THE MOUTH
The small size of the entrance makes it impossible to open the mouth wide; this limitation, coupled with the great depth of the cavity, severely hampers clinical inspection.
The vestibule communicates with the mouth cavity proper only between the incisor and cheek teeth (where the diastema may be interrupted by the canine) and by small gaps behind the last molars.
The hard palate is therefore largely bounded by the alveolar processes and teeth. It is almost uniformly broad and is marked by two more or less symmetrical series of ridges (Figure 18-11/5). The incisive papilla is found directly behind the central incisors; grooves that flank the elevation end blindly and do not communicate with the nasal cavity and vomeronasal organs (see Figure 18-12). The mucosa of the hard palate is thick, particularly in its most rostral part, and incorporates a very generous venous plexus, which may become engorged (lampas) at the time of tooth replacement when it may project above the occlusal surfaces of the neighboring teeth. The appearance is striking and laypeople are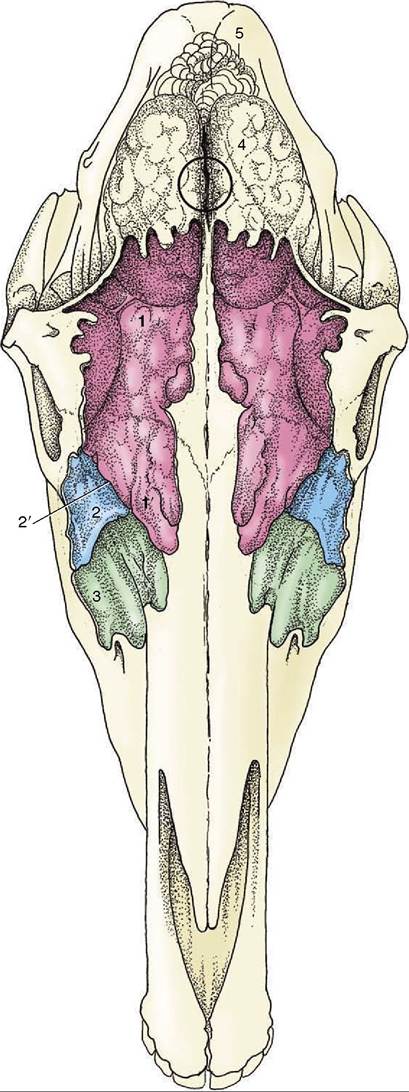
Figure 18-14 Projection of the brain and frontal and maxillary sinuses on the dorsal surface of the skull. The sinuses are filled with casting material. The frontal sinus extends caudally over the rostral part of the brain and rostrally beyond the level of the orbit. The circle indicates the center of the brain and the location where a horse may be shot. 1, 1', Conchofrontal sinus; 1, frontal part; 1', dorsal conchal part; 2, caudal maxillary sinus; 2’, position of frontomaxillary opening; 3, rostral maxillary sinus; 4, cerebrum; 5, cerebellum.
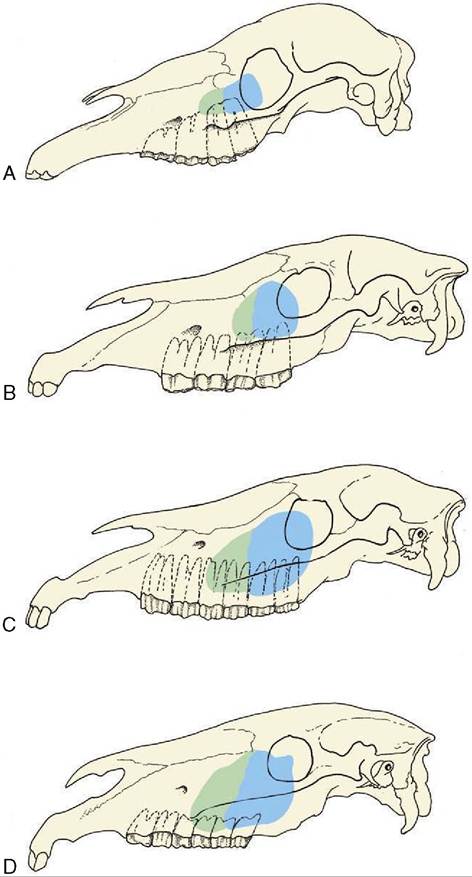
Figure 18-15 Projection of the maxillary sinuses at various ages.
In older horses the cheek teeth are more rostrally placed. A, 1 month. B, 1 year. C, 4 to 6 years. D, Older than 12 years.sometimes alarmed by this purely physiological phenomenon.
The soft palate continues the hard palate beyond the level of the second molar tooth. It is remarkably long and hangs down before the epiglottis; its free margin is closely applied to the tongue. The palatopharyngeal arches extend caudally from the palate, completing a sphincter about the structures that bound the entrance to the larynx, which thus projects some way into the nasopharynx. The application of the palate to the tongue is so firm that an air-tight seal is created that closes the oropharynx, which then provides a barrier between the mouth and the pharynx. This ensures that breathing is through the nose, precluding use of the oral route and incidentally resulting in ingesta passing into the nasal passages on the rare occasions when horses vomit. These relationships of the palate are normally maintained except during deglutition. The obstructions of the upper respiratory tract commonly recognized in horses worked at a fast pace are often due to anomalous position and relations of the soft palate.
Understanding of these matters has been greatly improved by video endoscopy of the nasopharynx and larynx of affected horses undertaken while they were strenuously exercised on a treadmill. Two abnormal conditions of the soft palate are now recognized; both apparently occur after admission of air into the oropharynx breaks the seal that normally maintains the parts in close apposition. In the less severe form, there is abnormal movement of the caudal part of the palate, aptly described as “billowing.” In the more severe form, of which billowing is probably a precursor, the soft palate is displaced dorsally, losing contact with the ventral side of the epiglottis and narrowing the nasopharyngeal airway. At endoscopy the epiglottis is no longer visible. Both forms may be accompanied abnormal respiration sounds.
The impairment of respiratory efficiency inevitably leads to diminished physical performance. It is uncertain how the seal comes to be broken, but among the factors blamed are the following: the extreme negative pressure developed in the rostral nasopharynx at one stage of the respiratory cycle; dysfunction of the palate musculature weakening the contact between tongue and palate; overactivity of those ventral cervical muscles that attach to the larynx and hyoid drawing the larynx caudally, freeing the palate from entrapment by the epiglottis; and abnormal activity of the hyoepiglottic muscle, tilting the epiglottis caudally with the same effect. There is some evidence that obstructions are commoner at the palatopharyngeal level in younger animals and at the laryngeal level in older animals and that frequently both occur together.The mucosa on the oral surface of the soft palate is marked by numerous pits where the palatine glands open. It also exhibits a rostral median tonsillar swelling (see Figure 3-25).
The tongue is long, conforming to the shape of the cavity, and is spatulate at its apex, which is incompletely restrained by a narrow frenulum. Its upper surface is thickly strewn with delicate filiform papillae that confer a velvetlike texture; the larger papillae with gustatory function are less widely spread (Figure 18-16/9,10,11). A scattering of lymphoid tissue over the root constitutes a diffuse lingual tonsil. Each of two low mucosal folds beneath the apex of the tongue carries a fleshy sublingual caruncle where the mandibular duct opens.
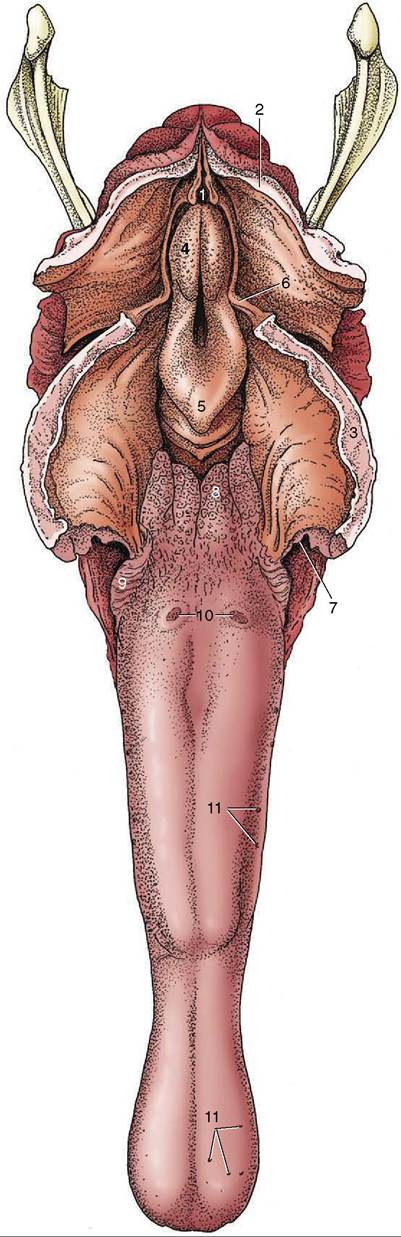
Figure 18-16 The tongue and pharynx; the latter has been opened dorsally to expose the entrance to the larynx. 1, Entrance into esophagus; 2, dorsal wall of nasopharynx (split in median plane); 3, soft palate (split in median plane); 4, corniculate process of arytenoid cartilage; 5, epiglottis; 6, free border of soft palate, continued caudally by palatopharyngeal arch; 7, palatoglossal arch; 8, lingual tonsil; 9, foliate papillae; 10, vallate papillae; 11, examples of fungiform papillae.