THE LARGE INTESTINE
In addition to its enormous capacity, the large intestine is also characterized by having a sacculated form. The sacculations or haustra result from the shortening of the teniae, bands formed by the concentration of the external longitudinal muscle and elastic fibers at certain (from one to four) positions on the circumference.
Semilunar folds project internally where grooves divide adjacent haustra externally (see Figure 21-11). The haustral segmentation is not constant but is constantly modified in life by gradual “haustral flow” and by intermittent disappearance of the contractions followed by their reformation in a different pattern.The arrangement of the large intestine of the horse predisposes to various forms of obstruction and displacement, conditions collectively known as colic (although this term is widely used to include any painful abdominal disorder).
The Cecum
The cecum incorporates an initial portion of the ascending colon as is revealed by its extension distally beyond the entrance of the ileum. It follows that the so-called cecocolic orifice is actually a constriction of the ascending colon set some distance distal to its true origin. However, the conventional terminology pays no regard to such considerations and is based entirely on the form of the adult organ (Figure 21-12).
The cecum consists of an expanded dorsal base, a curved tapering body, and a blind ventral apex; these parts merge smoothly, and the organ is often likened to a comma (Figure 21-13). In large horses it may have a capacity in excess of 30 L and may measure a meter or more between extremities. The base lies in the right
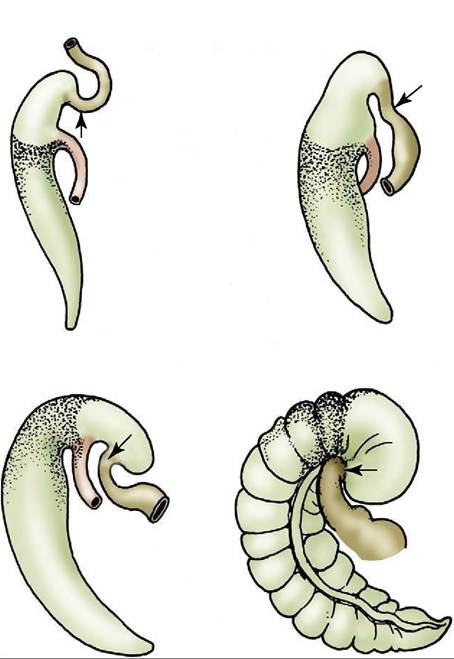
Figure 21-12 Development of the equine cecum, schematic. The stippled part of the cecum is homologous with the cecum of other species.
The nonstippled part is the annexed first part of the colon. The cecocolic orifice is a constriction of the ascending colon (arrows).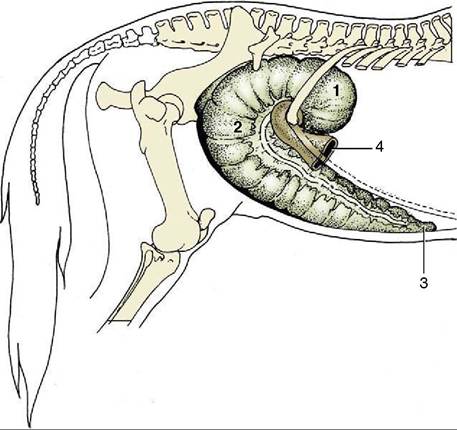
Figure 21-13 The cecum in situ. 1, Base of cecum; 2, body of cecum; 3, apex of cecum; 4, right ventral colon.
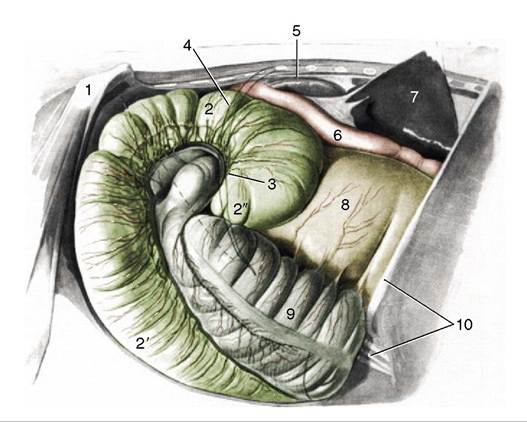
Figure 21-14 Cecum and related organs lying against the right abdominal wall and flank. The broken line indicates the position of the cranial branch of the deep circumflex iliac artery crossing the flank. 1, Coxal tuber; 2,2', base and body of cecum; 2'', overhanging part of cecal base; 3, position of cecocolic orifice; 4, position of last rib; 5, right kidney; 6, descending duodenum; 7, right lobe of liver, elevated; 8, right dorsal colon; 9, right ventral colon; 10, tenth rib and costal arch.
dorsal part of the abdomen, partly against the flank and partly under cover of the ribs. It has an extensive contact with the abdominal roof and sublumbar organs from the fifteenth rib (or thereabouts) to the coxal tuber, but the direct dorsal adhesion is confined to the region of the pancreas and right kidney. This retroperitoneal attachment extends caudally to the level of the second lumbar vertebra. The base also fuses with the root of the mesentery medially and with the right dorsal colon cranially. The cranial part of the base forms an overhanging enlargement that at first sight appears to be blind (Figure 21-14); closer inspection reveals the origin of the colon from the middle of the caudal wall of this overhang. The caudal part of the base merges imperceptibly with the body of the cecum. Microbial fermentation within the cecum produces gas that is normally discharged at intervals into the right ventral colon. Occasionally, gas is produced excessively, causing the overhanging part of the base to press on the origin of the right ventral colon, interfering with the normal mechanism.
The resulting tympany of the base can only be relieved by needle decompression through the para- lumbar fossa.The body runs ventrally before turning cranially (Figure 21-13/2). At first it lies against the right flank, following the caudal border of the right ventral colon, but as it sinks within the abdomen, it is displaced medi-
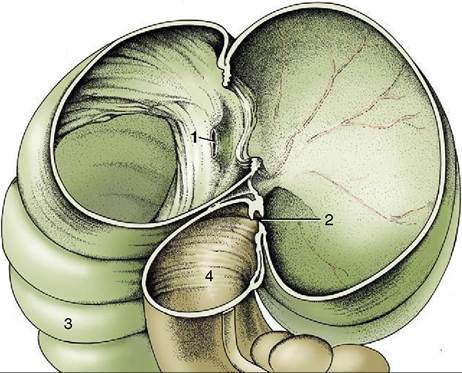
Figure 21-15 The interior of the base of the cecum, right lateral view. 1, Termination of ileum at ileal papilla; 2, cecocolic orifice; 3, body of cecum; 4, right ventral colon.
ally; when it reaches the abdominal floor, it lies between the ventral parts of the ascending colon. It terminates in the apex, close to the xiphoid cartilage. There are four teniae over most of the organ, but the number diminishes toward the apex. Retroflexion of the apical part of the cecum is occasionally encountered in apparently healthy subjects.
The interior is marked by numerous folds corresponding to the external divisions of the haustra. These folds are impermanent, but a larger and more persistent fold at the level of the ileal papilla partially separates the cranial expansion from the remainder of the base (Figure 21-15). The ileal papilla is variable in form. In most postmortem specimens it is a low conical projection whose summit carries a slitlike opening bounded by lax folds of mucosa (Figure 21-15/7). In life, it is usually much more salient and more cylindrical and has a rounded orifice circumscribed by a firm and thickened rim. The erection of the papilla is caused by the tonus of the muscle and engorgement of a mucosal venous plexus.
Although the exit from the cecum near the cecocolic orifice (Figure 21-15/2) lies at some distance from the ileal papilla, the curvature of the cecal base brings it more or less into the same transverse plane. In the dead specimen it is a transverse slit that scarcely admits a few fingers, but in life it generally allows the passage of a hand.
The Colon
The colon consists of the usual ascending, transverse, and descending parts (see Figure 3-45). The first two together constitute the “large colon” of common usage, and the third constitutes the “small colon” (Figure 21-11/75). The ascending colon is arranged in four parallel limbs separated by three flexures, each separately named. The sequence runs as follows: right ventral colon (Figure 21-11/7), ventral diaphragmatic flexure, left ventral colon, pelvic flexure, left dorsal colon, dorsal diaphragmatic flexure, and right dorsal colon (Figure 21-11/75). The right dorsal colon leads to the short transverse colon (Figure 21-11∕7√); this is followed in its turn by the descending colon, which is long and thrown into coils (Figure 21-11/75).
The cecocolic transitional region forms a sigmoid flexure: the convexity of the first bend (provided by the overhanging part of the cecal base) is directed ventrally, and that of the second bend (provided by the first part of the colon) is directed dorsally (Figure 21-14 and Figure 21-16). This conformation appears to be caused by the looser attachment of the medial and lateral teniae at this level; they run as chords across the arcs into which the bowel is drawn. The right ventral colon is narrow when it emerges from this siphon-like arrangement but soon expands to continue, first ventrally, then cranially on the abdominal floor, as a wide (ca. 20-cm) tube of uniform caliber (see Figure 21-7). It is deflected across the midline on reaching the diaphragm (ventral diaphragmatic flexure) and then becomes known as the left ventral colon (Figure 21-17). The left ventral colon runs toward the pelvis, still on the abdominal floor (see Figure 21-6) until a sharp flexure through 180° marks its junction with the following left dorsal part. The pelvic flexure is also distinguished by a reduction in caliber (see Figure 21-11) and by the disappearance of three of the four bands found on the ventral parts, of
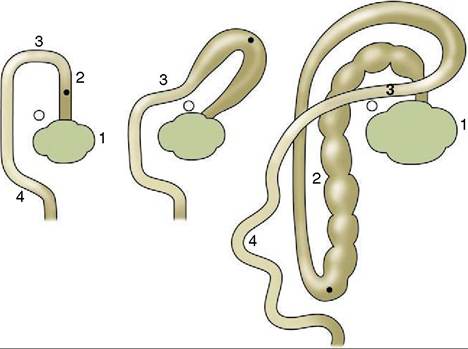
Figure 21-16 The development of the ascending colon, dorsal view.
The dot indicates the position of the pelvic flexure, the circle that of the cranial mesenteric artery. 1, Cecum; 2, ascending colon; 3, transverse colon; 4, descending colon.which the consequence is the loss of the haustrations. Although there is no evidence of a conventional sphincter, the pelvic flexure marks the boundary between two distinct functional units of the colon. The decrease in the fluidity of the ingesta, the sudden alteration in course, and the reduction in caliber explain why impaction is common at this level. The location of the flexure varies with the fullness of the rectum, bladder, and uterus, but because it is usually just within or in front of the pelvic cavity, it is easily found on rectal examination especially if impacted.
The left dorsal colon is narrow and smooth-walled where it emerges from the pelvic flexure, but it gradually widens; the teniae increase from one to three, and the sacculations return. It runs cranially above the left ventral colon, below the coils of small intestine and descending colon, to reach the liver, where it continues as the right dorsal colon at the dorsal diaphragmatic flexure. Toward its termination it is related to the spleen and the stomach (Figure 21-6/7). The right dorsal colon is both the shortest and, at its termination, by far the widest part (ca. 30 cm) of the ascending colon (Figure 21-18/7). It ascends below the liver to meet the cranial part of the cecal base by which it is deflected medially to become the transverse colon (Figure 21-18/5). The right dorsal colon is also the best-fixed part and is
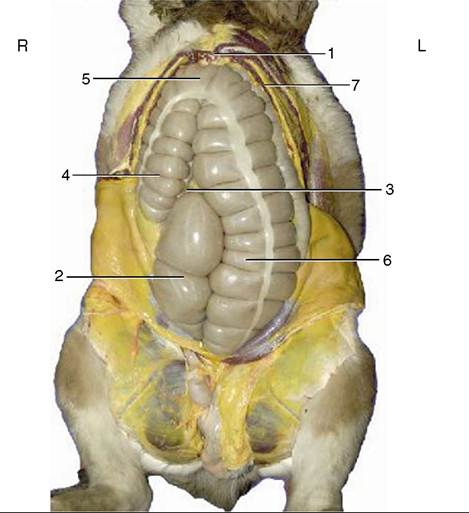
Figure 21-17 Visceral projection on the ventral abdominal wall. The position of the apex of the cecum is variable. 1, Xiphoid cartilage; 2, body of cecum; 3, apex of cecum; 4, right ventral colon; 5, ventral diaphragmatic flexure; 6, left ventral colon; 7, dorsal diaphragmatic flexure.
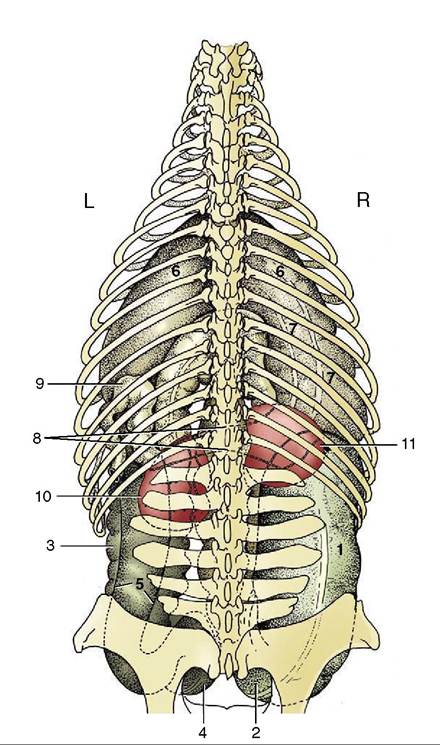
Figure 21-18 Position of the large intestine and the kidneys, dorsal view.
1, Base of cecum; 2, body of cecum; 3, left ventral colon; 4, pelvic flexure; 5, left dorsal colon; 6, dorsal diaphragmatic flexure; 7, right dorsal colon; 8, transverse colon; 9, proximal part of descending colon, cut; 10, left kidney; 11, right kidney.adherent to the abdominal roof, the cecal base, and the root of the mesentery. It carries three bands.
The transverse colon is very short and is situated according to the common mammalian pattern, passing from right to left in front of the root of the mesentery. It carries two bands and rapidly funnels to the much smaller caliber of the descending colon (Figure 21-18/9) by which it is succeeded in the region of the left kidney. The transverse colon also has a direct retroperitoneal attachment to the abdominal roof.
Except at its origin and termination the ascending colon is free within the abdomen, although its great bulk ensures that it does not change much in position. The folding it undergoes in development transforms the original mesentery into a short peritoneal sheet (ascending mesocolon) passing between adjacent portions of the dorsal and ventral limbs (Figure 21-11/75'). Through continuity with the cecum and transverse colon it is anchored by the retroperitoneal attachments of these parts. The loose attachment between the left limbs allows the dorsal part to slip some way to the side (generally the right side) of the ventral part as a common and probably temporary variant of the usual topography. When the rotation of these parts about their common axis is pronounced, there arises the condition known as twist (torsio), which is one of the most severe abdominal catastrophes to which the horse is subject. A torsio coli initially narrows the lumen, but more important is the interruption of the blood flow in the capillaries of the bowel wall and in the vessels that follow the bowel. Another malposition of the ascending colon that has been increasingly recognized in recent years involves the lodgment of the left limbs above the spleen. Although the cause of this painful condition is not known with certainty, it is postulated that the accumulation of gas raises the left limbs against the abdominal wall until they pass over the base of the spleen to be trapped on the shelf formed by the phrenicosplenic and renosplenic ligaments (left dorsal displacement). Spontaneous restoration of normal topography is possible, but quicker restoration may be achieved by rolling and maneuvering the recumbent (anesthetized) animal. If the rolling procedure is failing, surgical intervention (decompression) is required.
The descending colon (Figure 21-11/75), much narrower than the other parts, is several meters long and alone hangs within a conventional mesentery. These features account for its alternative names, small colon and floating colon. It lies mainly within the dorsal, caudal, and left part of the abdomen, largely dorsal to the small intestine, and ends in the rectum (Figure 21-6/5). The distinction between the descending colon and rectum is based entirely on the pelvic location of the latter, and no immediate change in structure or appearance occurs. The descending colon is drawn by two prominent bands into a linear series of sacculations occupied by the familiar dry fecal balls. The rectum is considered with the pelvic organs.