THE SMALL INTESTINE
The small intestine measures about 25 m in the carcass, although it is probably much less in life. The duodenum is relatively short, and because it is closely tethered, it is more or less constant in position.
It commences ventral to the liver where the initial (cranial) part forms a sigmoid flexure of which the first curve is convex dorsally, the second convex ventrally. The second (descending) part then runs caudally, still below the liver, until it reaches the lateral margin of the right kidney, which it follows to the caudal pole; it then bends medially behind the root of the mesentery (Figure 21-10/d and Figure 21-11/2,3). The descending duodenum is also related to the right lobe of the pancreas and crosses above the last part of the right dorsal colon and the base of the cecum to which it is attached (see Figure 21-14). This relationship permits the formation of a temporary duodenocecal anastomosis in the treatment of gastroduodenojejunitis, obviating the reflux of fluid and consequent overloading of the stomach that characterizes this condition. The third (ascending) part runs forward against, and adherent to, the left face of the mesentery; it bends ventrally below the left kidney to continue as the jejunum. The caliber of the duodenum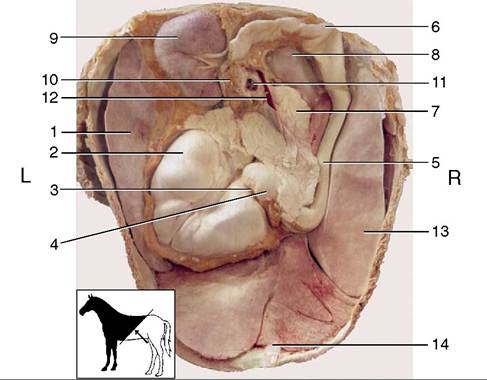
Figure 21-10 The organs in the Craniodorsal part of the abdominal cavity of a young horse, Caudoventral view (see inset). 1, Spleen; 2, stomach; 3, pylorus; 4, 5, cranial and descending parts of duodenum; 6, caudal flexure of duodenum; 7, pancreas; 8, right kidney; 9, left kidney; 10, left adrenal gland; 11, cranial mesenteric artery and vein; 12, portal vein; 13, liver; 14, falciform ligament.
is uniform except at its commencement, where the first bend of the sigmoid flexure is somewhat widened.
The bile and pancreatic ducts open here. The bile and major pancreatic ducts discharge through a single papilla within an enclosure (ampulla hepatopancreatica) bounded by a circular mucosal rampart. This is situated on the convex margin of the flexure, while the accessory pancreatic duct opens on a small papilla on the facing margin (see Figure 21-21/7,8).The position and restricted mobility of the duodenum make its access difficult through the usual surgical exposures; fortunately, indications for duodenal surgery are largely restricted to the condition recently mentioned.
The remainder of the small intestine lies within the free margin of the great mesentery, which is sufficiently long to allow the coils considerable latitude in position. Most are piled into the left dorsal part of the abdomen where they mingle with those of the descending colon; however, some insinuate themselves between the large intestine and the flanks, while others may reach the abdominal floor between the body of the cecum and the
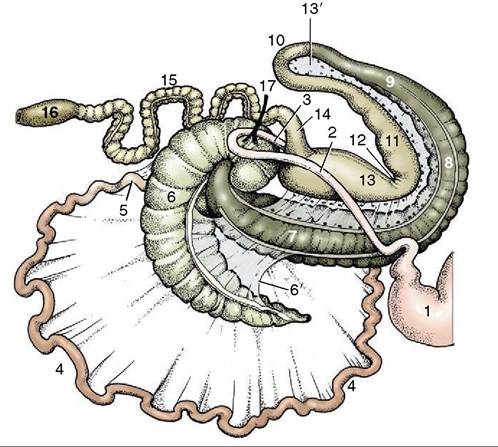
Figure 21-11 The intestinal tract seen from the right, schematic. The caudal flexure of the duodenum and the cranial mesenteric artery (17) have been displaced to the right of the animal to lie over the base of the cecum. 1, Stomach; 2, 3, descending and ascending duodenum; 4, jejunum; 5, ileum; 6, cecum; 6', cecocolic fold; 7, right ventral colon; 8, ventral diaphragmatic flexure; 9, left ventral colon; 10, pelvic flexure; 11, left dorsal colon; 12, dorsal diaphragmatic flexure; 13, right dorsal colon; 13', ascending mesocolon; 14, transverse colon; 15, descending (small) colon; 16, rectum; 17, cranial mesenteric artery.
ventral parts of the ascending colon. The ileum (according to the convention we employ [p. 129]) is very short, and in most circumstances it is distinguished from the remainder of the small intestine by its much thicker wall and firmer consistency. It approaches the left side of the cecal base from below and ends by protruding into the cecal interior, raising a papilla on which it opens.
The mobility of the small intestine may be blamed for the incarceration of a part within one of several openings such as the epiploic foramen, vaginal ring, or even a rent in the mesentery. Intussusception is also relatively common, especially in the young horse. A form peculiar to the horse involves the passage of the terminal part of the small intestine into the interior of the cecal base. Necrosis of the intruded part follows quickly unless surgical correction is undertaken.