THE PHARYNX

2
1
Figure 18-24 Characteristic appearance of lower incisors of Standardbred horses of accurately known ages.
A, 1.5 years. B, 2.5 years. C, 3 years. D, 4 years. E, 5 years. F, 6 years. G, 7 years. H, 8 years. I, 9 years. 1, Deciduous teeth; 2, newly erupted I1; 3, dental cup; 4, dental star; 5, enamel spot (proximal end of infundibulum).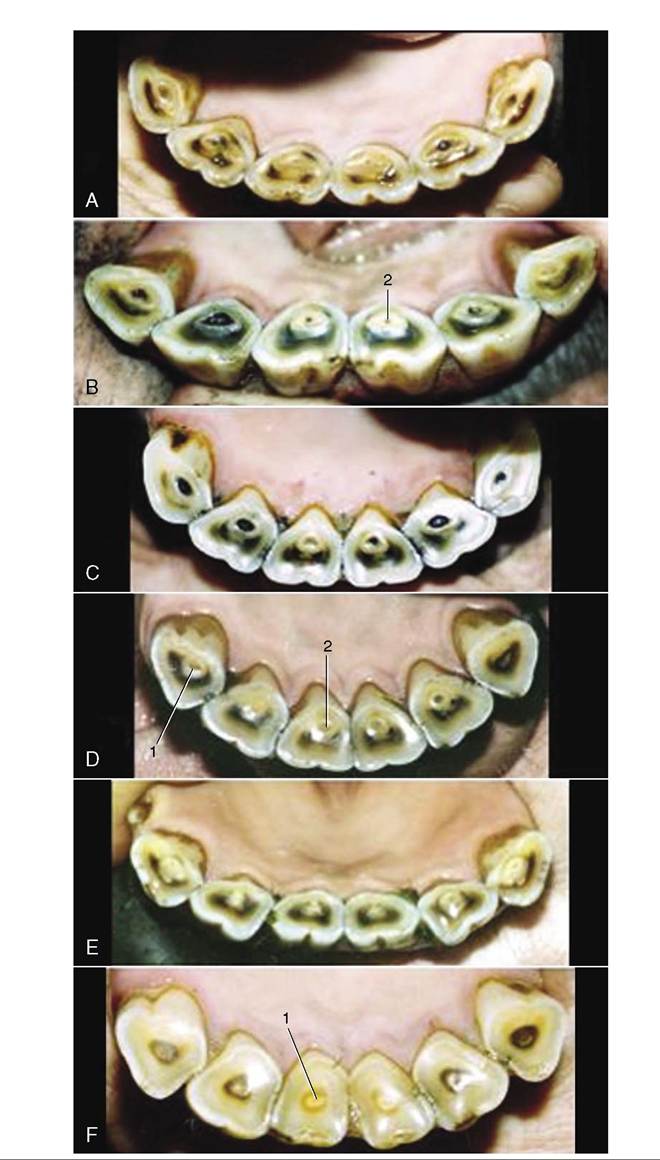
Figure 18-25 Characteristic appearance of lower incisors of Standardbred horses of accurately known ages. A, 11 years. B, 12 years. C, 14 years. D, 16 years. E, 17 years. F, 20 years. Note particularity of the changes in form of the occlusal surface: from round to triangular. 1, Dental star; 2, enamel spot.
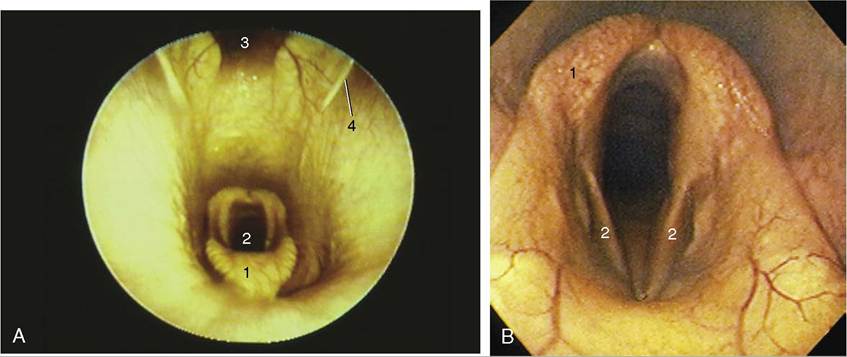
Figure 18-26 A, Endoscopic view of equine nasopharynx. 1, Epiglottis; 2, laryngeal entrance; 3, pharyngeal recess; 4, entrance to auditory tube. B, Endoscopic view of larynx. 1, Arytenoid cartilage; 2, left and right vocal folds.
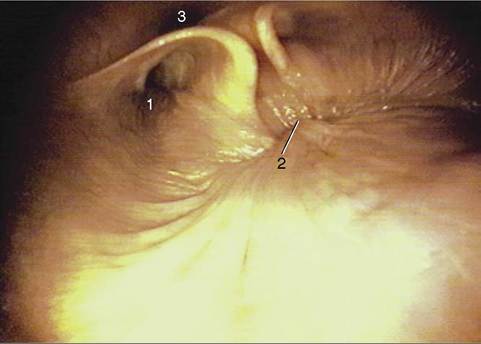
Figure 18-27 Endoscopic view of the caudal part of equine nasopharynx (foal). 1, Entrance to auditory tube; 2, closure of the intrapharyngeal ostium between the nasopharynges and laryngopharynges (during swallowing); 3, cartilage flange supporting the auditory tube.
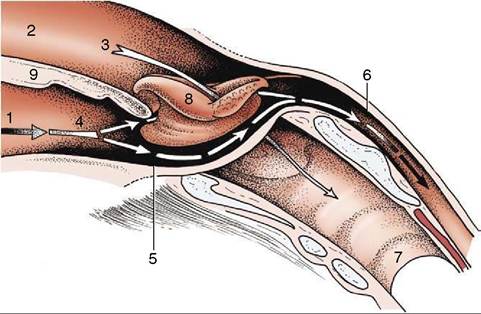
Figure 18-28 The communications of the pharynx, rostrally with the oral and nasal cavities, caudally with the esophagus; schematic. The broken arrows mark the digestive pathway; the unbroken arrow marks the respiratory pathway.
1, Oral cavity; 2, nasal cavity; 3, nasopharynx; 4, oropharynx; 5, laryn- gopharynx; 6, esophagus; 7, trachea; 8, epiglottis, laryngeal entrance; 9, soft palate.tympanic membrane. The maneuver, which can be observed endoscopically, involves the flap swinging medially while the soft palate rises and momentarily narrows the lumen of the nasopharynx (Figure 18-27). The flap can also be elevated passively, and it is a relatively simple matter to introduce an endoscope to examine, or a catheter to drain or irrigate, the guttural pouch. The entrance to the tube lies in the transverse plane of the lateral angle of the eye, which is a useful external guide to its position. An indication of the progress of the instrument through the ventral meatus and nasopharynx is provided by the resistance encountered; the firm support offered to its tip by the vertical lamina of the pterygoid bone is lost only a short distance rostral to the opening. Advancement of the instrument to this level generally provokes a swallowing movement when deflection of the cartilage flap facilitates entry to the pouch. When the procedure is performed blind, the absence of resistance to deeper penetration indicates that the pharyngotubal opening has been successfully passed.
The lower compartment of the pharynx is divided between the oropharynx and the laryngopharynx (Figure 18-28/4,5). The narrow oropharynx extends
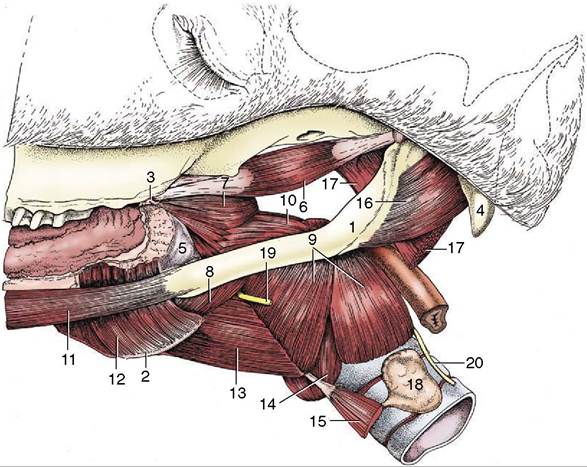
Figure 18-29 Muscles of the pharynx, soft palate, and hyoid apparatus. 1, Stylohyoid; 2, thyrohyoid; 3, hamulus of pterygoid bone; 4, paracondylar process; 5, buccopharyngeal fascia; 6, tensor veli palatini; 7, rostral pharyngeal constrictor; 8, middle pharyngeal constrictor; 9, caudal pharyngeal constrictor (thyropharyngeus and cricopharyngeus); 10, stylopharyngeus caudalis; 11, styloglossus; 12, hyoglossus; 13, thyrohyoideus; 14, cricothyroideus; 15, sternothyroideus; 16, occipitohyoideus; 17, longus capitis (stump); 18, thyroid gland; 19, cranial laryngeal nerve; 20, caudal (recurrent) laryngeal nerve.
between the attachment of the palatoglossal arches to the tongue and the epiglottis; its lateral walls and floor contain much diffuse tonsillar tissue, including the long palatine tonsil (see Figure 3-25). The Iaryngopharynx is largely occupied by the projection of the larynx, and its floor is reduced to the narrow flanking piriform recesses. The laryngopharynx narrows abruptly to the origin of the esophagus.
The structure and musculature follow the common pattern (Figure 18-29). Difficulties in swallowing sometimes arise from malfunction of palatine and pharyngeal muscles. The cause frequently lies in involvement of the relevant glossopharyngeal and vagus nerves in infections of the guttural pouch; because the nerves run together, they are equally susceptible (Figure 18-30/7,14).
THE GUTTURAL POUCH
A diverticulum of the auditory tube, the guttural pouch, is found in the horse and other Perissodactyla (Figure 18-31/9). It is formed by the escape of the mucosal lining of the tube through a ventral slit between medial and lateral supporting cartilages and attains a capacity of some 300 to 500 mL. It lies between the base of the skull and atlas dorsally and the pharynx and commencement of the esophagus ventrally; it is covered laterally by the pterygoid muscles and parotid and mandibular glands. Medially, the dorsal parts of the right and left sacs are separated by the ventral straight muscles of the head, but below this they meet, forming a thin median septum. The floor lies mainly on the pharynx but also covers and is molded to the stylohyoid, which raises a ridge that incompletely divides medial and lateral compartments (Figure 18-32).
More detailed relations include several cranial nerves and arteries that lie directly against the pouch as they pass to and from foramina in the caudal part of the skull. The glossopharyngeal, vagus, accessory, and hypoglossal nerves; the continuation of the sympathetic trunk beyond the cranial cervical ganglion; and the internal carotid artery are closely related for a stretch and together raise a mucosal fold that indents the medial compartment from behind; this is a conspicuous feature when the interior of the pouch is viewed endoscopically (Figure 18-33/4). The facial nerve has a more limited contact with the dorsal part of the pouch.
The large external carotid artery passes ventral to the medial compartment before crossing the lateral and then rostral walls of the lateral compartment (Figure 18-33/d) in its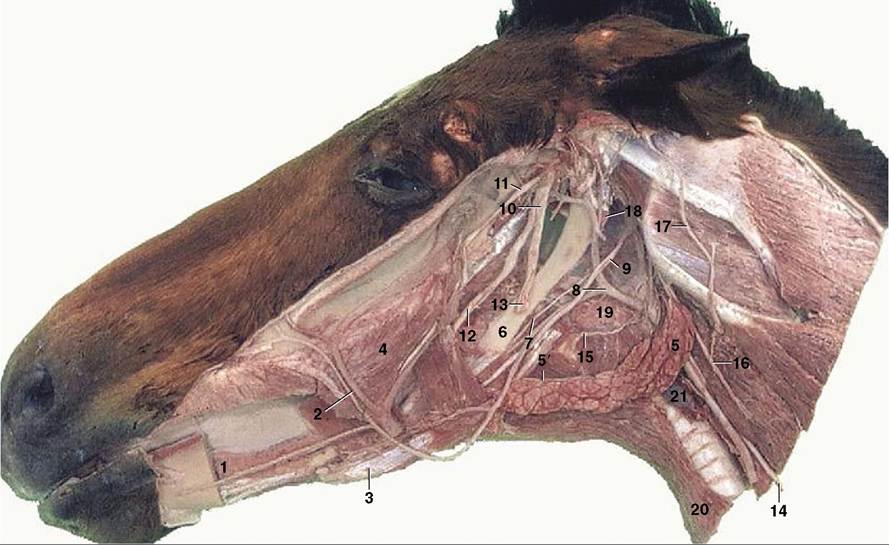
Figure 18-30 Deep dissection of the head. The mandible and masticatory muscles have been removed. 1, Sublingual gland; 2, facial artery and vein; 3, rostral belly of digastricus; 4, buccinator; 5, mandibular gland; 5', mandibular duct; 6, stylohyoid; 7, glossopharyngeal nerve; 8, linguofacial artery; 9, hypoglossal nerve; 10, mandibular nerve; 11, masseteric nerve; 12, lingual nerve; 13, inferior alveolar nerve, cut where it enters the mandibular foramen; 14, vagus and sympathetic trunk; 15, cranial laryngeal nerve; 16, dorsal branch of spinal accessory nerve; 17, great auricular nerve; 18, guttural pouch; 19, medial retropharyngeal lymph nodes; 20, sternohyoideus; 21, thyroid gland.
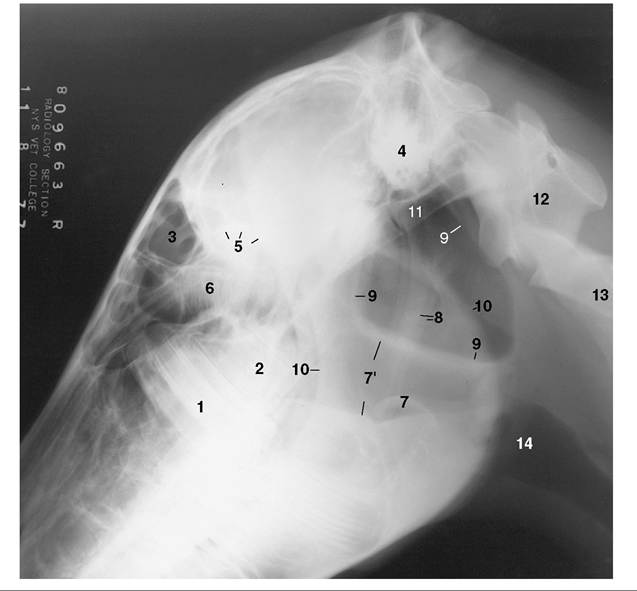
Figure 18-31 Lateral radiographic view of the head to show the position of the guttural pouches (9) in a horse 1∕2 years old (estimated). 1, M1; 2, unerupted M2; 3, frontal sinus; 4, petrous temporal bone; 5, caudal border of orbit; 6, ethmoid labyrinth; 7, epiglottis; 7, nasopharynx; 8, stylohyoid bones; 9, borders of guttural pouches; 10, rostral and caudal borders of mandible; 11, base of skull; 12, atlas; 13, axis; 14, larynx.
approach (as the maxillary artery) to the alar canal. The pouch also directly covers the temporohyoid joint.
The mucous secretion of the lining normally drains into the pharynx through the pharyngotubal opening (Figure 18-11Zstrident sound emitted at inspiration, is a common manifestation of this in high- performance horses. In its severe form it is characterized by unilateral adduction of the arytenoid cartilage and vocal cord; in less severe forms it is identified by limited abduction of these structures.
The abnormal sound is produced by passive vibration of a lax vocal cord in the airstream. The cause lies in dysfunction, proceeding to atrophy, of part of the intrinsic laryngeal musculature. For reasons that are unclear, the pathology is almost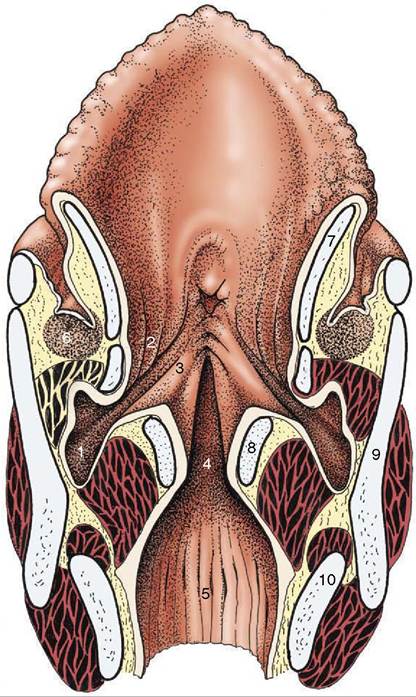
Figure 18-35 Dorsal section of the larynx. 1, Laryngeal ventricle; 2, vestibular fold with ventricularis; 3, vocal fold with vocalis; 4, glottic cleft; 5, infraglottic cavity; 6, caudal end of palatine tonsil; 7, epiglottic cartilage; 8, arytenoid cartilage; 9, thyroid cartilage; 10, cricoid cartilage.
always limited to the left side and is initially manifested in the cricoarytenoideus dorsalis, the abductor muscle of the cartilage, before possibly proceeding to affect other muscles with adductor actions.
The term roaring is applied to a strident sound produced at inspiration in affected animals. The sound is caused by the flow of air passively vibrating a lax, adducted vocal fold (Figure 18-26, A-B). The laxity results from paralysis of certain laryngeal muscles. A polyneuropathy is considered to be the underlying cause. The paralysis is almost always limited to the left side, and though it initially affects the cricoarytenoideus dorsalis—abductor of the arytenoid cartilage and vocal fold (see Figure 4-15/5)—other muscles may later become involved.
The asymmetry in incidence directs attention to differences in the courses and relations of the right and left recurrent laryngeal nerves. The left nerve loops around the aortic arch and has a closer relationship to tracheobronchial and other lymph nodes within the chest. Because the condition often follows a respiratory infection, the relationship to the nodes is perhaps the more relevant; it is not a complete explanation, however, as laryngeal muscular atrophy has been recognized in unborn foals. Wastage of the cricoarytenoideus dorsalis alters the contours of the larynx in a manner that can be appreciated on external palpation; it hollows the space above the arytenoid cartilage, which makes the muscular process of that cartilage more prominent.
One of the operations for the relief of roaring is the reinforcement of the wasted dorsal cricoarytenoideus muscle by a suture tightened to fix the arytenoid cartilage in permanent abduction. An older alternative was the eversion and excision of the lateral laryngeal ventricle in the expectation that the resulting scar tissue would bind this cartilage to the thyroid cartilage. Both operations result in tightening the vocal fold and widening the glottic cleft. Neither operation effects a cure of the condition, which has human and canine parallels. Other defects, such as partial collapse of an arytenoepi- glottic fold or prolapse of the cricotracheal membrane, may also cause obstruction. It is noteworthy that multiple defects, possibly involving nasal, pharyngeal, and laryngeal levels, are quite common. Recently a syndrome of deformaties that may afflict the derivates of the fourth branchial arch has been described. This 4-BAD syndrome may also result in multiple anomalies of the pharynx, larynx, and upper esophagus.