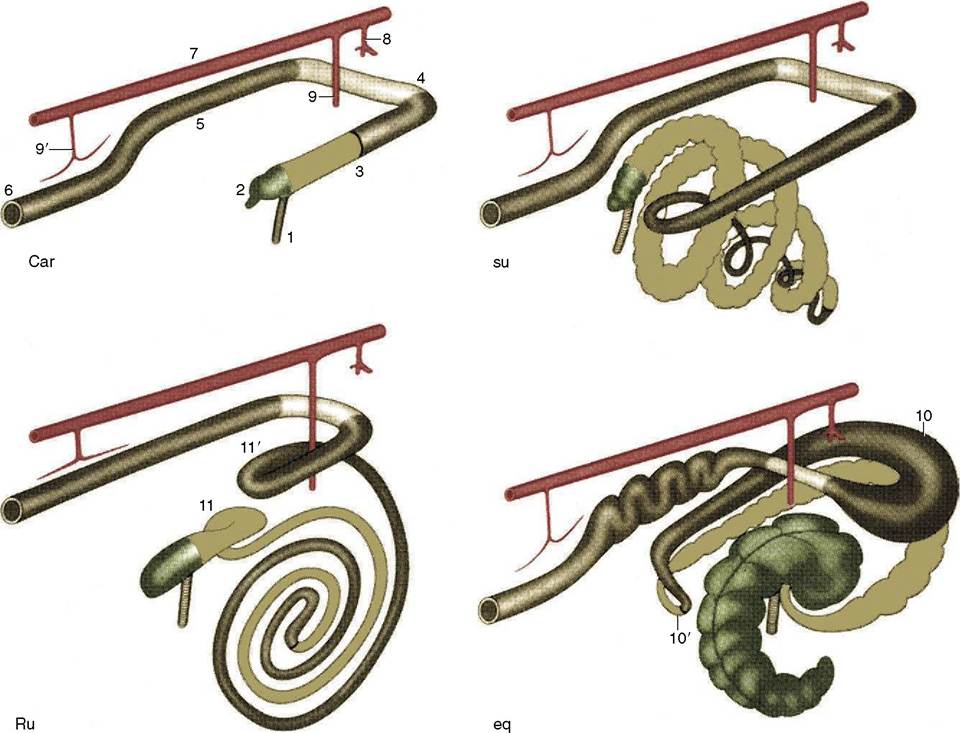
Figure 3-45 Schematic drawing of the large intestine of the domestic mammals: carnivores (Car), the pig (su), ruminants (Ru), and the horse (eq). Cranial is to the upper right. 1, Ileum; 2, cecum; 3, ascending colon; 4, transverse colon; 5, descending colon; 6, rectum and anus; 7, aorta; 8, celiac artery; 9, 9', cranial and caudal mesenteric arteries; 10, 10', dorsal diaphragmatic and pelvic flexures of ascending colon; 11, 11', proximal and distal loops of ascending colon.
The canine cecum is unusual in having no direct connection with the ileum; however, because it is conventional to regard the cecum as the first part of the large intestine, the description commences with it. The cecum of the dog is short and at first sight appears even shorter because it is drawn into a spiral and held against the ileum by folds of peritoneum. It is only slightly wider than the small intestine and tapers slightly toward its rounded blind extremity. The lumen communicates with the interior of the colon, immediately beyond the ileocolic junction, through an opening that is guarded by an inner, circular, muscular ring (the cecocolic sphincter) (Figure 3-46).
The smooth, externally featureless colon has a caliber that is uniformly and significantly, though not remarkably, greater than that of the small bowel. It is suspended throughout its length by a moderately long mesocolon, which allows it some mobility, and its position and relations vary within certain limits; the flexures that divide it into ascending, transverse, and descending parts are not precisely fixed. The short ascending part continues the axis of the ileum from a junction defined internally by an ileocolic opening of similar appearance and construction to that at the origin of the cecum. The transverse part runs across the abdomen from right to
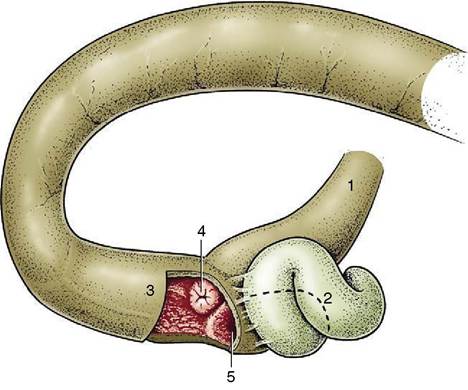
Figure 3-46 The ileocolic junction and its relation to the cecum in the dog. 1, Ileum; 2, cecum; 3, ascending colon; 4, ileal orifice surrounded by annular fold; 5, cecocolic orifice.
left, between the stomach cranially and the mass of small intestine and cranial mesenteric artery caudally. The descending part is the longest; it follows the left flank before edging medially to enter the pelvic cavity, where it is continued as the rectum without other visible demarcation than the passage across the abdominopel- vic boundary. The term rectum implies a straight course, but often this part of the bowel is deflected to one side by pressure from other viscera, most usually a distended bladder. The rectum is the most dorsal of the pelvic viscera and lies above the reproductive organs, bladder, and urethra. Its cranial part has the same relationship to the peritoneum as the colon, but this changes as the mesorectum shortens and the serosal covering is reflected laterally to continue into the parietal peritoneum of the pelvic cavity and ventrally to continue over the urogenital organs. The terminal part is wholly retroperitoneal and is directly attached to the vagina in the female, to the urethra in the male, and to the pelvic diaphragm in both sexes.
The mucosa of the large intestine is generally smooth because villi are lacking. No permanent mucosal folds are present, but there are numerous scattered lymph nodules, especially in the rectum, where they tend to be conspicuous; this is because the summits of the swellings are here depressed, leading to tiny pits. In many species, including the horse and pig among domestic animals, the outer muscle coat of the large intestine is mainly concentrated in a number of bands (teniae), which, on shortening, pucker the gut so that a linear series of sacculations (haustra) is produced (see Figure 21-11). Such bands are not present on the intestine of the dog and cat.
The anal canal joins the bowel to the exterior. It is a short passage that is derived from the proctodeum, the invagination of the surface ectoderm. The lumen is constricted at the rectoanal junction where the mucosa is thrown into longitudinal folds, normally pressed together to occlude the orifice (Figure 3-47). Anal continence, however, depends primarily on the presence of
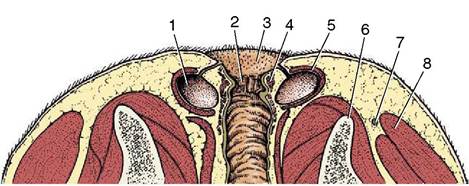
Figure 3-47 Dorsal (horizontal) section through the canine anal canal. 1, Anal sac; 2, columnar zone of the anal canal; 3, cutaneous zone; 4, internal anal sphincter; 5, external anal sphincter; 6, ischium; 7, sacrotuberous ligament; 8, gluteus superficialis.
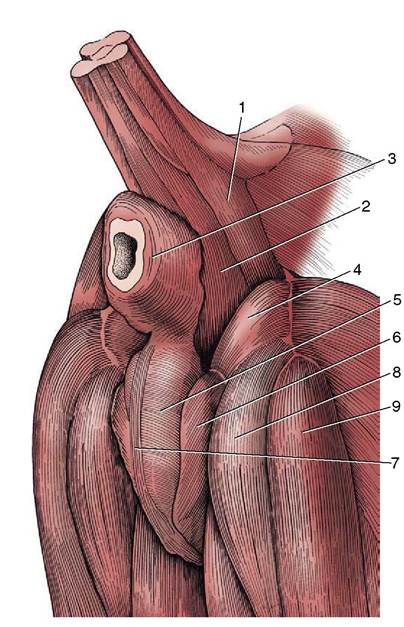
Figure 3-48 The muscles of the perineal region of the male dog. 1, Coccygeus; 2, levator ani; 3, external anal sphincter; 4, internal obturator; 5, bulbospongiosus; 6, ischiocavernosus; 7, retractor penis; 8, semimembranosus; 9, semitendinosus.
two sphincters; the internal anal sphincter is merely a thickening of the circular smooth muscle of the gut, but the external sphincter is striated, of somatic origin, and under voluntary control (Figure 3-48).
Many glands are always present in the anal region, both in the mucosa and in the surrounding skin.
Most are small, but the dog and cat also possess two so-called anal sacs (sinus paranales). Each is roughly the size of a hazelnut (in the dog) and is located ventrolateral to the anus between the internal and external sphincters (see Figures 3-47 and 15-4). The fundus of the sac secretes an evil-smelling fluid that drains through a single duct to an opening near the anocutaneous junction. The sac is compressed at defecation, expelling the secretion, which probably serves as a territorial marker. Such sacs are found in most carnivores and are most notorious in the skunk.The blood supply to the intestinal tract is mainly provided by the cranial and caudal mesenteric arteries; however, the initial part of the duodenum is supplied through the hepatic branch of the celiac artery and the caudal part of the rectum by rectal branches of the internal pudendal artery. The cranial mesenteric artery supplies the bulk of the small intestine, the ileocecocolic junctional region, and the midpart of the colon through its three primary divisions; the details of branching vary among species and also, though to a lesser extent, among individuals. The smaller caudal mesenteric artery has a distribution restricted to the descending colon and cranial part of the rectum. The arrangement in the dog is illustrated (Figures 3-42 and 3-49); although its relevance in surgery suggests that the pattern of arterial branching should be known, the richness of the anastomoses is of even greater importance. These ensure that the intestine can normally survive the complete obstruction of a major supplying vessel. The chain of anastomoses continues beyond the territories of the mesenteric arteries to connect with those of the celiac and internal pudendal arteries.
The veins are broadly comparable and join to form the cranial and caudal mesenteric veins, two of the main radicles (the splenic vein is the third) of the portal vein (Figure 3-50). Certain tributary veins connect with systemic veins at the extremities of their territories, which are the thoracic esophagus and anal canal, parts that normally drain by systemic routes.
Congestion within the portal circulation (p. 137) may lead to enlargement of submucosal veins in both these (and other) parts but is much more important in human than in veterinary medicine. The gut wall contains a considerable proportion of the lymphocyte population and represents an important component of the body’s defense mechanism, one capable of barring entry to a variety of antigens.The lymphatic drainage of the small intestine, in particular, is copious because some of the products of digestion are absorbed by this route. When these products include fat, the lymph is milky and the intestinal lymphatic vessels (“lacteals”) are unusually conspicuous. The flow is directed toward certain nodes through which the lymph percolates before joining the cisterna chyli, the dilated origin of the thoracic duct, the most important lymphatic vessel (p. 260). In the dog these nodes are large but few and are centralized toward the root of the mesentery (see Figure 3-40); in other species they may be more numerous and more widely scattered and may include many that are peripheral, close to the gut itself.
The intestine receives both sympathetic and parasympathetic nerves. The sympathetic pathways lead through the celiac, cranial mesenteric, and caudal mesenteric ganglia, and the postganglionic fibers enmesh the relevant arteries (see Figure 8-76). The parasympathetic pathways involve both vagal and pelvic nerves. The former supply the intestine to the junction of the transverse and descending parts of the colon; the latter supply the descending colon and rectum. The parasympathetic nerves augment peristalsis, but the effects of
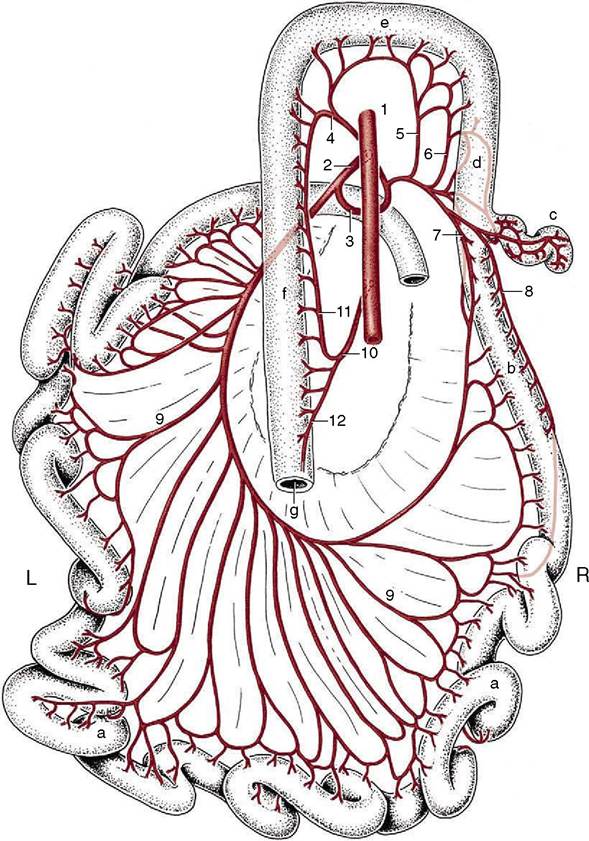
Figure 3-49 Distribution of the cranial and caudal mesenteric arteries to the intestines of the dog (dorsal view). a, Jejunum; b, ileum; c, cecum; d, ascending colon; e, transverse colon; f descending colon; g, rectum. 1, Aorta; 2, cranial mesenteric artery; 3, ileocolic artery; 4, middle colic artery; 5, right colic artery; 6, colic branch of ileocolic artery; 7, mesenteric ileal branch; 8, antimesenteric ileal branch; 9, jejunal arteries; 10, caudal mesenteric artery; 11, left colic artery; 12, cranial rectal artery.
intestinal denervation are far less striking than those of gastric denervation.
Under stress, vasoconstriction may close the capillary bed of the intestinal wall, leading to abnormal permeability that allows large molecules to overcome the gut barrier; septic shock is then an eventual possibility.