VASCULARIZATION, LYMPH DRAINAGE, AND INNERVATION OF THE GASTROINTESTINAL TRACT
The vascularization of the equine abdominal viscera was especially in the past of clinical importance because of the occurrence of vascular pathology caused by migrant nematode larvae.
The fact that these lesions are not often fatal is due to the extensive system of anastomoses between the arteries supplying successive parts of the gastrointestinal tract. The pathology is often most serious in the cranial mesenteric artery and its major branches; these may be so greatly enlarged by aneurysm formation and by connective tissue reaction that the normal structure and topography are grossly disturbed. Paradoxically, obstruction of one of the large branches may have much less serious consequences than closure of a smaller one: the anastomoses of the major arteries are large and constant, but those of the minor arteries are small and often dangerously deficient. The caudal mesenteric artery, specifically concerned with the descending colon, may also be affected.The branching and distribution of the two mesenteric arteries are shown in Figure 21-19. The celiac artery has essentially the same distribution to stomach, liver, and spleen as in other species. The venous drainage parallels the arterial supply, in that the portal vein
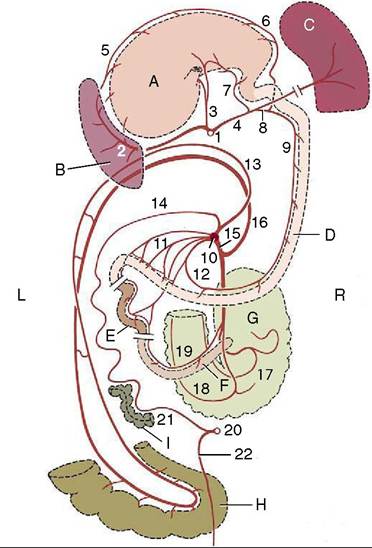
Figure 21-19 The major arteries of the gastrointestinal tract, schematic dorsal view. The structures have been stretched craniocaudally for clarity. A, Stomach; B, spleen; C, liver; D, duodenum; E, jejunum; F, ileum; G, cecum; H, pelvic flexure; I, descending colon. 1, Celiac a.; 2, splenic a.; 3, left gastric a.; 4, hepatic a.; 5, left gastroepiploic a.; 6, right gastroepiploic a.; 7, right gastric a.; 8, gastroduodenal a.; 9, cranial pancreaticoduodenal a.; 10, cranial mesenteric a.; 11, jejunal aa.; 12, caudal pancreaticoduodenal a.; 13, right colic a.; 14, middle colic a; 15, ileocolic a.; 16, colic branch of ileocolic a.; 17, lateral cecal a.; 18, medial cecal a.; 19, mesenteric ileal a.; 20, caudal mesenteric a.; 21, left colic a.; 22, cranial rectal a.
is ultimately formed by the union of the caudal mesenteric, cranial mesenteric, and splenic tributaries.
Lymph from the regional nodes of the stomach, spleen, liver, pancreas, and diaphragm drains to a lymph center about the celiac artery and thence to the cisterna chyli via a celiac trunk.
The very numerous nodes that receive lymph from the intestines (with the exception of the caudal part of the descending colon) are scattered at the root of the mesentery and along the arteries of the cecum and colon. Lymph is collected and conveyed to the cisterna chyli by an intestinal trunk. The nodes scattered along the remainder of the descending colon send lymph to a center at the root of the colic mesentery and then to the lumbar trunk; this route is also followed by most of the lymph draining the rectum and anus.
The abdominal viscera are supplied by nerves that pass through plexuses associated with the mesenteric ganglia (see Figure 21-24/18,20). The nervous structures about the celiac and cranial mesenteric arteries may be involved in the reaction provoked by the nematode larvae and are difficult to display satisfactorily except in juvenile animals. It is often asserted, although it remains unproven, that the “colic” pain and functional disturbance associated with helminth infestations are caused by secondary involvement of the nerves rather than by the primary vascular lesions.