» The Thoracic Wall and Pleura (see also pp. 38-39, 4547, and 148-149)
The dog generally has 13 rib pairs of which 9 are sternal. Asymmetry of number and the presence of 12 or 14 pairs are both occasionally found. Although the first three to four ribs are almost vertical, the remaining slope increasingly caudoventrally (see Fig.
2.1). The ribs are relatively narrow, resulting in wide intercostal spaces, an advantage in thoracic surgery. The costal cartilages at first continue the direction of the bony ribs but then bend forward, almost at right angles (see Fig. 13.5), to form the rib "knees." The cartilages of the sternal ribs form synovial articulations with the sternum, which allow expansion of the thorax when the ribs are carried cranially in the "buckethandle" movement. The cartilages of the four asternal ribs join to form the costal arch, which is easily palpated and may be followed to the vicinity of the xyphoid cartilage (Fig. 13.7/5). The slender, cylindrical sternebrae are slightly thickened at their extremities where the costal cartilages attach. Only a thin layer of compact bone encloses the spongy interior of sternebrae; this characteristic, combined with their superficial position, makes them ideal for bone marrow biopsy.
FIG. 13.2 Broad, barrel-shaped thorax of the Pug.
FIG. 13.3
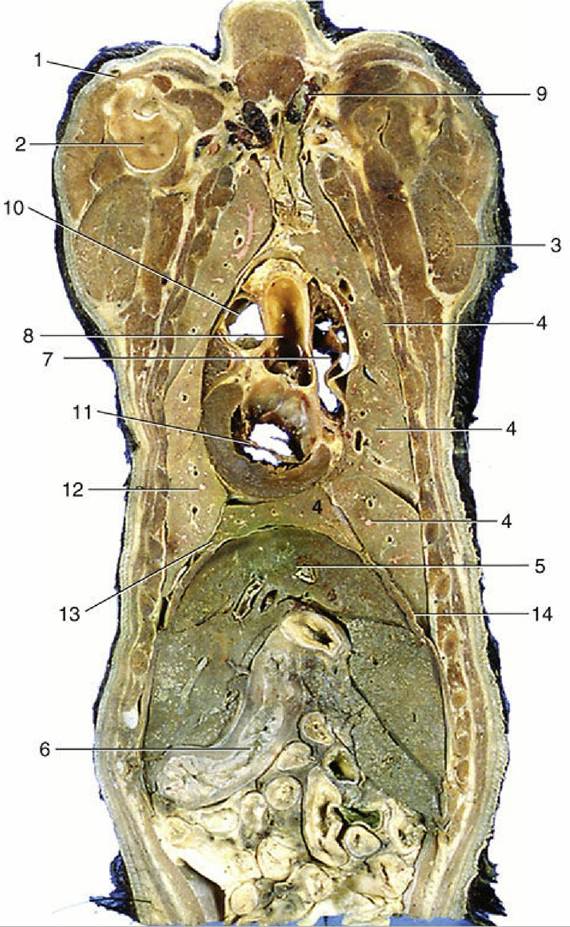
Dorsal section of the canine trunk level with the base of the heart, dorsal view. 1, Cephalic
vein; 2, proximal end of humerus; 3, triceps; 4, cranial, middle, caudal, and accessory lobes of the right
lung; 5, liver; 6, stomach; 7, right atrium; 8, aortic arch; 9, cranial vena cava; 10, pulmonary valve; 11, left
atrioventricular valve; 12, divided cranial and caudal lobes of the left lung; 13, caudal mediastinum; 14,
diaphragm.
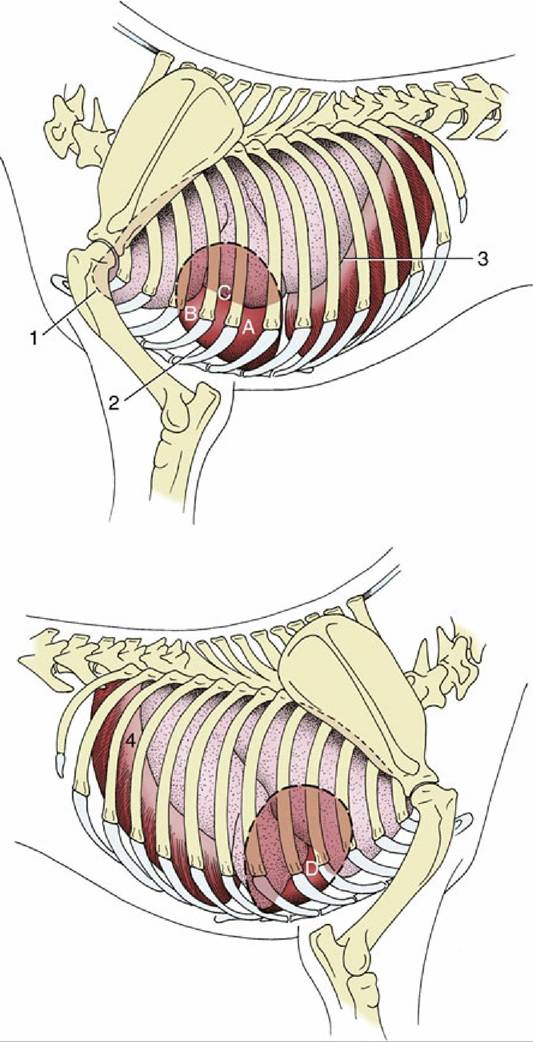
FIG.
13.4 Left and right surface projections of the canine heart and lungs. Circled letters on the heart: puncta maxima of left atrioventricular valve (A), pulmonary valve (B), aortic valve (C), and right atrioventricular valve (D). 1, Apex of left lung (broken line) in cupula pleurae; 2, heart; 3, basal border of lung; 4, diaphragm.
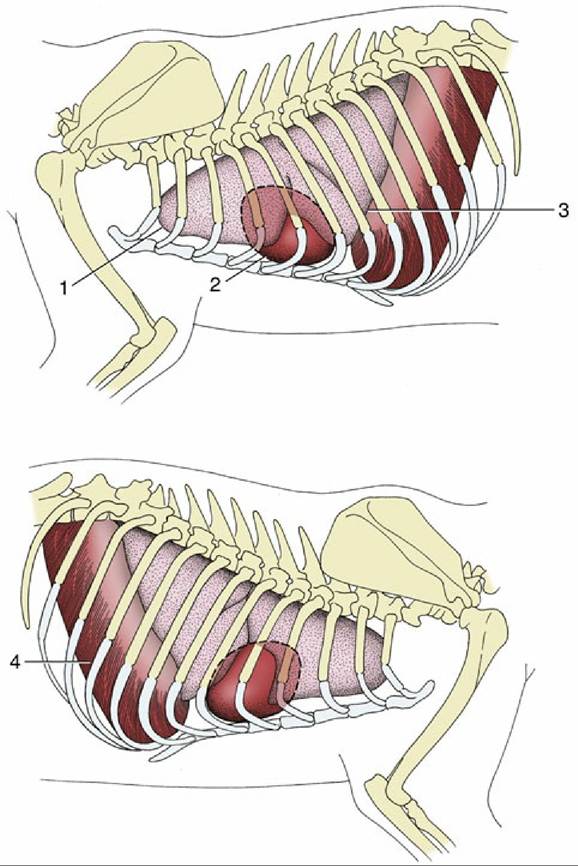
FIG. 13.5 Left (top) and right (bottom) surface projections of the feline heart and lungs. 1, Apex of left lung; 2, heart; 3, basal border of lung; 4, diaphragm.

FIG. 13.6 Notice the attachment of the external abdominal oblique muscle on the ribs.
The principal intercostal vessels and nerves run caudomedially to the ribs, under the endothoracic fascia. Additional vessels from the internal thoracic trunks follow the cranial borders of the ribs in the ventral parts of the spaces (Fig. 13.8). These locations must be borne in mind when incision or puncture is contemplated. It is helpful to know that the boundary between the scalenus and external abdominal oblique muscles is the fifth intercostal space. The ribs are so much more easily displaced cranially than caudally that a more favorable exposure of the "target" region for clinical procedure may be gained by opening the space immediately caudal to the one that initially seemed most appropriate.
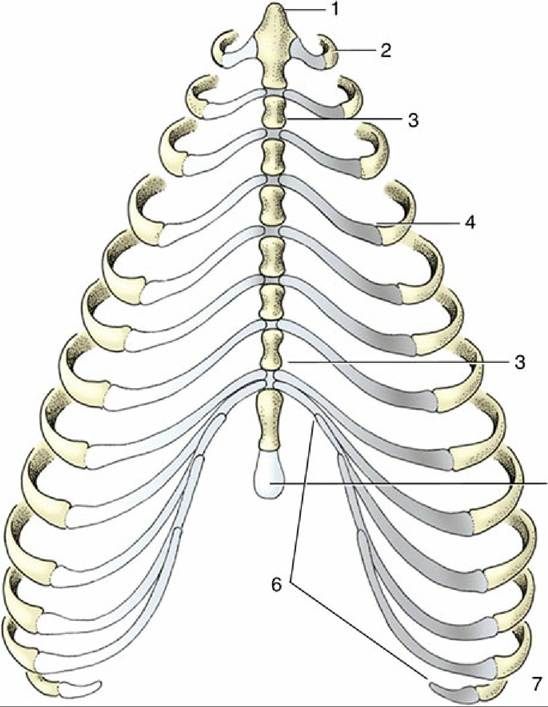
FIG. 13.7 Canine sternum and costal cartilages, ventral view. 1, Manubrium; 2, first rib; 3, sternebra; 4, costochondral junction; 5, xiphoid cartilage; 6, costal arch; 7, floating rib.
The diaphragm arises by right and left crura from the first few lumbar vertebrae and attaches to the medial surfaces of the ribs close to the costal arches and to the sternum. Its strong curvature brings its most cranial point to the level of the 6th or 7th rib.
The small, triangular tendinous center transmits the caudal vena cava a little to the right of the median plane. The openings for the esophagus and aorta lie in the fleshy lumbar part, and the former is opposite the upper palpable part of the 10th rib (Fig. 13.9). In lateral radiographs the strongly convex ventral part of the diaphragm presents a simple border that is continued dorsally by the paired outlines of the cupulae (Fig. 13.10A/4); the more cranial outline of this double image is provided by the cupula on the "lower" side of a laterally recumbent animal, which is the side subjected to greater forward pressure from the abdominal viscera. The correct identification of the twin elevations is further provided by the gas bubble usually found in the gastric fundus, which is of course located on the left side. The doubling of the outline is less distinct in cats, in which the lighter abdominal organs exert possibly less pressure. Diaphragmatic hernia is the entry of abdominal viscera into the thoracic cavity. It occurs when the diaphragm is torn by a sudden increase in abdominal pressure, which is commonly produced by compression in traffic accidents.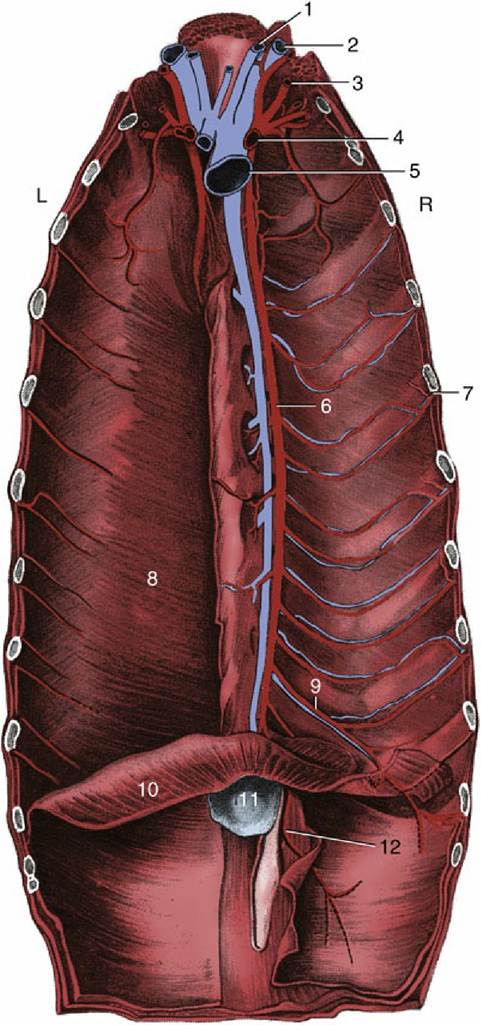
FIG. 13.8 The vessels on the floor of the canine thorax; the transversus thoracis muscle has been removed on the right. 1, Internal jugular vein; 2, external jugular vein; 3, vertebral artery; 4, right subclavian artery; 5, cranial vena cava; 6, internal thoracic artery; 7, intercostal artery; 8, transversus thoracis muscle; 9, musculophrenic artery; 10, diaphragm; 11, xiphoid cartilage; 12, cranial epigastric artery; L, left; R, right.
At rest, ventilation depends principally on the diaphragm. However, increased respiratory demand engages other muscles as well. Although some or all of the external intercostal, sternocephalic, ventral serratus, and scalenus may be used to assist at inspiration, the internal intercostal and abdominal muscles may help at expiration.
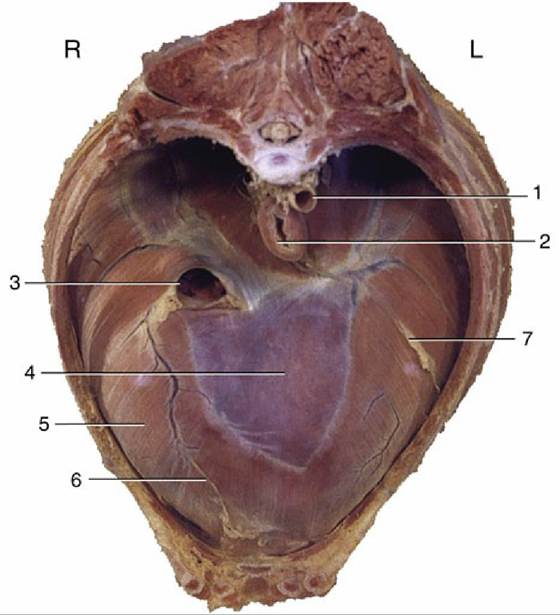
FIG. 13.9 Cranial view of the canine diaphragm. 1, Aorta; 2, esophagus; 3, caudal vena cava; 4, tendinous center; 5, sternal and costal parts of diaphragm; 6, attachment of plica venae cavae; 7, attachment of caudal mediastinum; L, left; R, right.
The most important clinical features of pleural cavities are the cupulae cranially, the caudal reflection of the costal pleura onto the diaphragm, and the presence and extents of the costomediastinal and costodiaphragmatic recesses. Although the cupulae (see Fig. 13.5) project only slightly in front of the first ribs in the dog, they are still susceptible to puncture wounds that appear to be confined to the base of the neck; the resulting entry of air into the pleural cavity (pneumothorax) causes uncoupling of the lung from the thoracic wall and its collapse.
The line of pleural reflection is at the junction between costal and diaphragmatic pleura, and it defines the caudal extent of the pleural cavity. The line runs from the sternum along the 8th costal cartilage, crosses the middle of the 9th cartilage, and then proceeds in a curve that intersects the 11th costochondral junction to reach the dorsal end of the last rib. The two recesses are of course never fully exploited by the lungs. Fluid may be collected through the ventral third of any of the 4th to 7th intercostal spaces of a dog standing or restrained in sternal recumbency. In cases of pneumothorax, air may be aspirated at the dorsal part of the 7th or 8th space of dogs similarly placed. The 8th space is optimal for this purpose in the cat.
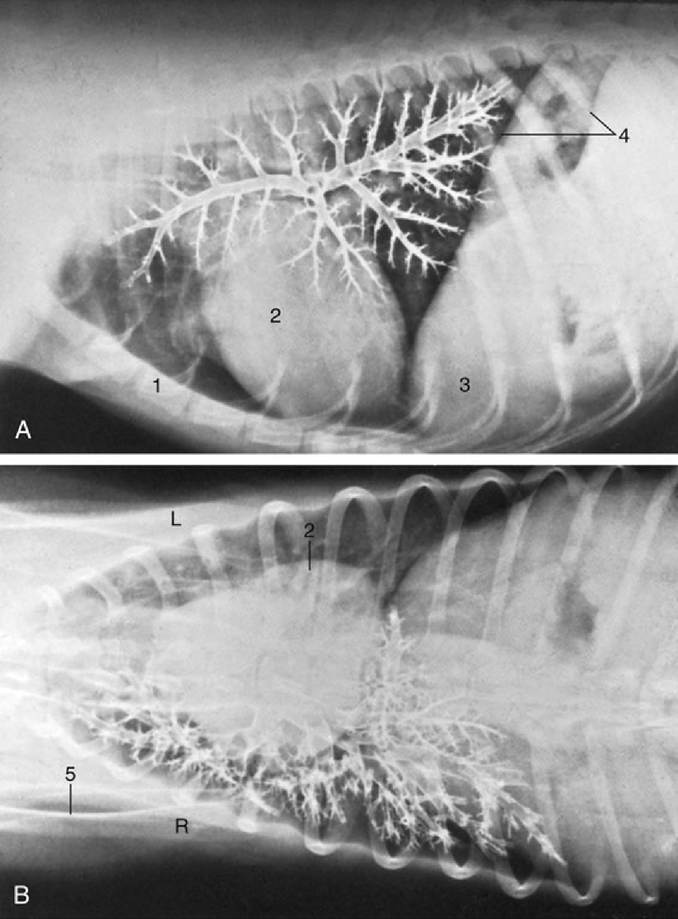
FIG. 13.10 (A) Lateral and (B) ventrodorsal bronchograms of the right canine lung. 1, Sternum; 2, heart;
3, liver behind diaphragm; 4, paired shadows of the cranial extent of the diaphragm; 5, scapula; L, left; R, right.