» The Stifle Joint and Leg (see also pp. 83-85 and 8990.)
The stifle joint is flexed in the standing posture. Although it is more fully extended in certain phases of locomotion, the femur and tibia are never brought into line, and the caudal angle of the joint does not open beyond 150 degrees or so in dogs; considerably greater extension is permitted in the cat.
Some lateral or medial angulation of the joint may often be observed when the limb is viewed from the front or behind. In the "bowlegged" version common in certain toy breeds, the pull of the quadriceps does not coincide with the axis of the femoral trochlea and there is a tendency to medial luxation of the patella. The luxation, which may be intermittent or permanent, causes the limb to be carried and, if left uncorrected, leads to deformity of other parts. The trochlea can be brought into alignment with the axis of the tibia by translation of the tibial tuberosity. The same procedure can be used to correct any medial or lateral patellar luxation, whatever its origin.Palpation of the stifle joint reveals the following features of the skeleton: the patella; the ridges of the trochlea and the outer surfaces of the condyles of the femur; the sesamoid bones within the origin of the gastrocnemius; the head of the fibula; the edge of the lateral condyle adjacent to the fibula; the tuberosity; the extensor groove; and the medial surface of the tibia. The single patellar ligament and the medial and lateral collateral ligaments may also be distinguished; however, the femoropatellar ligaments cannot be distinguished because they are overlain by the aponeuroses of the sartorius and semimembranosus on the medial side and by that of the biceps laterally.
The most distinctive internal feature of the joint is the free communication of the various synovial compartments, which ensures that a single injection will reach all parts of the cavity.
The most convenient entry is from the lateral side, caudal to the thick pad of fat interposed between the patellar ligament (and adjoining retinaculum) and the synovial membrane. The lateral femorotibial joint has two pouches: one is under the tendon of the long digital extensor muscle at its origin from the extensor fossa, and the other invests the tendon of origin of the popliteal muscle, which contains a sesamoid bone close to the lateral tibial condyle.The cruciate ligaments are set well back (see Fig. 2.63/15 and 16) and assist the collateral ligaments in opposing rotation and medial or lateral deviation of the leg; they are most susceptible to injury when tautened. The cranial cruciate ligament, named for the relative position of its tibial attachment (see Fig. 2.63/16), is therefore at greatest risk during overextension of the joint, and its rupture allows abnormally free forward displacement of the tibia in relation to the femur (the "cranial drawer" sign). A short cranial drawer movement (1-3 mm) brought to an abrupt stop is normal in young dogs. A deterioration in the strength of this ligament is correlated with age and is due to fiber bundle disruption and metaplastic cellular changes; the central part of the ligament is most affected. The changes are more pronounced and appear at earlier ages in larger dogs.
Cruciate Ligaments: The cruciate ligaments also have nerve endings and receptors for sensing mechanical forces. These nerves and receptors provide proprioceptive feedbacks to check the abnormal or excessive flexion or extension of the joint. Rupture of the cruciate ligaments is common in older dogs, and that may suggest an underlying degenerative process. Of course, mechanical trauma also is a major cause of rupture of the cruciate ligaments.

FIG. 17.4 (A) Lateral and (B) craniocaudal radiographic views of canine stifles. (D) Lateral radiographic view of feline stifles.
(C) Frontal (M, medial; L, lateral) and (E) axial 4-mm-thick T1-weighted spin-echo magnetic resonance slices of the left canine stifle. 1, Femur; 1', extensor fossa; 1", lateral condyle; 1'", intercondylar fossa; 2, patella; 2', patellar ligament; 3, sesamoid bones in gastrocnemius; 3', popliteal sesamoid bone; 4, tibia; 4', tibial tuberosity; 4", tibial crest; 5, fibula; 6, femoropatellar joint cavity; 6', infrapatellar fat; 7 and 7', medial and lateral menisci, respectively; 8 and 8', cranial and caudal cruciate ligaments, respectively; 9, gastrocnemius; 10, popliteal lymph nodes.The caudal cruciate ligament is at greatest risk in the flexed position of the joint, and its rupture allows excessive caudal displacement of the tibia (the "caudal drawer" sign). Various surgical techniques for the restoration or replacement of the cranial and caudal ligaments use fascial or artificial substitutes. The lateral collateral ligament can be used as a substitute for the cranial cruciate ligament after transposition of the head of the fibula cranially.
The menisci, joined cranially (also caudally, in the cat) by an intermeniscal ligament, provide additional restraints and are also prone to injury. They are most vulnerable when torsion is imposed on a limb in which the stifle is extended and the foot fixed — a combination of circumstances found when an abrupt change in direction is attempted by a dog traveling at speed. Most often a meniscal tear is found in combination with a rupture of the cranial cruciate ligament.
The meniscal horns are more richly supplied with blood vessels and nerves in comparison with the more central parts. The involved portion, or sometimes the whole meniscus, is often removed after injury; an imperfect replacement may ultimately be formed from granulation tissue produced by the capsule at the site of the original attachment. The medial meniscus has an additional restraint imposed by a connection with the medial femorotibial ligament by way of the joint capsule.
This may limit the range of its excursions compared with those of the lateral meniscus and may thus be a factor in determining the incidence of injuries.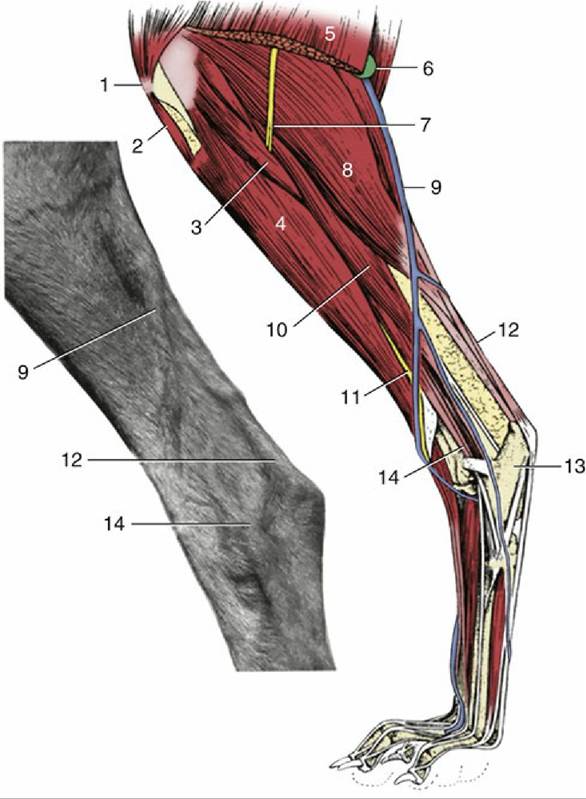
FIG. 17.5 Left canine hindlimb; the inset shows the actual appearance of the lateral saphenous vein (9); lateral view. 1, Patella; 2, patellar ligament; 3, peroneus longus; 4, tibialis cranialis; 5, biceps femoris; 6, popliteal lymph node; 7, common peroneal nerve; 8, lateral head of gastrocnemius; 9, lateral saphenous vein; 10, deep digital flexor; 11, superficial peroneal nerve; 12, calcanean tendon; 13, calcaneus; 14, peroneus longus tendon.
Both lateral and craniocaudal radiographic projections are commonly used in the diagnosis of stifle injuries (Fig. 17.4). In the craniocaudal view the patella is superimposed on the distal end of the femur, where it is flanked by the ridges of the trochlea, which appear as thin radiodense lines. The tibial condyles are relatively flat because they are not separated by the conspicuous intercondyloid tubercles found in the larger species. The head of the fibula falls short of the extremity of the tibia. In the lateral view the femoral and tibial condyles are seen to have only limited, rather caudal contact and the joint appears unstable because the menisci that maintain its congruence are not revealed. The patellar ligament, the most prominent soft tissue shadow, runs at some distance from the femur, and the space behind it is occupied by the infrapatellar fat cushion. Displacement of this fat may be evident in radiographs and may suggest either thickening of the capsule or effusion into the joint cavity. The same view best depicts the associated sesamoid bones. The pair within the heads of the gastrocnemius are large and well defined (Fig. 17.4/3). They articulate with small facets on the upper parts of the corresponding femoral condyles. The sesamoid within the popliteus tendon is smaller, less sharply outlined, and occasionally duplicated; it is related to the margin of the tibia (Fig.
17.4/3'). A relatively radiolucent area between the trochlea and lateral femoral condyle indicates the position of the extensor fossa (Fig. 17.4/1') and has occasionally been mistaken for an osteolytic lesion.In dogs, both the distal femoral and proximal tibial epiphyses generally fuse with their respective shafts between the 6th and 12th months. The wide and irregular cartilage line between the center for the tibial tuberosity and the shaft, which fuse between the 8th and 10th months, simulates avulsion of the tuberosity. The onset and completion of these fusions are somewhat delayed in cats.
Few features of the leg require further comment. The subcutaneous surface of the tibia divides the cranial and caudal crural muscles medially, while the fibula makes the same division laterally (Fig. 17.6). In lean dogs the fibula may be palpated along its length, but in fatter and particularly well-muscled animals only the head and the distal half of the shaft may be felt with certainty. The superficial flexor and gastrocnemius components of the common calcanean tendon may be identified separately, distal to the belly of the latter. The lateral saphenous vein is a very conspicuous surface feature of the lateral aspect (Fig. 17.5/9). It runs proximocaudally over the lower part of the leg before following the gastrocnemius on the caudal border to join the femoral vein within the popliteal fossa. The proximal part of the vein is relatively fixed and straight, making it more suitable for intravenous injections. The distal part undulates, dipping between the caudal crural muscles and the common calcanean tendon.
The vascularization of the leg and more distal parts depends on the cranial tibial and saphenous arteries because the caudal tibial artery is quite insignificant (Fig. 17.3/3 and 4). The cranial tibial artery continues the popliteal artery, which runs deep to the popliteal muscle on the caudal aspect of the stifle. The artery then passes between the tibia and fibula in the proximal part of the leg before penetrating the dorsal muscles.
It reappears toward the hock and then follows the long extensor tendon across the joint into the paw. The saphenous artery, which broadly serves the territory assigned to the caudal tibial artery in many species, crosses the medial aspect of the stifle before dividing into cranial and caudal branches. The cranial branch (Fig. 17.3/6) remains superficial and continues into the paw, where it supplements the cranial tibial artery in supplying dorsal structures; the caudal branch (Fig. 17.3/5) accompanies the tibial nerve and, after supplying caudal crural muscles, follows the flexor tendons into the plantar aspect of the paw.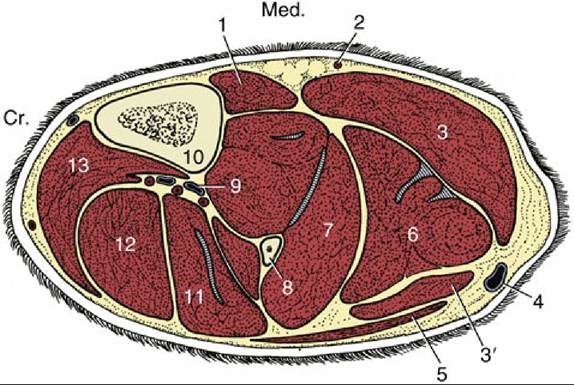
FIG. 17.6 Transverse section of the canine left leg. Cr., Cranial; Med., medial. 1, Popliteus; 2, saphenous artery; 3 and 3', medial and lateral heads of the gastrocnemius, respectively; 4, lateral saphenous vein; 5, biceps femoris; 6, superficial digital flexor; 7, deep digital flexor; 8, fibula; 9, cranial tibial vessels; 10, tibia; 11, peroneus longus; 12, long digital extensor; 13, tibialis cranialis.